

How Well Can the Deadlift Tone My Entire Body?

The deadlift is a divine way for women to “de-flab” their body and create firm muscle tone from head to toe; and it’s an easy exercise to learn.
First, you need to learn proper form with this “lotsa bang for your buck” compound movement.
The deadlift is a much favored movement among people, including women, who know the importance of acquiring overall body strength.
Though the deadlift is associated with strength and power, it’s also an amazing exercise for toning many areas of your body.
How Do Women Do a Deadlift?
The same way a man performs this exercise. Grab a barbell that’s on the floor, bending the legs to reach it, keeping the shoulders above the hips, an arch in the lower back.

Shutterstock/Tyler Olson
The distance between your feet can vary, depending on what’s most comfortable for you. There can also be variation in the distance between the hands.
Now straighten, keeping the shoulders above the hips AT ALL TIMES, maintaining the lower back arch.
Rise until you’re erect, holding the barbell against the thighs with straight arms. Never round the back.

Shutterstock/SerdyukPhotography
Why does the deadlift tone a woman’s entire body?
Because it works the following muscles: the upper, middle and lower back; butt, hamstrings and calves; thighs and abs; shoulders, biceps and forearms.
That’s practically the entire body.
How Women Can Tone Entire Body with Deadlifts: How much Resistance
Practice first with a very light barbell. I recommend an Olympic bar with no weight, because ultimately, you’ll be wanting to do deadlifts with an Olympic bar because this tool is the one in the “squat rack,” the best place to perform deadlifts.
Squat racks are located where mirrors are. Some gyms have a deadlift station, and these stations fit only an Olympic bar.
As a woman gets stronger she’ll need heavier weights, and it’s just easier to load an Olympic bar than fuss around with removing pre-fixed barbells from their station and returning them.
Women should master the deadlift form before focusing on how much weight to lift.
For women new to the deadlift, use a load that allows 20 clean, solid repetitions; see if you can do this with an unloaded Olympic bar, which is 45 pounds.
When 20 reps feel comfortable, start increasing the resistance over time so that 8-12 repetitions are difficult but not straining.
Finally, hand position in the deadlift can be palms facing you or away.
There’s also the “mixed” grip, which is the most effective. One palm is facing you, and the other palm is facing away.
The mixed grip allows you to lift more than either an all-supinated grip (palms facing away) or all-pronated grip (palms facing you).
Perform this exercise twice a week with two or three days of rest in between. Do five sets with about 90 seconds in between.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Jasminko Ibrakovic

Cardio Workouts for Migraine Headache Sufferers

Here is a cardio workout that will benefit people with migraine headaches.
This cardio workout for migraine headaches is based on a study that showed that those with this condition can, indeed, tolerate certain types of physical activity fairly well.
The study results included that of a lower frequency of the pain occurrence.
What is the cardio exercise mode?
It is that of indoor cycling.
In the study, the exercise sessions on the indoor bikes did not aggravate the symptoms of the study subjects.

Shutterstock/ Seasontime
In the last month of the study, the frequency of migraine headaches dropped considerably.
The intensity of pain also dropped. As a result, the amount of medication taken also was reduced.
“While the optimal amount of exercise for patients with migraine remains unknown, our evaluated program can now be tested further and compared to pharmacological and non-pharmacological treatments to see if exercise can prevent migraine,” says study co-author, Dr. Emma Varkey in the paper.
Cycling indoors seems just what the doctor ordered, as it eliminates most of the jarring or bobbing up and down that occurs with other forms of cardio exercise.
This is one mode of cardio in which a person’s head stays virtually immobile, since the entire upper body is locked nicely in place.
Unfortunately, since exercise historically worsens this unique type of head pain, studies in this realm have been lacking. More research is called for.
Avoiding Exercise Due to Headaches
If you suffer from migraines and, as a result of this, have been avoiding aerobic activity, it’s time to hop on a stationary bike and see what happens.
- Don’t get ahead of yourself by attempting a Spin class as your first session. These classes tend to be intense and loud.
- Start out on a stationary cycle in the cardio section of a gym, or perhaps you can buy a bike for your home.
- Do not get into the habit of reading while pedaling, as this will distract you from being aware of how your body is responding.
- Watching TV while pedaling is actually less distracting than reading, as it’s quite possible to pedal vigorously while viewing a TV screen — whereas trying to maintain a vigorous pace while reading is more difficult.
Sprint Cycling
When I was a personal trainer I instructed my clients how to do sprint cycling, which is another term for high intensity interval training on a stationary bike.
Once you find that pedaling a bike is migraine-friendly, you may want to try sprint cycling — regardless of your body weight.
It’s just a superior way to use a stationary bike; plus, it saves time. Twenty minutes of sprint cycling is far more effective than a whole hour of steady state pedaling.
Here’s how to get started with sprint cycling — also called anaerobic cycling.
Pedaling super fast may jostle the bike somewhat, depending on the machine. If this brings on a headache, slow down or try a different machine.
Find a bike that is more stable on the floor.
If at some point you feel ready for a Spin class, then go for it.
Make sure you’re well-hydrated throughout your exercise, since dehydration can cause headaches.
The study is published in Headache: The Journal of Head and Face Pain.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/B-D-S Piotr Marcinski
Source: sciencedaily.com/releases/2009/03/090326141557.htm

Can Exercise Make You Have Fewer Menopausal Hot Flashes?

Exercise may reduce the number of hot flashes a woman has in the 24 hours following the activity.
This is great news for menopausal women who suffer from sudden waves of feeling overheated and sweating, which can sometimes be drenching.
The perception of hot flashes is more common in overweight and sedentary women.
A Penn State study that was released in 2014, headed by Steriani Elavsky, a specialist in exercise, was formatted so that actual, real hot flashes were accounted for, without the perceived hot flashes interfering with data.
This study focused on exercise, not menopause, and hence, the women in the study (ages 40-59 and not on hormone therapy) were those with mild to moderate symptoms, rather than severe.
The women were divided into groups:
1) normal weight
2) overweight/obese
3) high fit, and
4) low fit.
Hot flashes were recorded with a device on the skin, and the women themselves recorded their hot flashes.
The results showed that fewer flashes were recorded by the skin device following exercise.
The study, along with any current research, does not 100 percent verify that exercise will reduce hot flashes in every single woman.
“Hot flashes are poorly understood, but there are some studies that suggest they may be tied to insulin levels and insulin resistance which tends to occur more frequently when estrogen levels drop – like during menopause,” explains Heather Bartos, MD, a board certified OBGYN, and chief of Obstetrics & Gynecology at Texas Health Presbyterian Hospital in Denton, TX.
“If exercise helps hot flashes it probably helps in the same way it does for diabetics managing their blood sugars. It’s definitely worth a try!”
Exercise, Insulin Levels, Hot Flashes
Exercise, particularly strength training, helps prevent insulin resistance. Insulin resistance is when the uptake of insulin, by insulin receptors on muscle cells, is impaired.

Shutterstock/CandyBox Images
Insulin brings blood sugar to muscle cells for their fuel source. If insulin sensitivity is improved via exercise, this may somehow lead to reduced hot flashes in the 24 hours following the workout.
Working out will never make you have MORE or longer hot flashes.
If you have a hot flash while in your spin class or jogging on a treadmill, this is a coincidence!
The hot flash may seem worse than usual — but that’s because your body is already warmed up and sweating from exertion — in an enviroment that may not have optimal ventilation.
 Dr. Bartos served as an assistant clinical professor of OBGYN at the Uniformed Services University of Health Sciences for several years and was a physician in the U.S. Navy for eight years.
Dr. Bartos served as an assistant clinical professor of OBGYN at the Uniformed Services University of Health Sciences for several years and was a physician in the U.S. Navy for eight years.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2012/06/120627122254.htm

5 Shocking Reasons You Can’t Shrink that Fat Stomach

Why aren’t you able to get rid of that belly fat?
What’s preventing this? You may not be the problem. Here are 5 shocking reasons the fat stays:
Belly fat that won’t go away is frustrating to deal with and even look at, but there are reasons it continues to stick around.
Some people feel bad about their belly fat and blame themselves, even though they’ve truly tried very hard to make it go away.
It may not be your fault, so don’t feel bad. Once you understand the reasons behind the problem you may be able to finally get the kind of toned abs you’ve dreamt of.
Often, belly fat won’t go away because of cortisol.
Cortisol is the infamous stress hormone that promotes excess fat storage in the midsection.
This gives you one more reason not to let thing stress you out. Cortisol is your emergency response hormone that is part of you fight or flight instincts.
There are more cortisol receptors in the abdominal area than elsewhere.
You might be shocked to learn that cortisol will actually extract fat from other parts of your body and deposit it into your midsection.
It could be a hernia, and not just belly fat that won’t go away.
Hernia can easily be mistaken for belly fat, especially if there aren’t any other symptoms.
While some suffer pain from their hernia, it’s not uncommon for the condition to be painless.
Hernia is actually a protrusion of an organ through the lining that would normally contain it.
While hernia in men is most commonly talked about, women can get abdominal hernia too.
High insulin can make fat in the stomach stubborn.
The main purpose of insulin is to take blood sugar and store it as fat. Producing too much insulin can cause a person to be overweight, or at least have a flabby looking midsection.
While some would argue that they’ve reduced their sugar intake for the sake of dieting, remember that there are many healthy foods that contain natural sugars, or have elements that convert into sugar during the digestive process.
Genetics can cause the retention of fat in the abdomen.
Genetics should not be used as an excuse, but it is the reason why some people have a hard time getting rid of belly fat. It’s really all about the fat distribution.
Those who inherited an apple-shaped body will have a harder time slimming down their midsection.
Menopause is often why belly fat won’t go away in women.
Fat caused by hormones can prove to be the hardest to get rid of.
The hormonal imbalance of estrogen during menopause results in increased amounts of belly girth.
While there may be some very shocking reasons you can’t seem to get rid of the belly fat, they only serve to make it stubborn, not permanent.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Paulus Rusyanto/dreamstime

How to Avoid Chest Pain while Bar, Bench Dipping

Chest pain from bar or bench dipping can be quite intense, or mild, or anything in between.
Though chest pain, in general, can be frightening, since it calls to mind the idea of having a heart attack, chest pain that occurs during dipping, or right after you complete a set of this exercise, is very much most likely caused by strain on soft tissue, rather than strain on your heart.
In fact, though a set of dips on a bar or bench can be made to be very grueling, it actually doesn’t place all that much stress on the heart.
I find that after performing highly intense sets of dips with significant weight loads, my heart rate is only minimally elevated at the conclusion.
To help avoid chest pain from bench or bar dips, here are guidelines.
Warm up properly.
I don’t treat dips as a warm-up any more than I treat bench press or deadlifts as a warm-up.
To me, this multi-joint triceps routine is as real a compound weight routine as are bench press and chin-ups.
My warm-up here is a shoulder routine, and even that has a warm-up.
Though dipping is primarily a triceps exercise, it taxes the shoulder joints, so before bench dips, I do a set of lateral raises.

GeorgeStepanek/creativecommons
This really warms up the shoulder joints including the rotator cuff, which gets hit during dips.
Any shoulder routine will do for a nice warm-up, or, if you prefer, warm up with a chest exercise.
This may be better for people who get chest pain from dips. A cold, stiff chest is more likely to be strained during dipping, than is a chest that’s warmed up with prior pressing motions.
And of course, do bodyweight-only dips before you do your heavier sets of this exercise.
If your heaviest bar dips are bodyweight-only, then do a few sets with your feet assisting; or, do seated (bench) dips as the warm-up.

Freepik.com
Some chest stretching motions will also be a good idea, and these can be done in between dip sets.
Control the negative.
Don’t drop down or let gravity assist you when lowering yourself. Control the negative as you would with the negative in a bench press or squat.
Don’t go too deep.

Freepik.com, prostooleh
I always tell my clients not to let their elbows bend more than 90 degrees. Or, to put it another way, don’t let the upper arm go past parallel with the floor.
For very trained individuals, a little past parallel is fine, but don’t overdo it.
Breathe correctly.
Inhale when you lower, and exhale when you push up.
Relax shoulders.
Don’t tense them up. Some people may do this out of nervousness when getting ready to do bar dips, or heavy-weighted bench (seated) dips.
Don’t place hands too far apart.
The further your hands are apart, the more chest muscle fiber is recruited; the more strain on the chest muscle.

Shutterstock/RomarioIen
Placing hands closer together than usual will more target the triceps and will help prevent chest pain during dips.
Don’t get ahead of yourself with increasing weight load with this multi-joint exercise. Yes, it’s so tempting to do this.
But don’t increase the weight load until you can do 12 reps. And then increase it just a little bit.
If none of these tactics work in preventing chest pain from dips, then take a break from this exercise for a few weeks or so, and focus on substitution exercises like very narrow-grip bench press and supine elbow extension with a barbell.
You may have an inflammatory process caused by injured cartilage. If rest still doesn’t combat the problem, see a sports medicine doctor.
If you experience chest pain from exercise in general, see a cardiologist immediately.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Long Femur, Short Torso Squat Myths About Body Proportions

There’s some false beliefs out there about long femurs, short torsos and difficulty with squats that need to be cleared up fast.
It’s bigger than I thought, all this talk about long femurs and short torsos screwing up people’s attempts to perform a halfway decent parallel back squat, let alone a full back squat.
Let’s clear up some myths surrounding the anthropometrics of the long femur to torso ratio and how it relates to breaking parallel in the back squat, as well as just going parallel.
“Tall people necessarily have long femurs.”
Well, yeah, when you consider absolute length. But the whole issue of “long femurs” and the back squat has to do with relative length of the thigh bone to the length of the torso.

Note the exceptional “anthropometrics” here as far as squatting. This man can be any height, including 6-5. Femur length to torso length has nothing to do with overall body height.
People also forget to realize that with the tall person’s long femurs also comes a longer torso, and this typically balances things out.
Sometimes, long thigh bones go with short shin bones, but this ratio won’t interfere much with the back squat if the torso exceeds the length of the thigh bone.
A person can be 7 feet tall and still have a femur that’s much shorter than his torso, and also shorter than his shin bone.
So though the thigh bone is long in the absolute sense, it’s short in the relative sense.
“Disproportionately long femurs occur only in tall people.”
Wrong. Short people can have out of whack femur length to their body height, such as marathon runner John Kagwe (below) who stands 5-6.

Look around at your gym for further proof.
“Short people can’t have relatively long femurs.”
See above.
“People with long femurs can learn to squat upright by developing other efficiencies.”
This is a grey, fuzzy area, because some athletes can squat virtually upright due to femurs much shorter than their torsos.

His femurs appear to be HALF his torso length!
On the other hand, “upright” to many athletes does not mean “vertical.” It means a straight back (not rounded), albeit somewhat leaned forward.
Honing hip and ankle flexibility will allow the long-femur person to lessen the vertical lean, but they will never have what is considered an upright posture during the back squat unless they use a good Sumo stance or heel elevation.
“People with long femurs should avoid doing back squats.”
There’s no reason why they shouldn’t do back squats as long as they execute excellent form and never round their back.
Having longer femurs than the torso is not a handicap (just ask any competitive cyclist, kickboxer or high jumper).
“If the femurs are longer than the torso, this is no excuse to struggle with back squats.”
Yes it is. If you can’t understand why, try this experiment. Sit in a chair at the edge where your thighs are parallel to the floor.
Lean forward and keep an arch in your lower back.
Stop when your shoulders are vertically over your ankles.
No problem, right? This assumes you don’t have “long femurs.”
You shouldn’t be that much leaned forward.
Now, to understand what someone with “long femurs” experiences, imagine that your knees protrude out a few inches more, beyond your shoulders.
This would make your ankles a few inches further from the chair. Thus, in order to align your shoulders over your ankles, you’d have to lean forward more.
Pretend, and lean forward more. And more. Keep your lower back arched.
Can you appreciate what someone with long femurs to torso must go through?
If you’re not really feeling it, then add a few more imaginary inches to your upper legs.
If you have short (relatively!) thigh bones, you may have to imagine six extra inches.
“Those with long femurs that interfere with back squats should wear Oly shoes.”
Unless you’re training for competition in which these shoes are required, there’s no need to spend all the money.
One-inch shoe inserts (targeted to people who want to appear taller) will suffice.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Source: marathonchamps.com/a-JohnKagwe.html

Why Obese Women Can’t Lose Weight on a Treadmill

Just because you haven’t lost weight despite all the time you’ve spent walking on a treadmill doesn’t mean that you can’t change this outcome.
I’ve worked with many heavy women who wanted to lose large amounts of weight, and the treadmill is an inviting mode of exercise.
What I’ve also noticed, in my years of working out at many health clubs, is that almost every obese woman who uses a treadmill…HOLDS ONTO THE MACHINE.
This very act—holding onto the treadmill—is what’s preventing you from losing weight.
Now, if previous to using the machine, you were very sedentary, and then you decided to walk an hour on your new treadmill (or the one at the local gym) every day after work, replacing an hour of TV or computer time, then of course there will be some weight loss.
But have you noticed it only went so far? It stopped after 10 pounds, maybe only five?
Maybe you lost more, but it then halted, and you’ve continued walking that hour, day after day, month after month after month … and the scale has not budged, even though there’s a lot more weight to be lost.
What’s going on? You’re holding on. (If you’ve been swinging your arms and have hardly lost any weight, I’ll explain that soon.)
Obese women who hold onto a treadmill should expect very little weight loss from specifically this exercise.

Shutterstock/ LightField Studios
If they’re also doing intense, compound strength training and sticking to a sensible diet, they’ll lose a good amount of weight.
But the time spent on a treadmill, holding on, will serve almost entirely to waste time or as a social platform to chat with other treadmill users. But don’t count it in as a weight loss station.
Why does holding onto a treadmill sabotage weight loss?
You use far fewer muscles. The act of holding on eliminates most of the workload from the core muscle group.
It also subtracts work from the legs. Don’t be fooled by the calorie display. If you stepped off the machine and let it run empty, the calorie display would continue showing rising numbers!
You may think that an hour a day on a treadmill, even if holding on, amounts to a lot of exercise, but just think about something for a moment:
How can something SO easy melt off excess weight? Yes, you put the time in, but time is meaningless if the workload is meaningless.
In order for the obese woman to force her body to burn fat for fuel, she must add an activity to her baseline that forces her body to adapt.
The activity must shock the body and force it to change. The activity must be easier for a slim body to perform than an obese body.
Holding onto a treadmill does not meet any of these criteria. Put aside all the science of human kinetics, kinetic chains, gait patterns, biomechanics and all the other mumbo-jumbo, and repeat to yourself these four simple words: YOU ARE HOLDING ON.
Say these words enough and you’ll soon have powerful insight into why this sabotages the weight loss plan.
What is the obese woman’s baseline?
That’s the level of activity your body is used to, that it’s adapted to and efficient at.
This includes the normal walking you do in day-to-day life (on the job, at stores, around the house).
If you step onto a treadmill, only to hold on while your feet glide along with the moving tread…you’ve just taken yourself a notch BELOW your baseline.
This is because your baseline consists of walking around without holding onto anything for support (on the job, at stores, around the house).
A downgrade in baseline! Repeat that: a downgrade in baseline activity!
You may still rationalize by thinking, “Well, at least it’s more activity than sitting in front of the TV.” Yes, it is, you’re correct.
But is it enough to accomplish your weight loss goal? No, no, no.
Do you want to simply make comparisons to the energy expenditure of watching TV? Or do you want to lose a large amount of weight?
How can an obese woman lose weight with a treadmill?
Take your hands off the treadmill and walk at a pace that your body is not used to. This will put you ABOVE your baseline.

Shutterstock/ Ljupco Smokovski
Your body will go, “Hey! What’s going on here?” It will be forced to adapt. Forced adaptation raises your body’s energy needs. Translation: weight loss!
Make the session challenging. You should be breathing heavily, and hot and sweaty. It should be uncomfortable. This will force adaptation. Your body will dip into fat stores to accommodate this new demand.
Keep your hands off the treadmill!
- Don’t go setting the incline at 15 percent and the speed at 3 mph, and then say you can’t walk without holding on.
- Settings like this are far beyond your capacity.
- Be realistic.
- Even 2 mph at 15 percent, sustained, is pretty stiff.
Obese women who haven’t lost weight with the treadmill must remove their hands from the machine.
If you’ve already been swinging your arms and have not lost much weight…increase the speed and/or incline to force more adaptation—but no matter what you do—swing your arms.
Hold on only to steady yourself while drinking water, taking heart rate or changing the settings.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Creativa Images

What Does a Tiny Dark Spot in a Mole Mean?

Can a small dark spot inside a mole possibly mean melanoma?
Unfortunately, the answer is YES — it can be an early sign of this deadly skin cancer that can sneak up on people.
“Any area of excess pigmentation in an existing mole can be an early sign of skin cancer,” says Dr. Rebecca Tung, MD, a
“Similarly focal bleeding or scabbing can also be worrisome signs that a mole is undergoing malignant change.
“Getting this mole looked at by a dermatologist would be a good idea to find out whether or not the mole is okay or not.”
You should have a dermatologist check your skin, including your scalp, on an annual basis. Even if your primary care specialist performs a skin check, they don’t have the training that a dermatologist has.
What to Do
Ideally, have both your primary care doctor and dermatologist perform the clinical skin exam, because two pairs of medical eyes are always better than one pair.
The doctor will not only check all throughout your scalp, but on the soles of your feet and between your toes.
Request that your dermatologist use a “dermatoscope,” sometimes also called a dermascope.
This device provides lighting and magnification, enabling the doctor to get a much more detailed look at moles and other spots on your skin.
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/metamorworks

Small Moles Growing Together: Melanoma or Benign?

Here’s what a dermatologist says about small moles growing together and the possibility of melanoma.
“Sometimes a normal existing mole (round and regular in shape) may seem to morph into a larger, irregular lesion,” says Dr. Rebecca Tung, MD, a
Dr. Tung explains, “There are a few possible scenarios that may be in play:
“1. The mole may have undergone change into an atypical (dysplastic) mole or even skin cancer (melanoma).
“2. Sometimes adjacent freckles grow darker with sun exposure and seem to join up with a nearby mole.
“In either case, it is a good idea to have that concerning mole checked out by a dermatologist.
“He or she will examine the spot visually, and possibly with a special instrument that magnifies called a dermatoscope.
“If the lesion looks suspicious, a skin biopsy may be recommended to view the cells and architecture of the skin under the microscope.”
When in doubt, have it checked out.
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/LightField Studios
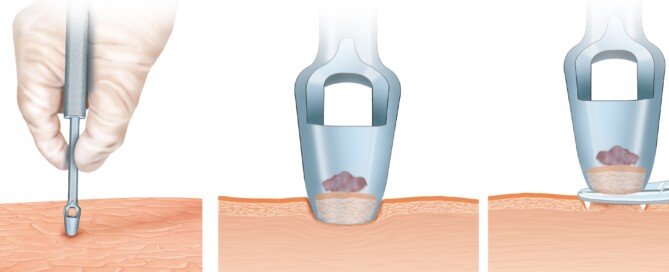
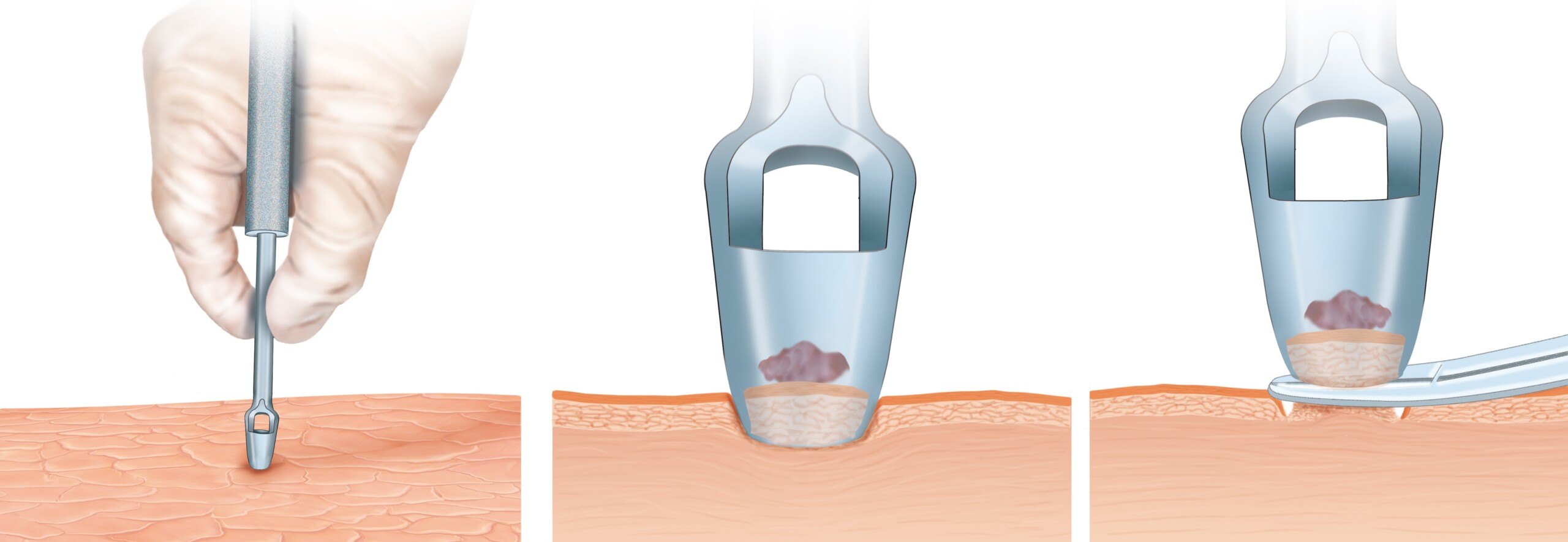
Punch Biopsy for a Mildly Atypical Mole
What does a dermatologist think about a punch biopsy for a mole that’s slightly atypical?
An “atypical” mole means it’s more likely to morph into melanoma than is a typical mole.
“A suspicious mole can be biopsied (sampled) in a variety of ways: a punch biopsy, shave biopsy or excision,” says Dr. Rebecca Tung, MD, a
“After the skin is numbed with local anesthetic, the lesion in question can be removed with a circular scalpel (punch biopsy) and closed with a stitch or two.
“If the mole seems more superficial, a special scalpel called a dermablade can be used to remove the mole.
“Alternatively, if a deeper biopsy is needed or the doctor wants to remove the lesion entirely, an excision (removal with a scalpel needing stitches) may be suggested.
“Regardless of how the biopsy is performed, the intent is to make sure the spot is not skin cancer.”
Make an appointment with a dermatologist to have a full skin exam. Ask the doctor to point out any moles that appear to be atypical.
Keep a close eye on them as well as for any new or changing spots on your skin.
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}