

Constantly Swallowing, Tight Throat: Causes & Treatment

Always swallowing and throat tight?
Your need to swallow often, and that tight throat may be from a medical condition.
Or, it may be from plain anxiety, says Jordan S. Josephson, MD, FACS, ear, nose and throat specialist; director of the New York Nasal and Sinus Center, and author of “Sinus Relief Now.”
“There are two major reasons that cause patients to complain about constant swallowing and throat tightness.”
He continues: “Those two major reasons are post-nasal drip and gastroesophageal reflux disease (GERD).”
So though anxiety can cause frequent swallowing and a tight throat, keep open minded about sinus problems and allergies, which can cause the post-nasal drip.
“These two problems are often connected, and when one acts up the other gets worse,” says Dr. Josephson.
Mucus is normally produced in the nose and sinuses. Normally, 1-2 liters of mucus is produced.
It “traps dirt infection and pollution. The mucus drips into your throat and you swallow about 10-12 times per minute.”
Infection, allergy, pollution, tobacco smoke and chemicals can change mucus’s volume, pH and consistency.
“This causes inflammation to the throat, leading to tightness and swelling and the need to swallow more frequently, thus causing discomfort,” continues Dr. Josephson.
GERD can act up from post-nasal drip increase.
It’s a nasty cycle because when GERD acts up, “the reflux can cause swelling in the throat, causing the patient to feel tight in the throat, and this causes the patient to swallow more frequently than normal, giving the patient the sensation of constant swallowing,” points out Dr. Josephson.
The reflux can cause a laryngospasm, “a sudden closure of the voice box which can make the patient feel like they are choking. “This may spark a panic attack where the patient feels like (s)he cannot breathe.
“This sudden closure is to protect the lungs, and — although scary, will not cause the patient to suffocate.”
Thus, any alarming tightness or frequent, stubborn swallowing does not mean you’re literally having trouble breathing, even though the reflux can actually reach the nose/sinuses, causing further post-nasal drip, increasing swallowing and throat tightness yet.
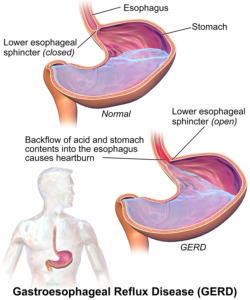
How acid reflux occurs. Image: BruceBlaus
The more you worry about your problem, the tighter your throat will seem to get, or actually get for real, because it is well-known that enough anxiety will cause tightness, or cause that so-called lump there.
Excessive swallowing, either due to GERD or anxiety, can, in and of itself, lead to the sensation of a tight throat.
So what is the treatment for problems with GERD and post-nasal drip? Dr. Josephson recommends a complete medical history, complete physical and appropriate tests by an ear, nose and throat physician.
“An accurate diagnosis with targeted therapy needs to be instituted to resolve the underlying causes for this complex problem to be resolved.”

Dr. Josephsonhas taught hundreds of physicians the technique of functional endoscopic sinus and nasal surgery, and was an instructor on the faculty at the Johns Hopkins Medical Center.
 Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/9nong

Quadriceps Muscle Dent Causes: Atrophy? MS/ALS? or What?

The quad muscle dent, that scary groove that appears in your quadriceps muscle, has more than one possible cause.
There are several causes of the quad muscle dent. The quadriceps dent is often described as being one to two inches long, and sometimes horizontal, and other times diagonal.
Occasionally a description for the quad muscle dent comes in as closer to vertical, and may exceed two inches in length, sometimes stretching for almost half the length of the thigh.
This article explains the causes of dents in your quad muscle.
“First of all, any obvious or irregular change in tissue structure — such as ‘denting,’ is worth getting checked,” says Dr. Joseph J. Ruane, a sports medicine specialist with OhioHealth Physician Group.
“Rarely (and I mean rarely) it may be a sign of something bad going on underneath.
“However, it may be reassuring to know that the dent is most often a loss of subcutaneous tissue (the fat under the skin) rather than loss of muscle tissue itself.
“This can result from local trauma (bumping hard into the corner of a desk). The fatty tissue is damaged in the impact, and sometimes shrivels and shrinks; leaving a dimple, or dent.
“Sometimes it fills back in, often it may not. Muscles do not atrophy in small, defined sections that leave dents.”
If you’ve been worried sick over the dent in your quad muscle, re-read Dr. Ruane’s last line:
“Muscles do not atrophy in small, defined sections that leave dents.”
Is a Quadriceps Dent Really Atrophy?
Oddly, people who have hypochondria related to MS or ALS have somehow formulated the idea that an early sign of muscle atrophy is some little depression or groove in the muscle.
Nowhere in the annals of medical literature is muscle denting named as a sign of wasting muscle tissue or atrophy, or any kind of disease.
Another cause of the quad groove, in addition to local trauma, is prolonged leaning of the thigh into an object.
A person who spends a lot of time at a counter of sorts may be unknowingly leaning (pressing) their thigh into a hard edge.
Or, perhaps they are seated, and something weighted is resting atop their thighs, such as a heavy briefcase.
Later on, the person happens to notice a small impression or depression in their quadriceps while changing clothes, showering or working out.
They fail to recollect earlier in the day when something was pressing into their leg and “molding” the dent. The image below shows natural quadriceps musculature.

Shutterstock/JRP Studio
Now…if only a tiny area of your natural muscle grooves is visible, do not take this out of context and think you have ALS or atrophy.
It’s normal for only a small area of natural grooves to be visible, creating a “small” indent.
Anatomy
Another cause of quad denting to consider is the natural anatomy of the muscle, if the fissure is more vertical than horizontal. A person who has toned thigh muscles, along with low body fat in that area, will likely see vertical dent in the middle of their quads, a few inches to several inches in length.
This fissure may come and go, depending on body position.
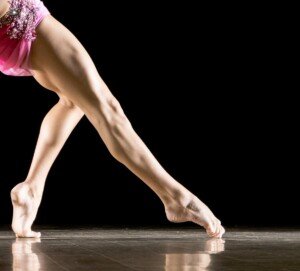
Dents are clearly visible in these buff legs.
Acquaint Yourself with Natural Dents
If you’re not sure what the cause of your quadriceps dents, impressions or grooves are, check out images of bodybuilders’ legs. They have very visible muscle definition and all sorts of grooves and “topography.”
This way you’ll learn what a normal muscle dent should look like, as opposed to what could be the result of local trauma.
 Dr. Ruane’s practice is dedicated to comprehensive, nonsurgical musculoskeletal care. He is active in clinical research and is a nationally recognized speaker and educator.
Dr. Ruane’s practice is dedicated to comprehensive, nonsurgical musculoskeletal care. He is active in clinical research and is a nationally recognized speaker and educator.
Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Top image: Shutterstock/KlaraBstock
Aneurysm Headache vs. Normal Headache: Recognizing the Difference
How can you tell if that sudden, alarming headache is an aneurysm headache?
Can a headache hurt really bad and still be normal?
Does an aneurysm headache feel different than a normal, regular headache?
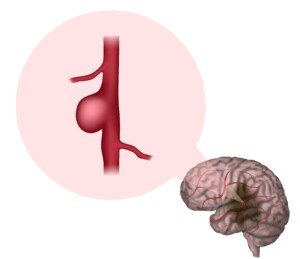
If you’re worried about your headaches possibly coming from aneurysms, then you likely already know to some extent just what an aneurysm is:
a blood-filled portion of a blood vessel, that causes it to “balloon” up into a sac-like structure; or, the blood-filled portion can be cylindrical in shape.
Nevertheless, an aneurysm has the potential, especially as it gets bigger, to rupture. The rupture may cause an alarming headache.
An aneurysm leak may also be over a period of days. A ruptured or leaking aneurysm is a life-threatening medical emergency.
Where do aneurysms come from?
“Aneurysms can either be developmental or acquired,” says Carol Redillas, MD, founder of Crescent City Headache and Neurology Center.
“A person can have an inherited weakness of the vascular wall, and develop an aneurysm with repeated, longstanding hemodynamic stress on the vascular wall.
“There are conditions that have been associated with an increased incidence of aneurysms such as connective tissue disorders, fibromuscular dysplasia, polycystic kidney disease, aortic coarctation, etc.
“Furthermore, trauma, infection, and cocaine use are also risk factors for developing aneurysms later in life.”
Can a person have an aneurysm for years and not know it?
“People can harbor an aneurysm without knowing it, as most are asymptomatic and are incidentally found only when a brain MRA is performed,” explains Dr. Redillas.
“They become symptomatic only when they reach a certain size and rupture or leak.”
Shutterstock/Veronika Zakharova
Do ruptured aneurysms always cause headaches?
“Aneurysms don’t always present with headaches, but those that rupture do. Before eventual rupture, aneurysms typically ‘leak’ and present with a sudden onset headache, i.e., sentinel headache,” says Dr. Redillas.
“Aneurysms that are located near the posterior communicating artery typically present with ptosis (drooping eyelid) and/or miosis (constricted pupil) without any headache at all.”
If a rupturing or leaking aneurysm is presenting with a headache, is it rare, then, for the headache to be the only symptom?
“A leaking aneurysm may present with headache as the sole symptom, but those that rupture may also be associated with change in mental status, loss of consciousness, seizures, meningismus or other focal neurological deficits, depending on the site of involvement.”
If someone has a severe headache seemingly out of nowhere, should they worry it might be an aneurysm rupture/leak?
“People always think that they have an aneurysm when they experience a severe headache,” says Dr. Redillas.
“The truth is, about 98% of headaches are due to a primary headache disorder such as migraine, cluster, tension type, etc.
“Headaches that have been present for years or even months are most likely migraines or tension type.
“Aneurysms are suspected only when a patient presents with a sudden-onset severe headache which may or may not be associated with ptosis, miosis, meningismus (neck stiffness and intolerance of bright light, with headache).
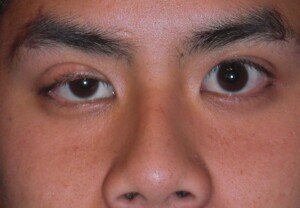
Ptosis: drooping eyelid
“However, pain is very subjective: a 5/10 pain for one may be a 10/10 for another; thus, a very unreliable way to diagnose headache.
“But if somebody presents with a new onset headache that is severe, especially those associated with exertion, an aneurysm should always be ruled out with further studies.
So if someone has had migraines or cluster headaches for years, how can they tell if that next sudden painful headache might be an aneurysm?
“Neurologists and headache specialists always look for a significant change in headache character, i.e., change in quality, location, associated symptoms, etc., to exclude other secondary causes.
“Aneurysmal headaches are typically short-lived because they usually rupture when it reaches a certain size.
“Thus, you don’t see a patient with a 10 year history of headaches due to an aneurysm.
“Aneurysms can also rupture with Valsalva’s maneuver (holding breath during physical exertion) such as straining, sexual activity, etc.”
So if an aneurysm headache is “short-lived,” can you elaborate?
And…suppose someone suddenly gets a “thunderclap” or severe headache…
It’s so bad it makes them stop cold what they are doing, but there are NO other symptoms.
At what point, then, should this person head to the ER?
After all, a benign headache can present in a very sudden, painful way.
And what if this individual doesn’t even have a history of sudden, severe headaches?
Dr. Redillas explains, “Aneurysmal headaches are usually ‘short-lived,’ like a thunderclap.
“However, not all patients with thunderclap headaches have an aneurysm, as these can also be seen in crash migraines, pituitary apoplexy, meningitis, increased or decreased intracranial pressure, thyroid disorders, etc.
“Patients are usually conscious with aneurysms that leak, and leaks can precede rupture by several days or even weeks.
“They can have a sentinel headache today, be symptom-free or headache free for weeks, then quickly deteriorate when the aneurysm ruptures.
“The best advice is, if you never had any significant headaches in the past, or this headache feels different than your usual headaches, it is better to have it checked than be sorry when you end up dead.
“If an MRA or a 4 vessel angiogram is negative for an aneurysm and the same headache recurs, then you can be rest assured that your headache is most likely benign.”
Dr. Redillas served as the head of the headache division at Ochsner Medical Center for over 10 years. In addition to headaches, she also treats a variety of other neurological conditions.
served as the head of the headache division at Ochsner Medical Center for over 10 years. In addition to headaches, she also treats a variety of other neurological conditions.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Top image: Shutterstock/Syda Productions
Cause of One Pupil Temporarily Dilated, No Response to Light
Can Aneurysm Cause One Pupil to Be More Dilated than the Other?

Numb, Tingling Hands and Arms in the Morning?

Numb, dead, tingling arms and hands…
Do you awaken in the morning, or in the middle of the night, realizing that an arm, hand or both are completely numb, as though dead?
When you poke at the arm or hand with your “good” hand, is it like poking a piece of dead meat?
There are multiple possible reasons why with sleep, your arm, hand or flingers will “fall asleep” and be numb and tingly.
I know what it’s like to awaken in the middle of the night with a totally numb arm or hand, but never thought much of it beyond the nuisance of it.
However, I came to realize that waking with a limb that feels dead or disturbingly tingly can be frightening to some people.
What causes a limb to go numb or dead and/or become tingly while a person sleeps?
Numbness or tingling that you feel in the arms is transmitted by the nerves that run from the arm to the brain.
Anywhere along this pathway, a nerve can be impaired.
“The more severe and more prolonged the symptoms, the more appropriate it is to seek medical advice,” says Dr. David Beatty, MD, a retired general practitioner with 30+ years of experience and an instructor of general medicine for 20+ years.
There may be pressure on the nerve in the arm itself — caused by being in the same position for a while, sustaining that pressure.
However, the point of pressure may also be in the spinal cord or brain.
This would be a much less likely possibility, and any pathology in these locations wouldn’t only cause morning symptoms.
You can quickly verify a positional cause by changing positions, such as removing what seems to have been sustained pressure on your arm or hand.
In my case, waking in the middle of sleep unable to feel my numb arm and/or hand, was always the result of falling asleep with the limb bent across my midsection.
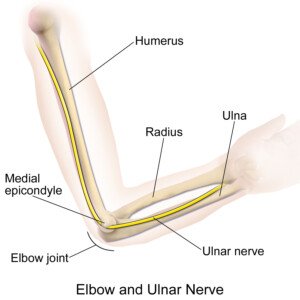
This position caused my elbow to press into the bed, which put pressure on the ulnar nerve (the “funny bone” nerve).
Source: BruceBlaus/CreativeCommons
Body Position’s Effect on the Hands and Arms, and Solutions
If you’ve been suffering from numb, tingly arms and hands after falling asleep, take note of the position of your body.
Where is your elbow?
Is the elbow against anything?
The pressure doesn’t have to be that much to offend the ulnar nerve.
This nerve is not buried deep within the arm, and hence, even what seems like light pressure on it can cause the entire limb to go dead or numb over a period of a few hours or even less, while you are fast asleep.
The ulnar nerve distributes into the hand and the pinky and fourth finger, so that if it’s receiving pressure at the elbow, this will affect the lower arm, hand and the fingers.
Simply straightening the arm at your side, palm up, will relieve the ulnar pressure.
To prevent my own arms from becoming numb overnight, I make sure to fall asleep with my arms straight at my sides, not folded over my midsection, and palms up, which minimizes pressure of the elbow against the bed.
Sleeping on your side can compress nerves in the arm closest to the mattress, so keep that in mind when slipping into bed.
Another cause of numb hands and fingers, though not the arm, while you sleep is a flexed wrist (meaning, the palm is bent towards the underside of the forearm).
This puts pressure on the median nerve, and the result may be a numb, tingly hand and fingers.
Solution? A wrist splint, available at drug stores and online.

Wrist brace. Shutterstock/Praisaeng
“There are lots of neurological diseases that can cause pins and needles or numbness in the arms and hands,” says Dr. Beatty.
If a new-onset numbness is present, and there’s no positional-related explanation, there may be a condition involved — especially if there are other symptoms with it.
Neurological but Benign Conditions
Waking with a numb, tingling, dead-feeling arm or hand is many times a benign condition, even though it’s very uncomfortable and can be quite startling to discover.
“This is a very common problem and the majority are caused by either carpal tunnel syndrome or cervical spondylosis,” says Dr. Beatty.
“The median nerve passes through a bony tunnel in the wrist as it goes into the hand.
“Anything that increases the pressure or tightness within the carpal tunnel can cause symptoms.
“Typically there will be numbness or pain over the thumb, index and middle fingers.
“Part of the ring finger may also be affected. Sometimes the symptoms are referred up the palmar side of the wrist and forearm.

“The symptoms are aggravated by tapping over the base of the palm (Tinel’s sign) or by fully flexing the wrist (Phalen’s sign).”
“CTS is often most troublesome in the morning — presumably because the wrists are flexed during sleep, and this puts more pressure on the median nerve,” continues Dr. Beatty.
“It’s more common in manual workers [plus heavy cashier and keyboard use].
“Any action that puts repeated pressure over the base of the palm can irritate the median nerve.
“The vibration from using power tools and the pressure needed to force a drill in are often to blame.
“Arthritis or a previous fracture of the wrist can trigger it.” So can obesity and drinking.
“If the symptoms are only affecting you briefly in the morning you can try adjusting your lifestyle to lose some weight and reduce alcohol intake.
“Manual workers may be able to adjust how they use tools to reduce trauma to the base of the palm.
“CTS usually causes less symptoms if the wrists are splinted in a straight position overnight.”
A differential for CTS is pronator teres syndrome.
“With pronator syndrome the median nerve is compressed as it passes between the heads of pronator muscles in the forearm,” says Dr. Beatty.
“It’s more common in people performing repeated pronator movements of the forearm (rotating the hand inwards).
“Typically there’s tenderness over the pronator muscles just below the elbow. This tenderness can be aggravated when someone tries to push back on your hand during pronation.”
Cervical spondylosis affects most people as they age, says Dr. Beatty.
“Osteoarthritis of the neck bones can form bony spurs that put pressure on the nerves leaving the neck.
“Disc degeneration means the discs are partly flattened. The vertebral bones are closer together, leaving less space for the nerves to emerge from the spine.
“If a nerve is squeezed it can cause pain, pins and needles or numbness in the area where that nerve supplies.
“This is less likely to happen when the neck is in a straight neutral position.
“During sleep the neck can get bent or twisted inadvertently, irritating the nerves going to the arms and hands.
“Many people with cervical spondylosis know they have a neck problem and some can trigger symptoms by moving the neck in a certain way.
“If the symptoms ease up quickly after waking, there probably isn’t too much to worry about.
“Perhaps adjust the number or type of pillow you use, trying to keep your neck in a relatively straight position. Sometimes using a soft cervical collar, temporarily, gives relief.
“The more persistent, severe or progressive your symptoms are, the more important it is to see your doctor.”
A Serious Cause
If the symptoms persist even after you get up, but then disappear, you might have suffered what’s known as a transient ischemic attack.
This is when a blood clot temporarily cuts off blood flow to the brain.
The younger you are, though, the less likely this will be the cause.
However, a TIA is not at the top of the list for most likely causes of morning numbness and tingling when a pressure-related cause can be ruled out.
 Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Seasontime
Cause of Tingling on Tip of Nose Includes Multiple Sclerosis
Limbs Fall Asleep Easily? Causes, Solutions to Numb & Tingling
Chest Pain, Pain/Numbness in Left Arm, Burping: Heart Attack?

Why Does My Eyelid Twitch After I Sneeze?
Achoo! And here comes the eyelid twitch, right after the sneeze.
Does this happen to you? Sometimes the eyelid twitch persists for a minute or so afterward.
And other times, maybe there is only one twitch of the eyelid after a good sneeze.
What Sets off an Eyelid Twitch after a Sneeze?
Could it be that the sneeze causes a jarring and jangling of things, and the tiny, minute muscles of the eyelid get caught up in the act?
“One mechanism is that sneezing involves so many muscles in a coordinated movement, that ancillary muscles may be incorporated by the body to ‘stabilize’ itself,” explains Dr. Ravish Patwardhan, MD, nationally-renowned neurosurgeon and founder of Comprehensive Neurosurgery Network LLC.
“Similar to grimacing when lifting heavy weights, this may also be a compensatory mechanism.
“The twitch that follows may be related to this mechanism, or recovering from this mechanism.”
No matter how strange the twitching (also known as fasciculation) may feel, one should not necessarily get alarmed over this.
This does not necessarily signal that you might have a neurological problem.
Millions of eyelids twitch day in and day out, all across the nation, many preceded by a good sneeze.
In fact, it’s not uncommon for a sneeze to result in a fasciculation elsewhere in the body, such as in the abdomen or trunk. This can happen.
A sneeze can be quite potent, getting what seems like the whole body involved.
This sudden physical action can literally shake someone halfway out of a chair, or cause a person to lose control of a car if it occurs while they are driving.
And we all know how loud sneezes can be, even though I’m convinced that the loudness of a sneeze is directly proportional to how many people are within earshot of the guilty person!
Yes, nobody sneezes as loud as a jackhammer when they are the only ones in a room.
I’m convinced that loud sneezing is an attention-getting tactic. But anyways, back to the eyelid twitching phenomenon.
Dr. Patwardhan continues, “Sneezing and yawning (as well as swallowing or breathing, for that matter) are very coordinated behaviors, done involuntarily many times; many theorize about why we yawn or sneeze (or sigh), as the full answer is really not presently known.”
In conclusion, any kind of benign muscle fasciculation, including that twitching eyelid, following a hard sneeze, is absolutely nothing to worry about.
Comprehensive Neurosurgery Network provides treatment for neurological disorders of the brain, spine and peripheral nerves.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Might Bad Headache Be Brain Tumor? Stop the Anxiety

How to stop fearing that your headache means a brain tumor…
Is that throbbing headache making you think you might have a brain tumor?
Many people will fear a brain tumor when they get a sudden, sharp pain in their head, especially if it feels like it’s behind their eye.
A person prone to hypochondria won’t be able to help but think that there is a brain tumor — located behind their eye, perhaps.
Do you fear that every headache means a brain tumor?
“The bottom line is that a headache is highly unlikely to be due to a brain tumor,” says Jonathan Stegall, MD, an integrative oncologist and medical director for The Center for Advanced Medicine, an adult cancer treatment center in Alpharetta, GA.
“It’s important to remember that headaches are quite common, while brain tumors are very uncommon,” though their level of media attention creates the illusion that they’re as prevalent as prostate or breast cancer.
“Virtually everyone has had a headache at some point in their lives,” says Dr. Stegall.
Millions of people every day suffer pain in their head somewhere.
If you work in a large office, you’ve certainly witnessed this: Is it not true that practically every day, several people are complaining of headaches?
And that bottle of aspirin gets passed around like a jar of candy.
- Meanwhile, only five per 100,000 Americans per year will be diagnosed with a tumor that starts in their brain.
- Plus, about two-thirds of brain tumors are actually benign.
“A brain tumor isn’t likely to cause a headache in isolation, nor is it likely to mimic a tension headache or migraine,” says Dr. Stegall.
“Headaches caused by a brain tumor are typically persistent, lasting days or weeks. They frequently get worse over time.
“Some studies have found that they tend to be more painful in the morning, or wake a person from sleep at night.
“Positioning can impact the headache too, for example, when lying flat.”
Bear in mind, though, that a harmless sinus headache can immediately worsen upon lying flat.
“The headache from a brain tumor can also be accompanied by neurological changes such as vision changes, trouble speaking, seizures, confusion and having trouble walking.”
A Benign Mass Can Still Be Deadly
For example, a benign mass on the pituitary gland can result in abnormally high secretion of human growth hormone, which can kill the patient if not treated.
A benign tumor can encroach upon parts of the brain that control vital functions.
This is why it’s so important to see your doctor about any unexplained, persistent and especially worsening symptoms including lack of appetite, increased appetite, dizziness, mental fog and fatigue.
How Brain Tumor Headaches Behave
Ask yourself, as should your doctor, if your headache ever goes away.
A brain tumor headache, due to the mass being there all the time and growing, may never totally go away — and in fact, be non-responsive to painkillers.
A headache that comes and goes — being completely gone at times — is likely related to migraine or tension, such as tension in the muscles about the neck.
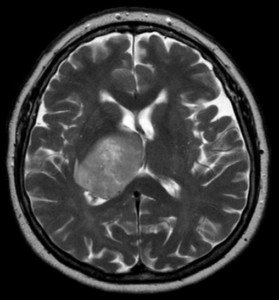
Glioblastoma multiforme. Credit: Hellerhoff
A tension type of pain can be quite aggravating, and a migraine type can be very strong and even quite debilitating.
Sometimes these pains tend to gravitate to the back of the eye, and this can be alarming.
But as painful as these can be, they do run their course, and also respond to over the counter painkillers, as well as sometimes just a big glass of water, since dehydration can be a causative factor.
A headache from a brain tumor would typically be ongoing for weeks or months.
And remember, if there are accompanying symptoms such as the ones already mentioned, more urgent medical attention is warranted.
Your headache is very likely from a harmless cause as long as it does not also come with worrisome symptoms, which also include numbness in a limb and sudden hearing loss.
To date, no known dietary risk factors exist for developing a brain tumor.
 Jonathan Stegall, MD, provides a long-awaited remedy for our cancer problem. Having a successful integrative oncology practice in Atlanta, GA, he’s seen firsthand what works and what doesn’t with cancer treatment. Dr. Stegall is the creator of the Cancer Secrets Podcast and author of “Cancer Secrets,” available on Amazon.
Jonathan Stegall, MD, provides a long-awaited remedy for our cancer problem. Having a successful integrative oncology practice in Atlanta, GA, he’s seen firsthand what works and what doesn’t with cancer treatment. Dr. Stegall is the creator of the Cancer Secrets Podcast and author of “Cancer Secrets,” available on Amazon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Stabbing Pain Behind Eye Possible Causes

It can be quite frightening to suddenly feel stabbing pain behind your eye.
Causes of Stabbing Pain Behind Your Eye
“Pain behind the eye can be from a number of causes,” says Dr. Ravish Patwardhan, MD, nationally-renowned neurosurgeon and founder of Comprehensive Neurosurgery Network LLC.
“The most important things to rule out are a tumor or aneurysm, which can usually be done by using an MRI scan with MR angiogram.”
Dr. Patwardhan also notes: “Other intrinsic problems with the eye can be determined by an eye doctor.
“Some conditions will exist without any of these findings, such as Tolosa-Hunt syndrome, diagnosed with the help of a neurologist.
“In either case, the proper healthcare professional will guide diagnosis and therapy.”
Next time you suffer stabbing pain behind the eye, what should you do?
This is probably NOT a rupturing aneurysm or a tumor.
Nevertheless, ongoing occurrences mean you should get this checked out.
If this nuisance is your only symptom (i.e., no visual disturbances, slurred speech, numbness in a limb, unsteady gait or one-sided weakness, dizziness or nausea), you should not lose sleep over this.
According to Dr. Patwardhan, the stabbing pain behind the eye is most likely just a benign headache in a nasty location, creating the illusion that it means a serious condition.
Even a mere tension headache or ice cream headache can cause considerable discomfort in this location.
Take it easy, relax, and to put your mind at ease, you may want to consider recording your incidents of severe pain behind an eye, so that next time it happens, you could refer to your documents and possibly say, “Hey, I had this 14 months ago and nothing came of it! So there’s no need to worry!”
As for Tolosa-Hunt syndrome, this indeed can cause pain around the eye, rather than what would be described as behind the eye.
However, key features of this neurological disorder include difficulty moving the eye or the eyelid, as well as a bulging eye.
Though a brain tumor can cause pain behind the eye, the longer the time passage without any additional symptoms that would be suspicious for a brain tumor, the more reassured you can be that there isn’t a cancer causing the problem.
Symptoms of a brain tumor include (no particular order) seizures, cognitive changes, one-sided weakness, clumsiness, nausea, vomiting, morning headaches, loss of vision in one or both eyes, blurry or double vision, tingling or numbness in the face, trouble with swallowing food, and even a bulging eye.
Comprehensive Neurosurgery Network provides treatment for neurological disorders of the brain, spine and peripheral nerves.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Lip Keeps Twitching: Causes, Solutions, when to Be Scared

Dang it, does your lip keep twitching?
What can it mean when a lip just won’t stop twitching? This can be very unnerving (no pun intended) for some individuals.
Not only can a twitching lip be noticeable to someone you are interacting with, but it can cause a lot of worry and anxiety.
Lip twitching is actually quite common.
Lip Twitching Causes
“Repeated twitching of any muscle is often related to a problem of either the muscle itself or the nerve(s) leading to that muscle,” explains Dr. Ravish Patwardhan, MD, nationally-renowned neurosurgeon and founder of Comprehensive Neurosurgery Network LLC.
“Examples of muscle problems include spasms (from overuse or tiredness of the muscle itself) or a condition where the nerve leading to the muscle is sometimes pushed on by an artery near the brainstem.
“An example is hemifacial spasm, where half of the face twitches, including eye and lip muscles on that side.
“In rare cases, seizures can cause twitching on half of the face as well.”
Before you start thinking that your lip is twitching because of a hemifacial spasm, rest assured, the vast majority of cases are caused by, as Dr. Patwardhan initially says, muscle fatigue.
In fact, twitching in the lips has the same general cause as twitching (also known as fasciculations) in the calves, arches of the feet, eyelid and even the tongue.
Any muscle, that can be voluntarily moved, is capable of sustaining fasciculations every now and then, or repeatedly throughout the day (as in eyelids and calves, though other locations can be “hot spots” for relentless fasciculations).
But because lip twitching has a unique feel, and because it occurs on the face, this can create undue anxiety in hypochondriac-prone people.
Shutterstock/Aaron Amat
Anything having to do with the face can bring with it undue anxiety and fear.
Lip twitching can also be caused by general anxiety, or anxiety over something specific, such as a relationship, paying the bills, problems at work, etc.
Muscle fasciculations can also be aggravated by excessive worry about muscle fasciculations themselves. This means that the more you worry and obsess about your lip, and the more you examine it in a mirror, the more likely it will twitch away.
Additionally, dehydration and a shortage of magnesium and potassium can cause fasciculations.
As for hemifacial spasm, Dr. Patwardhan says about the treatment: “An operation to put Teflon padding between the artery and nerve helps in the majority of cases.
“Treatment for spasms may require Botox. And, under severe circumstances, surgery may offer relief.”
Don’t fret if you have a twitching lip. Chances are very high that it will run its course and settle down before you know it.
This oddball symptom is not a sign of degenerative neurological disease. Talking will most likely bring some remission to the fasciculations.

Comprehensive Neurosurgery Network provides treatment for neurological disorders of the brain, spine and peripheral nerves.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

I Hit My Head Hard: When Should I Go to the ER ?

Have You Banged or Hit Your Head Really Hard Lately and Are Wondering If You Should Visit the ER?
Getting hit hard in the head isn’t pretty, and sometimes an ER visit is warranted.
Sometimes it’s a no-brainer that a visit to the emergency room is in order after one hits or bangs their head, if the ensuing symptoms are beckoning for medical attention.
But what if the symptoms are more subtle and the hit on the head doesn’t seem that bad?
When to Go to the ER
“Head injuries are very common and the vast majority are not serious,” begins Dr. David Beatty, MD, a retired general practitioner with 30+ years of experience and an instructor of general medicine for 20+ years.
“In the majority of people the skull is tough and prevents most trauma from causing brain injury.
“Young children, those on anticoagulants, the elderly and those with osteoporosis are exceptions to this rule.
“Having said that, head injuries are one of the major causes of death in young people. About 0.2% of people attending ER with a head injury die.”
Dr. Beatty provides 12 symptoms to look out for if you get hit in the head.
1) Severe or worsening headache
2) Vomiting
3) Confusion or drowsiness
4) Loss of consciousness
5) Convulsions
6) Visual disturbance such as double vision or loss of some of your visual field
7) Weakness or loss of power in a limb or a drooping on one side of the mouth
8) Clear fluid or bloody discharge from the nose or ears
9) If you take anticoagulants (blood thinners)
10) If there has clearly been a dangerous impact such as a high speed RTA or a fall from a great height
11) Memory loss
12) Any suspicion of non-accident injury
Hard Impact but No Symptoms
What if the impact to the head was really, really hard, but there weren’t notable physical symptoms immediately after?
Some trauma centers have used the criterion of whether or not there was an alteration of consciousness such as asking the same question over and over.
Nevertheless, a person with only one of the aforementioned symptoms may indeed have an intracranial bleed or subdural hematoma.
An ER physician may order a CT scan if the patient has only a headache, especially if it’s getting worse.
What if there’s a big bump or bruise — but no symptoms?
“After any significant bump on the head it’s good practice for the person to stay with a relative or friend for 24 hours after the injury — then if there’s a deterioration, further help can be called,” says Dr. Beatty.
“They should rest, avoid alcohol, avoid sedative drugs, avoid contact sports and avoid driving.
“The size of the bruise gives some measure of the severity of the impact and is certainly taken into account in infants.
“In adults it’s probably less useful as an indicator than the other factors listed above.”
CT Scan of the Head
“Most hospitals will have guidelines/protocols for which patient warrants a CT scan and which doesn’t,” says Dr. Beatty.
“If they are seeing the subdural patient on a good day they may not tick the right boxes to get the test done.
“The guidelines as to when a CT scan is needed will vary from region to region, but most of the above will warrant a CT scan.
“There may be specific guidelines such as more than one vomit or more than five minutes of memory loss.
“The assessment of confusion or drowsiness may involve assessment using a scale such as the Glasgow Coma Scale (GCS).
“This gives scores for eye opening, verbal response and motor response.
“A normal person would score 15 and a totally comatose person would score 0.
“The lower the GCS score the more appropriate it is to do a CT scan.”
Bleeding in the Brain
“After serious head trauma a rapid deterioration in the first few hours is usually caused by a bleed into the substance of the brain: an intra-cerebral hemorrhage,” explains Dr. Beatty.
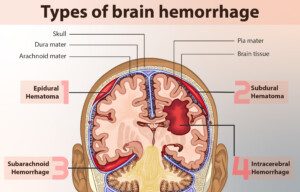
myupchar. comen
“These can bleed profusely, causing pressure and damage within the brain, usually leading to obvious symptoms. It’s easy to spot that things aren’t right.
“Relatively minor trauma can lead to a subdural hematoma when blood collects between the bones of the skull and the substance of the brain.
“The amount of blood may vary from very little to a great deal.
“Small subdurals may not cause many (or any) symptoms. They may cause obvious neurological symptoms with limb weakness.
“They can, however, cause more subtle symptoms which are less likely to be picked up by the doctor or the patient.
“The onset is often more gradual [a “chronic” subdural hematoma] — and the symptoms may fluctuate.”
For example the person may be normal one day but have confusion or memory loss the next.
A chronic subdural hematoma may also present with personality change, speech issues or drowsiness.
“A chronic subdural can grumble on for days or weeks before being diagnosed.
“Those on blood thinners and the elderly are more susceptible.
“If the elderly person doesn’t have normal cognitive function to begin with, it may be very difficult to pick up subtle changes in memory or mental ability caused by a subdural.”
Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Phovoir

How Do I Prevent Migraine Headaches at Night?

Migraine headaches can really mess up your sleep, but there’s good news:
Specific things you can do to finally get a good night’s sleep.
“Migraine headaches can happen at any time of the day or night,” says Daniel Kantor, MD, director of the Neurology Residency Program, Florida Atlantic University.
“We are often so busy during the day that some people are ‘too busy’ for the headache during the day (they have it but just don’t notice it), and only really feel the pain at night.”
And that’s when the problems begin, when the migraine headache sufferer tries to fall asleep.
First Tip for Falling Asleep Despite Migraine Headaches
“Sleep hygiene means doing things right to make the bedroom an environment conducive to sleep,” says Dr. Kantor.
“The bedroom is for two things: sleep and sex. It is not a place for TV watching, eating, etc. — these things are stimulating and will keep you awake and make it harder to fall asleep.”
You don’t want the bedroom to be a conditioned stimulus for staying awake.
Second Tip for Migraine Relief
The next thing is to make sure your doctor is doing all that’s possible to lower the intensity of your migraine headaches, since a good night’s sleep will be impossible if the pain is bad enough.
Dr. Kantor advises: “Try to relax before falling asleep — breathing exercises work great, as does mindful meditation.”
Wind down as bedtime approaches; avoid stressful or stimulating activities like heavy computer work.
Additional Sleeping Tips for Migraine Headache Sufferers
“Take a warm bath 45 minutes before your bedtime — as your body cools down, you get sleepier and sleepier,” says Dr. Kantor.
He also suggests taking a medication prior to bedtime that’s designed to subdue migraine pain, as these can induce a sleepy feeling.
“Go to bed at the same time every night, so that your body gets used to a full night’s rest.” This will help reset your body’s circadian rhythm.
“Make sure to talk to your doctor about your sleeping problems — they may be related to other problems, like anxiety, stress, depression and even sleep apnea and narcolepsy.
“Sleep apnea is important, not only because it makes you feel less rested, but also because it causes chronic migraines and can lead to an increased risk of heart attack and stroke.”
Being overweight, with a short thick neck, are risk factors for sleep apnea, though thinner people, including children (a tiny percentage) can have this treatable disorder.
If you suffer from migraines, it is absolutely crucial that you persistently try to remedy any sleeping problems. Dr. Kantor says, “We know that lack of sleep can trigger migraines.
Dr. Kantor is also President Emeritus, Florida Society of Neurology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}