

HEART BYPASS SURGERY (CABG): RISKS, COMPLICATIONS, RECOVERY

My mother had quintuple bypass surgery, so I was inspired to interview a cardiothoracic surgeon to answer the many questions I had.
These questions are based on my mother’s symptoms and other concerns following surgery.
They’re questions that anybody has when they or someone they know undergoes coronary bypass surgery (coronary artery bypass grafting — CABG).
CABG Post-op Complications that Seem Scary but Aren’t

Shutterstock/virgo1957
All sorts of things may develop immediately following this major procedure, making visitors very worried.
This includes a certain kind of heart rhythm deviation, excessive swelling, fluid in the lungs and mental confusion.
Crazy things occurred to my mother following her quintuple bypass, and at first, I was up in arms, and then I settled down with the power of knowledge. Read more.
Chest Pain After CABG
How long after coronary bypass surgery is it normal for the patient to experience chest pain?
How likely is it that chest pain post-surgery could mean something is wrong with the heart, possibly a pending heart attack? Go to article.
Trouble Breathing After Coronary Bypass Surgery
There are several causes of shortness of breath or labored breathing following this procedure.
And it’s SCARY to witness in a loved-one; you wonder if it means a problem with the heart, like a heart attack about to happen. Continue…
Abdominal Pain After CABG
Shutterstock/ShotPrime Studio
The night my mother was discharged from the hospital, she complained of severe abdominal pain and was crying and moaning. This was frightening and I phoned the doctor on call.
He told me to get her to the ER. Severe stomach pain can follow CABG, even a few weeks later, and can have different causes, including that of life-threatening. Continue…
Appetite Loss Weeks After CABG

Shutterstock/Photographee.eu
Loss of appetite is normal after any major surgery. But what if it persists for weeks after? Are you or a family member struggling with this?
My mother’s appetite went down the tubes for weeks following her procedure, and she kept losing weight and looked sickly.
Weight loss under these circumstances is potentially dangerous. Possible cause? Continue…
Can CABG cause dangerous blood pressure drops for weeks afterwards?

Shutterstock/ Alexander Raths
Since your (or a family member’s) coronary artery surgery, have you been struggling with severe blood pressure drops every time you rise from a seated position? This is called orthostatic hypotension. Continue…
Life Expectancy of Elderly CABG

Shutterstock/ wavebreakmedia
Is it worth it for an elderly person to even have coronary bypass surgery? How many years can this major, invasive procedure add to their life?
Well, if the doctor tells you that your aged parent or spouse needs CABG or else they’ll soon have a massive heart attack, you don’t have a choice. Continue…
Causes of Vomiting After CABG
What does it mean if a patient vomits after this surgery, well after the general anesthesia has cleared out of the system? There are different causes. Continue…
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ChaNaWiT

Post-Surgical DVT Treatment without a Blood Thinner?

How is a post-surgical DVT treated if giving the patient a blood thinner can cause dangerous internal bleeding?
If a DVT develops during or after surgery, how is it treated if giving the patient a blood thinner (anticoagulant) can cause life-threatening internal hemorrhaging?
I was alarmed when the doctor ordered no treatment for my mother’s post-surgical DVT in her neck.
There was the risk that it would break loose and go to her lungs and become a pulmonary embolus — a blood clot blocking a vein leading to the lungs, which can kill in minutes.
Instead, the “big DVT” was just left to sit there while she was in ICU following her quintuple bypass surgery.
I asked, “Why can’t you give her coumadin or heparin?” I was told that these blood thinning drugs could very well spark a very serious internal bleeding somewhere, putting her life at immediate risk.
I was also told that the blood thinners would not break up the DVT, only prevent it from proliferating further.
I then asked why not give her tPA (a clot-busting drug)?
I was given the same reason about the internal bleeding. I was also told that the chances were small that the DVT would go to her heart.
Well gee, how could they know that?
“Generally, DVTs are treated with anticoagulation (blood thinners), except when there is a contraindication for this,” explains Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“Along with recent surgery, there is a long list of other reasons why one would not want to systemically anticoagulate a patient (trauma, head injury, brain tumors, frequent falls, etc.).
“In these cases we would place what is called a ‘filter’ in either the IVC (in case of DVT in legs) or SVC (if DVT is in arms/neck veins).”
Inferior vena cava and superior vena cava are known as IVC and SVC, respectively.

IVC filter. BrusBlaus/CreativeCommons
“These devices take 15 to 20 minutes to insert percutaneously and are meant to prevent pulmonary embolism, not formation of DVT.”
Nobody at the hospital mentioned anything about any filter.
The IVC and SVC are “the two largest veins that return the venous blood back to the heart,” says Dr. Gashti.
The filter in these locations would prevent a dislodged DVT from traveling deep enough into the lungs or heart to cause a catastrophic event.
If a loved one is fresh out of surgery, recovering in the ICU or regular hospital room, and it’s discovered they have a DVT (an ultrasound should be ordered if there is swelling in a leg or arm), ask about an IVC or SVC filter!
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
How Does Surgery Cause a DVT?
A vascular surgeon explains why most DVTs form during surgery rather than during the immobility after the surgery.
The estimate for annual U.S. deaths from pulmonary embolism (which begin as a deep vein thrombosis) ranges from 50,000 to 200,000.
When a pulmonary embolism is fatal, it’s often a sudden, unexpected death, often attributed to heart attack.
“The difficulty is that you will never know the exact numbers unless you did an autopsy on everyone with sudden death, which is not a practical thing,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“So most of these numbers are estimates, and in my opinion are very conservative.”
Immobility is a major risk factor for a DVT.
This is why after knee replacement surgery, for example, the patient wears surgical stockings and their legs are wrapped in a special device that encourages increased blood circulation at varying intervals.
I was surprised to learn, though, that most DVTs form at the time of surgery. My mother had a DVT in her neck following bypass surgery.
People who take long airline flights in which their legs are crammed immobile in a small space are warned to guard against DVT.
Dr. Gashti explains, “During surgery, especially when you are under general anesthesia, you are completely paralyzed, so you not only are immobile, but also not have any of your muscle tone (muscle pump) that would help with movement of the venous blood from the extremities, thus causing stasis which can lead to DVT.”
When I told my mother this (long after she had recovered from the bypass), she asked why, then, don’t people develop DVT overnight during sleep.
Well, I’m not a doctor, but my response was based on common sense:
We are not perfectly immobile during sleep. When under general anesthesia, yes, we are perfectly immobile because of a chemically induced, very deep unconsciousness—an unnatural state that can mess with blood circulation.
Though some people claim they don’t move at all while asleep, and even awaken seemingly in the same position that they were in when they went to bed, there are still many minute muscle movements and minute shifting while they are asleep.
There may also be myoclonus incidents – sudden jerking of a muscle.
If you’ve ever seen time lapses of people sleeping overnight, they indeed change positions many times. I’ve observed my parents while they were fast asleep.
It’s never long before a foot twitches or a hand or whole arm moves, even though they are asleep.
Sleep is a natural, necessary process, and nature would not have engineered it to cause a DVT.
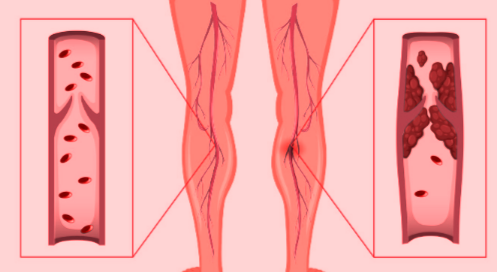
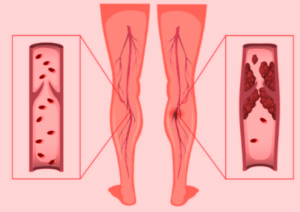
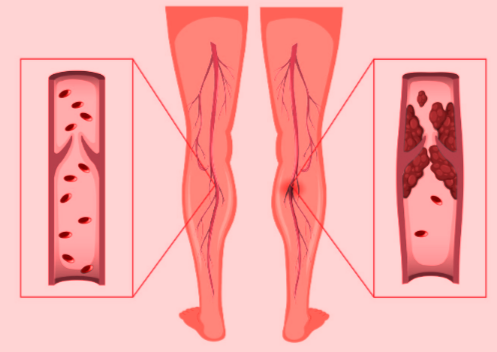
Symptoms of a Deep Vein Thrombosis
• Swelling where the blood clot is (lower leg, upper leg, pelvic region)
• Cramping or pain in the area (particularly the lower leg, but can also be in the foot)
• The pain does not go away with resting the leg or lying down.
• The suspect area is tender to the touch.
• Redness and/or extra warmth in the affected area
• The color may also be bluish or pale
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Plantar Fasciitis Cause Foot Pain on Outer Side?

A foot care specialist addresses pain on the outer side of the foot being caused by plantar fasciitis.
“Most pain associated with plantar fasciitis originates near the point of insertion of the plantar fascia in the medial area of the calcaneus,” says Bob Thompson, certified pedorthist, executive director of the Institute for Preventive Foot Health (www.ipfh.org).
A pedorthist is a medical professional who designs footwear and devices to alleviate foot pain.
The medial side of the calcaneus means inner side of the foot, near the ankle.
When I had plantar fasciitis years ago, I had burning pain along the outer side of my foot, as well as at the medial calcaneus and smack bottom of the heel.
Thompson explains that the plantar fascia consists of inner, central and lateral (outside of the foot) bands of tissue, so that, yes, it is also possible to have inflammation in the lateral (outside) band.
“But if you read the literature, this is unusual,” adds Thompson.
“Plantar fasciitis is most likely to occur in the central band and manifest in pain in the center or medial aspects of the foot in the heel area.”
Whether plantar fasciitis causes pain on the outer side of the foot or the central or heel areas, conservative therapy is the first line of treatment.
This approach typically includes rest to avoid activities that aggravate the condition, along with applying ice to reduce swelling.
Over-the-counter anti-inflammatory medications may help manage pain.
Stretching exercises for the calf muscles and the plantar fascia can improve flexibility and reduce tension.
Orthotic devices, such as custom or over-the-counter arch supports, are used to provide better foot alignment and reduce stress on the heel.
Overnight splints (shown below), which keep the ligament bands stretched, can help immensely.
They come in a variety of styles and are sold online as well as at footcare retailers.

 Robert Thompson is a nationally recognized speaker on the topics of preventive foot health and soft tissue injury prevention.
Robert Thompson is a nationally recognized speaker on the topics of preventive foot health and soft tissue injury prevention.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Seasontime

6 Causes of Pain on the Outside of Your Foot

A foot pain expert describes the seven possible causes of pain on the outside (lateral) part of the foot.
Pain along the outside or lateral part of the foot can have one (or more) of six possible causes, according to Bob Thompson, certified pedorthist, executive director of the Institute for Preventive Foot Health (www.ipfh.org).
A pedorthist is a medical professional who designs devices and footwear to alleviate foot pain.
Arthritis
“There are three main joints on the lateral side of the foot – the calcaneal/cuboid, the cuboid/fifth metatarsal, and the fifth metatarsal/proximal phalange joint where the little toe begins,” says Thompson.
“In addition, closer to the center line of the foot are the cuboid/lateral cuneiform, cuboid/navicular and cuboid/fourth metatarsal joints.
“Lateral foot pain can be caused by inflammation (arthritis) in any of these.”
Cuboid Syndrome
“Where the cuboid bone articulates with the calcaneus it forms the calcaneocuboid joint,” says Thompson.
“This joint functions to lock the foot for stability on toe-off. Cuboid syndrome happens when the cuboid gets displaced or dislocated relative to the calcaneus, causing pain when walking or running.
“In cuboid syndrome the joint does not function properly, causing pain and weakness on the lateral side of the foot.”
Tendonitis
Thompson says that several major tendons run through the side of the foot. If any are inflamed, the side of your foot will hurt.
Muscle Strain
“The major muscles on the lateral side of the foot are the flexor digiti minimi and abductor digiti minimi, along with their tendons,” says Thompson.
Shutterstock/Seasontime
“Also, a larger and important tendon, that of the peroneus longus muscle, runs through the lateral side of the foot on its way to be joined to the lateral side of the first cuneiform and proximal end of the first metatarsal.”
Yes, sounds fancy, but a muscle strain indeed can cause pain along the outer side of the foot.
Fracture
“A broken bone in the foot, especially if it is one in the fifth phalanges, the fifth metatarsal or the cuboid will certainly cause lateral foot discomfort!
“The fifth metatarsal is especially prone to avulsion and Jones fractures.
“In an avulsion fracture, a small piece of bone is pulled off the main portion of the bone by a tendon or ligament.
“This type of fracture is the result of an injury in which the ankle ‘rolls’ (common among athletes). Avulsion fractures are often overlooked when they occur with an ankle sprain.”
Many years ago I had an avulsion fracture. I sprained my ankle playing volleyball.
In the ER the doctor said that the ligament tear took a small piece of bone with it. I heard him behind the curtain tell somebody (presumably a nurse), “It doesn’t look good.”
I had pain on the outer side of my foot, but of course, I knew why; the pain on the outer side of my foot wasn’t a mystery. I fully recovered from this sprain.
“Jones fractures occur in a small area of the fifth metatarsal that receives less blood and is therefore more difficult to heal,” says Thompson.
“A Jones fracture can be either a stress fracture (a tiny hairline break that occurs over time) or an acute (sudden) break.
“Jones fractures are caused by overuse, repetitive stress or trauma. Pain, swelling, tenderness on the outside of the foot, difficulty walking and bruising may all be symptoms of these fractures.”
Ankle Sprain
I’ve had more than one ankle sprain as an athlete, and they do cause pain along the outer side of the foot. But at least when an ankle sprain occurs, you know why you have the pain.
“Pain can radiate throughout the lateral side of the foot,” says Thompson.
Robert Thompson is a nationally recognized speaker on the topics of preventive foot health and soft tissue injury prevention.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/KlaraBstock
Hoarse Voice, Trouble Swallowing: Causes

Two doctors explain the possible causes of a hoarse voice coupled with trouble swallowing
The first expert source for this article about the causes of the symptom duo of hoarse voice and swallowing difficulties is John A. Elefteriades, MD, William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
You’re probably wondering why a consulting physician for hoarse voice and trouble swallowing would be an aorta specialist, being that the aorta is the largest blood vessel in the body, and arises out of the heart.
“An aortic aneurysm can, rarely, put pressure on the esophagus by virtue of its size,” explains Dr. Elefteriades, “and cause the symptom complex described.”
An aneurysm is a ballooned portion of a blood vessel. When a portion of the aorta is abnormally enlarged, this is an aneurysm.
Think of what a snake looks like after it just swallowed a big egg — the snake’s body is long and tube-like, and the egg inside bulges at some point along the snake’s body.
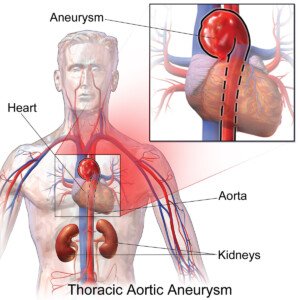
BruceBlaus/CreativeCommons
That’s kind of what an aneurysm looks like (but not always, as there are different kinds of aneurysms). But you get the picture.
Plus, if the aneurysm is located on the arch or descending portion of the aorta, it can cause compression of the nerve that controls the vocal cords, as this nerve passes along the aorta,” adds Dr. Elefteriades.
This disrupts signals to the vocal cords and will result in a hoarse voice.
If you have trouble swallowing, plus a hoarse voice, chances are that this is NOT from an aortic aneurysm.
Dr. Elefteriades says that these symptoms more commonly arise from “problems with the esophagus,” as well as “benign conditions, like reflux disease.”
Difficulty swallowing and a hoarse voice occurring together can also be caused by tumors, says Dr. Elefteriades.
What does an ear, nose and throat doctor have to say about causes of a hoarse voice?
Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology, says that acid reflux is a common cause of hoarse voice.
But she also includes in the list the following: “Laryngitis, vocal cord polyps or nodules, long-term smoking irritates the vocal cords causing chronic swelling, vocal cancer.”
But what if trouble swallowing is tossed in?
“The most common cause of a choking sensation,” says Dr. Silvers, “is acid reflux, ‘silent reflux’ with our indigestion or heartburn symptoms,” when a foreign object in the throat has been ruled out.
Stomach acid comes up into the back of the throat, making it swell, says Dr. Silvers.
“This makes it hard to swallow. Patients may describe choking sensation or trouble swallowing.” A cough may also be present.
Believe it or not, stress can cause difficulty swallowing and a hoarse voice, because, as Dr. Silvers explains, stress can cause stomach acid to rise up into the back of the throat.
Trouble swallowing, though not necessarily with a hoarse voice, can also be caused by a hiatal hernia.
Both of these symptoms can also be a sign of esophageal cancer.

Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.

An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Nik Stock
Sources:
webmd.com/heartburn-gerd/understanding-hiatal-hernia-symptoms
mayoclinic.com/health/esophageal-cancer/DS00500/DSECTION=symptoms

Swollen Neck, Face & Arms: Get to ER Immediately!

If you have a swollen neck, face and arms, this can mean a life-threatening condition that could result in brain death.
The expert source for this article about the cause of a swollen neck, face plus arms is John A. Elefteriades, MD, William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
“A swollen neck and arms is serious and should lead to immediate attention,” says Dr. Elefteriades.
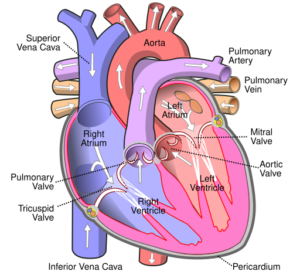
“This symptom complex may well mean that the ‘superior vena cava,’ or SVC, the great vein that drains the upper body, is narrowed or occluded.”
Occluded means blocked.
“If you do not seek immediate attention,” continues Dr. Elefteriades, “your brain may swell, leading to brain death.
“Such narrowing can be caused by tumors compressing the SVC, by blood clots in that area, or, rarely, by an aortic aneurysm compressing the vena cava.”
This situation is termed SVC syndrome.
The most common cause is cancer. Other causes besides blood clots from surgery, and (rarely) the aortic aneurysm, include syphilis and tuberculosis.
The swelling of the neck, face and arms develops gradually; it is not sudden or overnight. Shortness of breath may also be present.
Additional symptoms of SVC syndrome are a blue tinge to the skin, cough and chest pain.
Treatment of the swollen face, neck and arms depends upon the underlying cause that’s disrupting the function of the superior vena cava (see diagram below of the SVC).
Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Portnova Tatiana
Source: medicinenet.com/superior_vena_cava_syndrome/article.htm

Chest Pain with Trouble Swallowing: Dangerous & Benign Causes

The causes of chest pain combined with difficulty swallowing can be benign…or life-threatening.
The symptom duo of chest pain plus trouble swallowing is very frightening.
It can occur suddenly and at any time for people who have the life-threatening — or benign — conditions that would lead to this pairing of symptoms.
The expert source for this article about the causes of chest pain with trouble swallowing is John A. Elefteriades, MD, William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
This pair of symptoms is nothing short of alarming. “Trouble swallowing generally reflects problems with the esophagus, the swallowing tube,” says Dr. Elefteriades.
“These problems may be due to benign conditions, like reflux disease, or to tumors.
“Pain during swallowing reflects partial blockage impeding the contractile wave that propels food in the esophagus.”
Hopefully, chest pain with difficulty swallowing is not more serious than some acid reflux (gastroesophageal reflux disease).
But Dr. Elefteriades adds, “An aortic aneurysm can, rarely, put pressure on the esophagus by virtue of its size and cause the symptom complex” of chest pain and trouble swallowing.
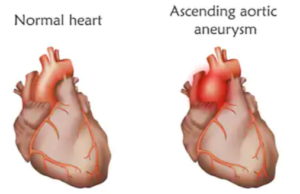
What is an aortic aneurysm?
- An aneurysm of the thoracic aorta is a portion of this great vessel that has abnormal enlargement.
- When an aortic aneurysm causes symptoms, it is time for surgical repair.
- Usually, these do not cause any symptoms, and most are discovered by accident during imaging for an unrelated issue.
Shutterstock/Veronika Zakharova
When an aortic aneurysm is asymptomatic and the patient does not have a connective tissue disorder, the aortic aneurysm is given a “watchful waiting” approach.
This protocol is to see if it gets big enough to warrant surgical repair; routine imaging tests are done to follow it.
Trouble swallowing along with chest pain can also be caused by a hiatal hernia, acid reflux or esophageal cancer.
Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/fizkes
Sources:
webmd.com/heartburn-gerd/understanding-hiatal-hernia-symptoms
mayoclinic.com/health/esophageal-cancer/DS00500/DSECTION=symptoms
Chest Pain with Neck Pain: May Be Heart Attack

A heart surgeon addresses the likely cause of chest and neck pain occurring at the same time.
Sudden chest pain, or gradually worsening and reaching severe proportions, is frightening enough.
But add neck pain to this symptom, and you have a pairing that can potentially mean a heart attack.
It’s one thing if your neck pain, ache or soreness is obviously occurring independent of a sudden onset of chest pain.
That’s entirely possible. Your neck could be sore from a kind you developed overnight.
Nevertheless, sudden severe chest pain still means you need to get checked out right away.
The expert source for this article about the causes of chest pain that is accompanied by neck pain is John A. Elefteriades, MD, William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
Sudden Pain in the Neck and Chest: Heart Trouble Possible
Dr. Elefteriades explains, “Chest and neck pain often accompanies a heart attack or an angina episode.”
Angina is a medical condition in which the heart is shorted of oxygen flow due to narrowed or constricted coronary arteries.
The obstruction in the arteries is caused by plaque buildup, which shrinks the diameter of these blood vessels or may cause a very narrowed section.
Angina may occur only upon physical exertion (and it doesn’t have to be a lot of exertion—may be only minor) and mental stress.
Or, it may occur spontaneously without any of these triggers, in which case it’s termed unstable angina, which can mean a near-future heart attack.
Dr. Elefteriades continues, “Every patient feels the (heart) attack differently. Chest pain is nearly ubiquitous, but only a minority of patients have what we call ‘radiation’ to the neck.”
If you’re in the ER for your chest with neck pain, and the blood test (repeated) for heart attack comes back negative each time — this doesn’t mean you’re heart is in the clear.
Chest pain with neck pain is also a possibility with an aortic dissection, which is a life threatening condition.
If this is what’s happening, it will NOT show up on the blood test (troponin) for heart attack.
An aortic dissection can also be missed on a chest X-ray.
An ER doctor will have a high suspicion for an aortic dissection if the patient has also been experiencing fainting or near-fainting episodes, back pain and if the chest pain is described as “ripping” or “tearing.”
An ER doctor should order a CT angiogram to investigate.
Chest and neck pain concurrently can also be caused by an esophageal spasm, which is a non-cardiac issue.
Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Deep, Throbbing Aching Chest Pain: Causes

Chest pain comes in many flavors, so what could it mean if it’s throbbing, deep and aching?
Three very serious conditions can cause what a patient might describe as a throbbing type of pain in the chest, or a sensation of being deep and aching.
Unfortunately, the first three explanations for these symptoms that come to mind for John A. Elefteriades, MD, are far from benign.
Dr. Elefteriades is the William W.L. Glenn Professor of Surgery, and Director, Aortic Institute at Yale-New Haven, New Haven, CT.
Causes of Throbbing, Deep Aching Chest Pain
Dr. Elefteriades explains, “Chest pains or aches can be the result of coronary artery disease, valvular heart disease or aortic aneurysm. The descriptor ‘throbbing’ is uncommon.”
- Coronary artery disease. People can live to 90 or more with this condition. But if you don’t take measures to aggressively manage CAD, it can kill you long before you cash in your first pension check.
- People can live years with valvular heart disease, but it can also kill. The key is treatment, which (as with CAD) may require surgery.
It’s important to point out that there are also benign causes of chest pain or aches, such as non-serious arrhythmias, inflammation of the rib cartilage, and acid reflux disease. Even the side effects of some medications can be a cause.
Aortic Aneurysm: Deadly and Stealthy
What very few people know is that a thoracic aortic aneurysm — though usually not causing any symptoms — can cause a very deep or penetrating chest pain — and quite suddenly.
Shutterstock/Veronika Zakharova
The imaging tests that a doctor will order to examine the heart, such as an X-ray (standard ER procedure) or an ultrasound (echocardiogram) will show the aneurysm.
An aneurysm that is producing symptoms like chest pain or aches can be surgically repaired.
If the bulge in the aorta ruptures, internal hemorrhaging will result. Mortality is high.
Other symptoms with a dissecting aortic aneurysm might be severe shoulder and/or back pain.
Formerly the chief of cardiothoracic surgery at Yale University and Yale New-Haven Hospital, Dr. Elefteriades is working on identifying the genetic mutations responsible for thoracic aortic aneurysms. He is the author of over 400 scientific publications on a wide range of cardiac and thoracic topics.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}