

How to Stop Your Puppy from Whining: Expert Explains

How do you stop a puppy from whining?
A pet behavior expert explains how you can stop your puppy from whining. (more…)

Pushing a Stroller vs. Holding onto a Treadmill: the Difference

What’s the difference between holding onto a treadmill while walking and pushing a stroller?
Are these two activities one and the same? (more…)


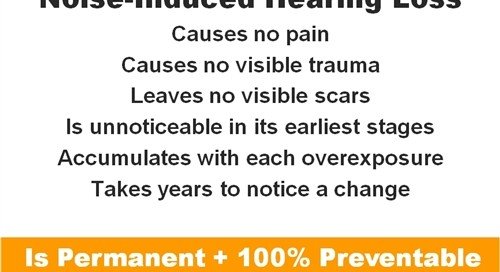
Hearing Loss Prevention Tips for Everyday Life

Here are things you can do in everyday life that will help prevent hearing loss.
“Best way to protect your ears is to first be aware of the guidelines established by the National Institute for Occupational Safety and Health (NIOSH) regarding exposure levels to loud noise,” says Rivka Strom, AuD, CCC-A, chief audiologist at Central Hearing LLC in NY.
Strom adds, “Once you realize what unsafe levels are, try to avoid those situations where there is potential harm or keep a few packs of earplugs in your bag.”
It’s the little day-to-day noises that can contribute significantly to gradual hearing loss over time.
Every Day Noises that Can Contribute to Hearing Loss
Kitchen Work. Wearing earplugs during the use of blenders, juicers, coffee grinders and other loud items would be a very smart idea.
- How much hearing loss will years and years of using a blender, juicer and coffee grinder cause?
- These machines are LOUD.
-
“Some kitchen appliances can absolutely cause NIHL after many exposures,” says Strom.
Entertainment. “Turning up the volume” for thrills will contribute to NIHL over time. Can you hear your TV dialogue just fine at a volume level of 10 (or whatever your volume indicator says)?
Then don’t go to 14. Stay at 10. During scenes of muddled speech, go to 11 or 12.
But to keep it higher just for the sake of “I like it loud” is setting you up for hearing loss.
“Listening to music at high volumes through earbuds is one of the more damaging behaviors in which people continue to engage, despite warnings,” says Strom.
Windows. Do you slam your windows shut? Repeated exposures of the loud noise that this makes is not good for hearing health.
In Public. Strom explains, “It’s a good idea to keep a pair of earplugs in your bag or pocket when you leave the house, in case you find yourself in a situation where ambient noise exceeds your comfort level (e.g., near a construction site, walking by heavy traffic sounds, attending a concert or party, going to the dentist).”
If you forgot your earplugs, then use your fingers and don’t mind what strangers might think.
“In 2016, the Center for Disease Control and Prevention began initiatives to raise awareness about the risk for permanent hearing damage attributable to non-occupational noise exposures,” says Strom.
“They published prevalence numbers close to 24% for adults with noise induced hearing loss.
“Again, these numbers are for non-occupational noise exposure, so that includes all those times you are exposed to high level noise when you are having fun and living life and may not even realize that the music of your car, or your child’s loud toy (and yes, loud toys too can get to unsafe levels!!) or blow drying your hair at max setting can harm you without protection.”
The Gym. Few people at gyms wear earplugs. Yet gyms are very loud.
- Booming speakers all over the ceiling on the main floor.
- Many cardio machines going at once.
- People banging large metal plates.
- Thundering music in group fitness classes.
An audiologist can fit you for custom made earplugs, which are superior to any that you can buy online or at a drug store.
If you’re worried what people will think of you protecting your ears from hearing loss, this inconvenience pales in comparison to the expense of hearing aids, which usually comes after years of denying you have hearing loss even though everyone is just sick of having to talk loudly and slowly to you all the time. Think about it.

And did you know that often, a person who wears hearing aids must undergo repeated testing to get things right?
I should know; I have accompanied my noise-induced hearing impaired father on countless trips to the audiologist over the past few years. Each testing lasts about an hour!

Dr. Strom is a member of the American Speech Language and Hearing Association and has received several awards including Brooklyn College’s Excellence In Audiology Award.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ANDRANIK HAKOBYAN

Will Colon Cancer Surgery Interfere with the Ability to Eat?

Will colon cancer surgery affect your ability to eat?
In colon cancer surgery, part or all of the large colon may be removed, and this information invariably makes many people wonder if surgery for this cancer will impair the ability to eat.
Surgry for colon cancer “almost never” interferes, says Whitney Jones, MD, a national expert and frequent speaker on early-age onset colon cancer prevention, and Founder, Colon Cancer Prevention Project.
Dr. Jones explains, “In fact, unless there are other circumstances — severe concurrent medical problems, coexisting nutritional issues, complications, ongoing battles with spread or metastatic colon cancer — the answer is never.”
Thus, if you suspect you might have this disease, and have been playing through your mind all sorts of scenarios depicting the aftermath that this disease will create, and some of these images are of you getting fed through a feeding tube at dinnertime – you can let go of these images and breathe a sigh of relief that colon cancer will not destroy your ability to enjoy your favorite foods.
Dr. Jones also explains, “Total removal of the colon with or without iliostomy usually causes only diarrhea, since the colon’s primary functions are waste transport, storage and water absorption.
“Some patients who have an ileal resection can have severe diarrhea, malabsorb bile salts and vitamin B12, sometimes with a failure to thrive syndrome.”
If you don’t have colon cancer but have wondered if surgery for this disease impairs the patient’s ability to eat, here’s something you should spend more time thinking about: what you are currently eating, as it relates to possibly increasing the risk of developing cancer of the colon.
A diet high in processed meat may increase the risk.
So may a diet low in fiber.
A diet that is high in fiber promotes faster transport time of food material through the GI tract.
The longer food just sits in the GI tract, the more likely that any toxins in the food will adversely affect colon health, as well as get absorbed into your system.
And there are plenty of toxins in today’s modern food fare, including pesticides, antibiotics, synthetic flavorings, chemical colorings and all sorts of preservatives — not to mention trans fats and white sugar.
A high fiber diet will contribute to having a “cleaner gut,” and this can lower the odds of developing colon cancer.
 Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

How Effective Is Housework for Significant Weight Loss?

Okay, so housework burns calories. So does sleeping. You’re alive, you burn calories, but housework will not lead to significant or even moderate weight loss.
In fact, being that you’ve already been doing housework all along, it’s not going to slim your body and make you fitter.
It’s true that cleaning house requires energy, but it is not an effective strategy for getting and staying physically fit and healthy.
While some fitness experts (and even medical professionals) like to offer the “do housework” as an exercise alternative, obese women who employ such a strategy will continue to fail in meeting their fitness and health goals, unless they engage in other calorie-burning and structured exercise activities that amount to a real workout.
What about extra housework?
Extra housework can actually be a stepping stone to getting a very morbidly heavy individual off the sofa or even out of bed, as it creates more movement than they’re normally used to, and will get the blood circulating.
But it’s a small stepping stone, and that’s all.
Maintaining a clean house is an activity that all individuals should engage in anyway. It’s a constant in an equation.
Living in a dirty house can add to depression, heightened stress and low-self-esteem, which can lead to increased eating and lack of motivation for structured workouts or athletic activities, which leads to even more excess weight added to one’s body.
The smart, effective approach is to keep your home cleaned and then hit the gym (or home workout devices) for the muscle toning and aerobic workouts that will bring you a transformed physique.

Depositphotos.com
Cleaning house cannot possibly duplicate the cardiorespiratory effects that structured cardiovascular exercise, especially that of interval training, can.
Do not believe this for a single moment.
Interval training is when you alternate brief high effort exertion with casual pacing.
Cleaning house is a good habit to keep, but not for attaining fat loss, physical fitness or good health.
A very overweight individual who’s serious about getting healthy, physically fit and losing bodyfat needs to think beyond the vacuum and washcloths, and embrace structured strength training and cardio exercise.
Pictured below are examples of exercises that will really help you lose weight.

Shutterstock/Aleksey Boyko

Shutterstock/Reshetnikov_art


Shutterstock/Reshetnikov_art


Shutterstock/New Africa

Shutterstock/gpointstudio
So how do you get started? It’s as simple as joining a gym or purchasing some basic exercise equipment for home workouts.
A few pairs of dumbbells, some tension bands, a kettlebell and a heavy ball are all you need to get started if you don’t plan on joining a gym.
However, you’ll want to see if you can come up with any compelling reasons for why you can’t get a gym membership, being that there are options for all budgets.
A gym membership will motivate you more to stick to a workout, and will offer a ton more options as far as different equipment, dumbbells and kettlebells in all weights, plus a variety of group fitness classes and different kinds of cardio equipment.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Nomad_Soul
Climber’s Home Treatment for Finger Injury

Learn a simple treatment for healing finger injuries from climbing. (more…)

Exercises that Work the Abs Without Targeting Them

There’s a way to get six-pack abs by springtime without doing a single sit-up or crunch, or Roman chair leg raise for that matter.
Why Breast Cancer Survivors Should Lift Weights




































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}