

Can a Habit of Heavy Breathing Have a Serious Cause?

When is heavy breathing benign and when is it serious? Are some people just “naturally” heavy breathers – or, does this necessarily signal a problem?
“Heavy breathing is typically identified by an elevated rate of respiration at rest,” says Angel Coz, MD, FCCP, board certified pulmonologist, Associate Professor of Medicine, University of Kentucky, Lexington Veterans Affairs Medical Center. (more…)
Conditions that Mimic Exercise Induced Asthma Symptoms

Exercise induced asthma (EIA) has several skilled mimickers. You should know what they are.
“The classic symptoms of asthma include wheezing and shortness of breath,” says Angel Coz, MD, FCCP, board certified pulmonologist, Associate Professor of Medicine, University of Kentucky, Lexington Veterans Affairs Medical Center.
“However, several other conditions may present with similar symptoms and mimic asthma.”
Asthma Mimickers
“Heart ischemia: condition caused by insufficient blood flow to the heart muscle,” says Dr. Coz.
“Although the main symptom is chest pain, it can present as shortness of breath.”
Another name for this condition is angina. It’s caused by clogged (blocked) coronary arteries.
“Gastroesophageal reflux disease (GERD): Patients typically experience heartburn from abnormal flow of stomach acid back into the esophagus.
“GERD can cause asthma or make asthma more difficult to control.
“Chronic obstructive lung [pulmonary] disease (COPD): disease most commonly caused by chronic cigarette smoking that presents with shortness of breath and wheezing.
“At times, it can be difficult to differentiate COPD from asthma. Patients with COPD tend to have chronic productive cough.
“Congestive heart failure: accumulation of fluid in the lungs caused by inadequate cardiac pumping of blood. It can cause shortness of breath and at times wheezing.
“However, heart failure typically presents with lower extremity swelling, inability to lay flat, etc.”
Coronary artery disease and untreated sleep apnea are major risk factors for congestive heart failure.
“Vocal cord dysfunction or paralysis.” This is one of those conditions that a primary care physician may easily overlook when the patient describes what happened to them out of the blue.
Vocal cords are muscles. Muscles are prone to go into spasm.
In VCD, the spasm locks the muscles into a closed or nearly-closed position, blocking the airway.
The result is a sensation that the windpipe is as narrow as a straw.
Inhaling, no matter how hard one tries, is difficult, and not enough air gets through.
A VCD episode may last seconds to a minute or so, and can occur in the fittest athletes.
When struggling to inhale, the person will typically hear a wheezing sound.
 Dr. Coz is a pulmonary and critical care specialist at the Lexington Veterans Affairs Medical Center. He has a special interest in sepsis resuscitation and medical education.
Dr. Coz is a pulmonary and critical care specialist at the Lexington Veterans Affairs Medical Center. He has a special interest in sepsis resuscitation and medical education.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Coughing Be the Only Symptom of Pneumonia?

Is it actually possible for a person with pneumonia to have only one symptom: coughing?
“One of the hallmark symptoms of pneumonia is cough, but it is infrequently the only symptom,” says Angel Coz, MD, FCCP, board certified pulmonologist, Associate Professor of Medicine, University of Kentucky, Lexington Veterans Affairs Medical Center.
“Infrequently” is the key word here. It’s possible for coughing to be the only symptom of pneumonia—but this is very atypical.
It Happened to My Elderly Mother
My mother’s only symptom of her second bout of pneumonia was, indeed, just coughing.
- She reported no feverish feeling.
- She reported no decline in energy or increase in fatigue.
- She “felt fine” and was up and about as she normally always was.
- There were no aches or pains anywhere.
- Her throat was not sore or scratchy.
- All she had was a cough.
However, I did not like the sound of the cough, and it just seemed like a different animal than what would be caused by a typical common cold.
It didn’t sound like her usual cough from a cold or from acid reflux.
There was something about the way it sounded that made me highly suspicious that it was pneumonia, which was easily confirmed with an X-ray. The treatment was antibiotics.
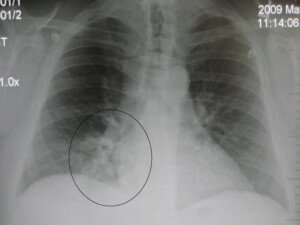
Pneumonia as it appears on an X-ray. James Heilman, MD, CreativeCommons
Dr. Coz continues, “It is important to mention that pneumonia tends to be more common in patients with pre-existing lung disease like emphysema (COPD).
“Those patients typically have cough on a regular basis. However, any change in the intensity of the cough or in the characteristics of the phlegm (increased amount, change in color, etc.) should alert the patient that a different process is occurring and that medical attention should be sought immediately.”
When a person over age 65 is diagnosed in the ER with pneumonia, even when the only symptom is a cough (or at least the patient reports this), it’s not uncommon for the doctor to recommend an overnight stay in the ER observation wing just as an extra layer of medical security.
Dr. Coz is a pulmonary and critical care specialist at the Lexington Veterans Affairs Medical Center. He has a special interest in sepsis resuscitation and medical education.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Stockbakery

Can You Die from an Exercise Induced Asthma Episode?

Exercise induced asthma, though seemingly well-controlled with an inhaler, can be deadly.
This is why, if you’ve been diagnosed with EIA, you should never think, “Oops, forgot my inhaler; well, I could do without it this one time.”
If you forgot your inhaler, then you must either go back home and get it, or, if that’s not practical at the time, then your only option is to cancel the physical activity.
Otherwise, you can be risking your life — even if you’ve never had any major complications in the past with exercise.
Exercise Induced Asthma Be Fatal
“Yes, although very rare, cases have been reported,” says Angel Coz, MD, FCCP, board certified pulmonologist, Associate Professor of Medicine, University of Kentucky, Lexington Veterans Affairs Medical Center.
“The best approach for EIA is to prevent the onset of symptoms with the use of an asthma inhaler prior to exercise.
“When symptoms present during exercise, it is important to stop exercise and provide immediately the asthma rescue inhaler (short acting beta 2 agonist).
“If not treated, symptoms can progress to severe status asthmaticus and even death.”
You certainly don’t want to take this chance if you forgot your inhaler, even if the physical activity is going to occur near a medical facility.
Severe Status Asthmaticus Defined
This is another name for a severe asthma attack that does not respond to inhalers or the hormone epinephrine given under the skin.
It’s as much a medical emergency as is a heart attack, and can occur to an athlete who, despite having been diagnosed with exercise induced asthma, is working out without an inhaler.
Even if the diagnosis is that of mild or moderate, an athlete or a person working out for fitness may die from an untreated episode of exercise induced asthma.
This doesn’t mean that a diagnosis of asthma means you shouldn’t work out or should avoid strenuous activity.
It just means that you should not exercise without your inhaler very nearby.
The inhaler should, ideally, be on your person for a quick retrieval in the event of a problem.
If you fear dying from an asthma attack triggered by exercise, then make the plan of immediately ceasing activity at the first sign of symptoms.
Next, immediately use your inhaler. Do not wait out the situation.
There is no data on what the average wait time, for using their inhaler, was for the athletes and exercisers who died from an asthma attack.
Perhaps most delayed the use because they had to complete those last few reps with a barbell, or had to make that hoop shot.
Ceasing activity immediately means IMMEDIATELY. Forget the set or game.
Dr. Coz is a pulmonary and critical care specialist at the Lexington Veterans Affairs Medical Center. He has a special interest in sepsis resuscitation and medical education.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: hutterstock/Zania Studio

Asthma vs. Vocal Cord Dysfunction: Symptoms Comparison

Asthma and vocal cord dysfunction (VCD) are strikingly similar in symptom presentation, but one subtle difference can point much more to vocal cord dysfunction. (more…)

Angina vs. Exercise Induced Asthma: Symptom Comparison

Is that chest tightness and shortness of breath from exercise induced asthma?
OR is it angina, in which blood flow to the heart is reduced due to clogged arteries?
The symptoms of angina and exercise induced asthma have some overlap. (more…)

Can Strenuous Workouts Dilate or Enlarge the Aorta?

Aortic dilatation, or dilation, refers to an enlarged portion of the aorta, the biggest blood vessel in the body that comes out of the heart.
An aortic aneurysm, or a bulge in a section of the aorta, arises from an enlarged or dilated area.
As the aneurysm grows in size, the inner walls of the aorta at this location become thinner—and hence more prone to rupture or dissection.
“Patients whose ascending aortas are more than 4 centimeters in diameter are generally considered to have dilation,” says cardiothoracic imaging specialist Christopher Maroules, MD, in a report.
As the area of dilatation grows, the aortic walls weaken. Think of what happens to the rubber of a balloon that’s being over-filled with air.
Study Shows Former Professional Football Players More Likely to Have Enlarged Ascending Aortas
The ascending portion of the aorta is the section that ascends out of the heart and supplies the coronary arteries.
Dr. Maroules et al was curious as to whether or not years of playing professional football — what with its strenuous nature and highly intense workouts—could lead to aortic dilatation.
• 206 former NFL athletes were compared to 759 controls from the Dallas Heart Study.
• All were older than 40.
• Body mass index exceeded 20.
• Cardiac gated non-contrast CT scanning was used to measure the aortas.
• Calcium scores were taken to get an indication for the presence of heart disease.
• Nearly one-third of the former athletes had aortic diameters exceeding four centimeters.
• Only 8.6 percent of the controls had aortic diameters over four centimeters.
• Age, BMI and cardiac risk factors were adjusted for, and still, the former athletes were twice as likely to have an aorta over four centimeters.
• Heart disease was ruled out as a factor because the calcium scores of both groups were similar.
Risk factors for an aortic aneurysm are smoking, high blood pressure and genetic connective tissue disorders.
So what’s going on?
Is there something about pro football that enlarges the ascending aorta?
Dr. Maroules, in his report, surmises that the strenuous training exercises cause remodeling of the aorta.
Gee, this begs the question: What about other forms of sport for which intense, strenuous training is key?
Football players lift hard and heavy in the gym, and are subjected to grueling workouts on the field, including training against resistance (e.g., pushing sleds loaded with weights).
However, other athletic disciplines also entail highly strenuous exercise, such as CrossFit, strongman, powerlifting, hockey and gymnastics. And even your ordinary gym rat who kills it at the health club.
And if the running component of football, rather than the resistance component, is the chief cause of aortic dilatation, then we must wonder if elite soccer players and sprinters are at risk for aortic enlargement.
“It remains to be seen if this remodeling sets athletes up for problems later in life,” says the report.
Much more research is needed as a follow-up to this investigation.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com Racool_studio

Waking up Every Hour with CPAP: Causes & Solutions

There are quite a few causes for waking up every hour or so despite compliance with CPAP therapy.
If this is happening to you, the obvious approach is to first identify if there are any new situations that are awakening you every hour, such as (by coincidence) a new pillow that’s not as comfortable as you thought it might be; a new pet that hops up on your bed throughout the night; etc.
Another obvious approach is to see if a condition — that pre-existed your use of CPAP — is the cause of waking up so often.
For example, do you have unresolved acid reflux?
Waking up Every Hour with CPAP: Causes & Solutions
“There are many potential reasons for this, and more history is needed before a conjecture could be made,” says Joseph Krainin, MD, board certified in sleep medicine and neurology and founder of the online sleep apnea clinic Singular Sleep.
“I recommend consulting with a sleep doctor to evaluate for sleep apnea treatment efficacy related issues vs. an additional co-morbid sleep disorder.”
In other words, an issue with the CPAP therapy is more likely to be causing frequent awakenings than is, say, restless leg syndrome.
Possible Causes of Frequent Waking Up Despite CPAP Compliance
• Swallowing air
• Too much air pressure
• Change in sleep position causing body part to contact hose
• Eye or lip irritation from exhaust flow
• Sore nose from nasal pillows
• Dry nose from lack of humidity
• Wet nose from too much humidity
• Irritated or itchy nose/lip from the mask
• Mask leaks
• CPAP noise
• New sleep position to accommodate mask/hose efficacy
Psychological Cause of Frequent Wakeups
“It is fair to say that among people with no biological explanation for repeated waking, stress is a common cause,” says David D. Clarke, MD, President, Psychophysiologic Disorders Association (stressillness.com), Clinical Assistant Professor of Gastroenterology Emeritus, Oregon Health & Science University, and author of “They Can’t Find Anything Wrong.”
Once you’re asleep, daytime worries and anxieties get temporarily pushed to the background, but eventually barge their way into the foreground and awaken you.
The anxiety may be solely related to your new status as a “hose head.” For example, how will this impact business and vacation travel?
Will you ever adjust to that thing on your face? This thought alone can be enough to waken you every hour.
“I divide stresses into two groups,” says Dr. Clarke. “Those that are obvious and can be accurately assessed when a person looks at their life and (2), those that are not as readily recognized. Among the latter are:
“Poor self-care skills (working to meet the needs of others to the neglect of oneself, often linked to lack of enough opportunities to play in childhood).
“Long-term impact of adverse childhood experiences.
“Unrecognized depression, anxiety or post-traumatic stress (quite common for these to be present but not detected by the sufferer or their doctor).”
The key, then, is to determine if your repeated awakenings, despite compliant CPAP use, were actually present prior to getting on CPAP.
Are you awakening more frequently with CPAP? Maybe it only seems you’re awakening every hour. Make a note of the times you awaken for no apparent reason.
If you’re clearly awakening more often since beginning CPAP treatment, chances are high that this is linked to a problem with the CPAP device – which includes stressing about having to use it lest you develop serious cardiovascular problems from untreated sleep apnea!
 In 2013 Dr. Krainin was elected a Fellow of the American Academy of Sleep Medicine, an honor reserved for sleep doctors who’ve made significant contributions to the field in education, research and service.
In 2013 Dr. Krainin was elected a Fellow of the American Academy of Sleep Medicine, an honor reserved for sleep doctors who’ve made significant contributions to the field in education, research and service.
 Since 1983 Dr. Clarke has successfully cared for over 7,000 patients with stress illness.
Since 1983 Dr. Clarke has successfully cared for over 7,000 patients with stress illness.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Mr.Nikon
Nocturia Continues after CPAP Therapy: Cause & Solution

You’re now on CPAP for the sleep apnea that’s been causing endless overnight trips to the john, but doggone it, you still suffer from nocturia. (more…)
How Long Can You Have Untreated Sleep Apnea Without Damage?



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}