

Strip Off Belly Fat: Cardio Exercise or Lifting Weights?

If you want to lose stomach fat and had to choose between cardio or lifting weights, which should you choose?
According to a Duke University Medical Center study, cardio wins for reducing belly size. But there’s probably a huge catch — which I’ll get to shortly.
The fatty tissue at issue here is that of visceral and liver; it’s deep within your abdominal cavity and raises the risk for heart disease and type 2 diabetes.
“Our study sought to identify the most effective form of exercise to get rid of that unhealthy fat,” says Duke University exercise physiologist Cris Slentz, Ph.D., the study’s lead author, in the report.
The study showed that to lose stomach fat, aerobics was actually more effective than lifting weights.
Lifting weights (strength training), according to the study, resulted in no significant results for midsection shrinkage.
Surprisingly, a combination of cardio and weight lifting to lose stomach fat didn’t make much of a difference when compared to just the cardio alone.
Slentz explains, “Resistance training is great for improving strength and increasing lean body mass, but if you are overweight, and you want to lose belly fat, aerobic exercise is the better choice because it burns more calories.”
These results beg the question: What KIND of strength training did the subjects undergo?
The study summary doesn’t mention this. However, what’s really telling is that the subjects were overweight and sedentary.
This tells me that they most likely performed single-joint, “isolation” exercises at submaximal intensity — perhaps at the moderate level range of effort.
In short, it is extremely unlikely that out-of-shape, inactive people, who have no experience with lifting weights, did intense sets of deadlifts, barbell squats and bench presses for a stomach weight loss study.
For the Duke study, there were three groups: cardio, weight lifting, and a combination.
The cardio group did the equivalent of 12 miles of jogging a week, 80 percent max heart rate. The weight lifting group did three sets of 8-12 repetitions, three times a week.
To lose stomach fat: the big questions:
- Were these sets taken to muscle failure?
- Or even near muscle failure?
- Or were the sets only of moderate challenge?
- Did they use light, medium or heavy resistance?
- How much rest was taken in between sets?
- Were these triceps kickbacks or barbell presses?
- Arm curls or lat pull-downs?
There are many possibilities here, and all influence how many calories are burned – during, and after, the workouts.
Was the strength training intense enough to keep resting metabolic rate elevated for hours after the workout?
Was the weight lifting protocol conducive to elevating the body’s release of human growth hormone and testosterone – two very powerful fat-burning chemicals? Something tells me a big fat “No.”
To lose stomach fat, strength training with compound routines, done intensely, will blast off more stored energy than cardio that equates to 12 miles of jogging a week at 80 percent max heart rate.

Freepik.com/pressfoto
Intense weight lifting, focusing on the “big lifts” like squats, leg presses, deadlifts, chest presses, pull-ups and rows, will burn significant amounts of stomach fat (and blub all over).

George Stepanek, CreativeCommons
I have seen this in my own clients. So what should be the final verdict when it comes to how to best lose stomach fat?
To lose stomach fat in the most effective way, do both cardio and lifting weights.
But if you’re a novice at strength training, I don’t recommend you attempt heavy, intense deadlifts or heavy squats.
A beginner who wishes to lose stomach fat needs to build up some conditioning and joint integrity before tackling intense, heavy compound routines.

Jasminko Ibrakovic
So to lose stomach fat, begin your journey by doing compound routines with light weights.
To lose stomach fat most successfully, increase weight as you get stronger and keep pushing.
Add cardio to that and you have a winning combination to lose stomach fat.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Sinelev
Fat-Burning Cardio Exercises You Can Do with Sprained Ankle

Don’t let a sprained ankle stop you from doing cardio exercise that burns fat.
First of all, make sure your sprained ankle is only that; no broken bones.
Make sure it is securely stabilized with a compression bandage. Compression bandages expedite healing of this injury.
Obviously, the cardio exercise that comes to mind for people with sprained ankles is the stationary bike, but there are other cardio modalities as well, and I’ll get to those shortly.
I’m a former personal trainer who’s had her share of sprained ankles.
I never let my sprained ankles stop me from doing aerobic exercise, and you shouldn’t either.
Pedaling Machines: Do HIIT
When using the stationary bike, if possible, strap both feet into the pedals, and employ a fat-burning technique known as high intensity interval training.
It’s possible to use an elliptical machine while recovering from an injured ankle — but keep the injured foot flat on the pedal pad at all times. Again, employ the fat-burning technique of HIIT.

The elliptical machine. Freepik.com/jcomp
Note: If at any time, a cardio routine starts aggravating your sprained ankle, stop the exercise.
The cardio exercises mentioned in this article have the potential to allow you to work out, without aggravating your injured foot.
Another fat-burning, cardio-based exercise you can do without compromising your ankle is that of standing in place and socking away at a heavy bag.
Make sure your ankle is securely taped and, ideally, in a brace. Of course, stop if your foot begins hurting.

Shutterstock/Dmitry Kalinovsky
If you know how to deliver punches, believe me, this will definitely count as cardio exercise and burn fat: hooks, crosses and uppercuts, as hard as you can and/or as quickly as you can, will elevate the heart rate and burn fat.
Ever see people sitting on the floor in a machine and rowing? This is safe for sprained ankles and will have a cardio effect.

Cardio rowing machine. Freepik.com/pressfoto
Rowing machines have adjustable settings; find the settings that will get your heart really pumping and your breathing going, and this will burn fat.
“Pedaling and rowing with a taped/braced ankle is safe, as long as the individual knows to exercise up to his/her tolerance level,” says Dr. Bruce Pinker, DPM, who specializes in sports medicine and surgery of the foot and ankle.
“Meaning, if the ankle becomes painful, he/she may need to slow down or stop.”
Always ice your sprained ankle after any kind of workout, and for a total of three or four times a day, 20 minutes maximum.
And remember, if there is any pain while exercising, stop immediately.
 Dr. Pinker is with Progressive Foot Care, which provides state-of-the-art, full diagnostic testing and treatment of the foot. He’s a professional foot and ankle health and wellness speaker who delivers many original seminars annually such as “Keep On Running.”
Dr. Pinker is with Progressive Foot Care, which provides state-of-the-art, full diagnostic testing and treatment of the foot. He’s a professional foot and ankle health and wellness speaker who delivers many original seminars annually such as “Keep On Running.”
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/fongbeerredhot

Best Organic Chocolate Milk: Promised Land, Horizon or Organic Valley?

Which brand of organic chocolate milk tastes the best? There are three popular “natural” brands that are sold at Whole Foods.
One is Horizon Organic. One is Organic Valley. And the other is Promised Land Midnight Chocolate Reduced Fat 2 % Milk.
However, there is no organic label on the Promised Land milk, but I’m including it here because they use hormone-free cows.
By far, the best tasting of these milks is the Promised Land. I am not kidding.
Both Horizon Organic and Organic Valley (at least the reduced fat varieties; I didn’t try the full fat varieties) leave a very unpleasant aftertaste.
The milk comes in a carton for these two brands, and I had briefly speculated that perhaps the milk was picking up some cardboard residue from the carton, causing the miserable aftertaste.
But if this is true, then how come I never detect any aftertaste in white milk by the same brands?
So I ruled out the carton. It’s the chocolate milk itself. The initial taste is okay. Nothing great. And then the aftertaste hits you.
Now, when you drink the Promised Land Midnight Chocolate, WOW! The flavor is much richer than the Organic Valley and Horizon Organic.
There is just no comparison. In fact, Organic Valley and Horizon Organic taste identical, both having the same aftertaste.
Promised Land Midnight Chocolate was previously sold in glass bottles, and now the bottles are plastic, and I’m telling you, THIS is the chocolate milk for health-conscious people.
Though it’s not organic, it’s still hormone free, and besides, if you’re hell-bent on drinking only organic chocolate milk, you just won’t get the same cocoa flavor experience with the organic brands, and the aftertaste is a complete turn-off.
It wasn’t a bad batch, either, because I purchased both cartooned brands on several occasions, initially thinking it’s just a bad batch. But each time, that aftertaste was there. Forget it.
The interesting thing about Promised Land is that their 2 percent variety actually tastes more chocolaty than the full fat version.
If you’re a true chocoholic like me, you’ll want to add chocolate syrup to the Promised Land Midnight chocolate milk, and Whole Foods sells organic chocolate syrup.
Go one step further and add chocolate ice cream! Now THAT’S a REAL chocolate milkshake!
While I’m at it, Promised Land Midnight also beats the taste of conventional chocolate milks sold at regular grocery stores, hands down.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Best Hot Chocolate Mix in the World: Silly Farms

Don’t let the name fool you: Silly Farms hot chocolate mix (there are several varieties) is absolutely the best tasting hot chocolate mix you’ll ever find.
I discovered Silly Farms hot chocolate mix at Whole Foods one day, and was attracted to the glass milk jug bottle.
Of course, I’m smarter than to buy a product based on its packaging, but I’ll admit, the compact glass bottle was inviting, and the chocolate powder was visible. I couldn’t say no.
I’m glad I fell for the packaging gimmick because this hot chocolate was the best I had ever tasted in my entire chocoholic life. Silly Farms makes three hot chocolate flavors: “chocolate chocolate,” “chocolate mousse” and “chocolate marshmallow.”
I’ve tried only the first two (don’t care for marshmallows), and I don’t know if there’s any difference in taste, but Silly Farms is now No. 1 on my list as to who makes the best hot chocolate mix.
Now, here is what I do not understand: the ingredients. I have the ingredients tag for only the “chocolate chocolate,” but I’m sure that these ingredients are pretty similar to those of the other flavors.
The ingredients are as follows: natural cane sugar, Dutch processed cocoa (with alkalai), and natural vanilla powder.
That’s it. I expected a bunch of scary ingredients to make this product taste so good. So I’m stunned that this is all there is.
I assume that maybe the “natural vanilla powder” is what gives this product its kick, but the kick is a rich chocolate flavor. So I don’t know how anything vanilla can produce this result.
Now, get this: The stated serving size is only two teaspoons! Come on, who takes only two teaspoons for hot chocolate?
Silly Farms, like just about every food company out there, uses the gimmick of crazy-small serving sizes to create the illusion that the product isn’t that caloric or fattening.
Well, I can’t be fooled by this age-old trick. Two teaspoons of this wonderful powder is 80 calories. I use four TABLEspoons per 8 ounces of hot milk – and that’s a minimum.
Total fat in the two teaspoons is 1.5 grams. One of those grams is saturated. Total carbs is 17 grams. Dietary fiber is one gram, and sugar is 17 grams.
The time to be health conscious is not when you’re drinking hot chocolate. However, I am very pleased that Silly Farms doesn’t add soy to their product. That’s what I was worried about. Thank goodness it’s free of soy – at least according to the label.
The caveat with Silly Farms hot chocolate mix is the shape of the bottle. It looks great on the shelf, but in terms of practicality, it misses. The opening is very small, like a classic glass milk bottle, and the bottle gets wider towards the bottom.
My tablespoon will not fit into the opening. So I must pour the powder into my tablespoon to get the amount just right for my taste preference.
The powder often “sticks,” so what happens is that nothing comes out. I shake a little harder and wham, a pile plops out.
Thus, I must do this over a plate to catch the excess powder.
But this won’t stop me from buying the best hot chocolate mix in the world.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Will Daily Aspirin Help Prevent a Stress Heart Attack?

It seems logical that a chronically stressed person could benefit from a daily aspirin in terms of helping prevent a heart attack, since aspirin is a blood thinner and stress thickens blood.
I wondered about this, so I asked a cardiologist if a healthy person under persistent stress should take that daily aspirin.
“It really depends on the risk factors of the patient,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
“For the reduction of myocardial infarctions [heart attacks] in men between 45-79, it is recommended if any of the risk factors exist: diabetes, hypertension, smoking, high cholesterol.
“For women between 55-79 there is no data to support primary prevention and aspirin use for myocardial infarction.
“There is an associated reduction in ischemic strokes if any of the following risk factors exist: atrial fibrillation, hypertension, smoking, diabetes, left ventricular hypertrophy.
“Taking baby aspirin in the absence of any risk factors probably doesn’t prevent a primary event, but may increase risk of GI bleeding.”
Chronic stress makes the blood thicker and stickier.
This is because the body, when faced with persistent anxiety, “thinks” that a threatening event is imminent.
Should the body get gashed in a fight or flee situation, thick, sticky blood will clot a lot faster than thinner blood—preventing a fatal hemorrhage!
The intense exertion of a fight or escape from the threat produces hormones that reverse this thickening.
However, for most people, that fight or flight is not possible (e.g., being trapped in a stressful job all day long). Thus, the blood remains chronically thickened—more likely to form clots…and one of these can form in the heart…
However, Dr. Stevens-Cohen explains, “In the average patient, even a patient who leads a very stressful life, there is no benefit to taking a baby aspirin in preventing MI.
“The studies simply don’t support it. While it may not be harmful, it is not considered protective at this time.
“When I was a resident, every patient with one or more cardiac risk factors was placed on ASA 81 mg for MI prevention (let’s forget stroke for now).
“Then studies were released showing that the incidence of MI was actually similar in patients taking ASA vs. not in this population.
“Keeping in mind, this study population had cardiac risk factors and there was no benefit (in particular with women).
“So now, let’s lower the threshold and say no risk factors at all in a heart healthy patient with chronic stress. There is no evidence to support daily aspirin would be protective.
Chronic stress may lead to anxiety, variations in blood pressure, lack of sleep and overall decrease in general health.
“Targeting the specific pathology that impacts a patient’s life may be more beneficial than generic baby aspirin for all.”

Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Mole with New Black Specks May Not Be Melanoma
Here’s a benign explanation for why you see new black spots in your mole that weren’t there before.
Before I give this explanation, you should know that the new appearance of black in a pre-existing mole can mean melanoma.
However, don’t panic yet if you’ve discovered a new black spot or speck or two in a pre-existing mole.
This is what happened to me. I have a prominent mole on my shin — prominent in that it’s obvious, a medium dark brown and extremely easy to closely inspect, due to its location.
One day I looked at it and saw three tiny specks of black that were not always there.
I lightly rubbed my finger on it to see if the spots might come off, since I supposed that it was some kind of dirt.
But they remained in place. This was pretty scary. Everything else, however, about the mole, appeared unchanged.
I then shaved my legs. I lightly grazed the razor up my entire shin, over the mole just once (very lightly at this point), in the manner that I’ve always done.
Then I rinsed the cream off and let my leg dry. I then inspected the mole: The black spots were completely GONE.
Does this mean I shaved off the part that was melanoma?
Or could it have been very tiny fibers from the black sweat pants that I had slept in overnight, that I had taken off before inspecting my legs?
I had a visit already scheduled later that day with a dermatologist, for my third serial digital dermoscopy appointment.
This is a teaching hospital, so the first person to examine me was a dermatology resident.
I told him about the mole.
He examined it with a dermatoscope and said it looked benign, that the “reticular pattern” was normal.
Then, the actual dermatologist said it looked normal.
I already had nine moles in the hospital’s digital dermoscopy database, but they decided to include this mole as well.
The computer analysis showed that it was normal. In fact, the doctor told me I could wait two years before coming in again because everything was “so stable.”
How would minute fibers from my black sweat pants or any black micro-debris just happen to find their way into a single mole?
“If a mole has black specks on the surface that easily wash off, this should not be of concern for melanoma,” says Emily de Golian, MD, a board certified dermatologist with Forefront Dermatology in Atlanta, GA.
“Just like any other location on the skin, dirt may adhere to a mole and is easily removed with soap and water.
“If, however, dried blood [which can appear as black specks] is present on the surface of a mole, the mole should be evaluated by a board certified dermatologist.
“Moles may bleed due to trauma, which is not inherently bad, but if a mole has developed spontaneous bleeding, this could be a sign that the mole cells are atypical and need to be removed.
“Dried blood will often appear red or dark red when moistened and removed with a white towel or tissue, so this may help distinguish what type of substance is being removed from the mole surface.”
I had not checked the skin elsewhere on my legs for any fibers, so for all I know, they were elsewhere, and would have been difficult to spot without getting close up, and impossible to spot on the back of my legs. But fibers can get anywhere.
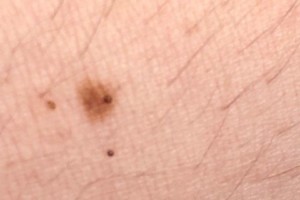
Irritated Mole Quickly Develops Black Spot
The image at the very top of this article shows a mole that rapidly developed a dark spot in it.
The cause was aggressive rubbing with a finger to see if a slightly darker area on the left was dirt (which it turned out wasn’t).
My aggressive rubbing irritated the mole plus the surrounding skin, resulting in three dark specks (tiny skin bleeds).
These tiny scabs persisted for a few weeks.
Below is the same mole, but the dark speck that had been in it had become dislodged and ended up loosely sitting on the skin next to it. The two other specks eventually fell off as well.

If you notice new black specks or spots in a mole, don’t try to pick them off. And don’t panic.
Take a normal shower and see if the water rinses them away.
If not, wait several more days to even a few weeks to see if they just naturally fall out. If they don’t, see a dermatologist.
 Dr. de Golian focuses on the surgical treatment of skin cancer via Mohs surgery, cutaneous oncology (melanoma and basal cell carcinoma), surgical defect reconstruction and cosmetic dermatology.
Dr. de Golian focuses on the surgical treatment of skin cancer via Mohs surgery, cutaneous oncology (melanoma and basal cell carcinoma), surgical defect reconstruction and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Convincing Someone Who Denies Depression to Stay on Antidepressant

Do you know a very depressed person who doesn’t think they are depressed?
You’d think that of all mental illnesses, depression would be the one that the patient is well-aware of.
But in the case of my mother, she was in denial, or at the most, attributed her profound depression to “the pain,” that is, pain from carpal tunnel syndrome!
My mother had a bad case of carpal tunnel syndrome in both hands, but her depression symptoms were alive and kicking well before the carpal tunnel syndrome began making its grand entrance, and the depression symptoms continued well-after carpal tunnel surgery.
However, if you have joint or nerve pain, clinical depression can amplify your perception of it.
My mother refused to try an antidepressant, and my father, oddly enough, felt the same way.
After six weeks, I finally convinced him that my mother needed an antidepressant, and that evening, my mother took her first antidepressant. The next morning she awakened feeling wonderful, and no longer did her whole body hurt.
Pre-antidepressant, my mother often said, “I’m depressed about all this pain,” but then would become teary-eyed over trivial issues.
Carpal tunnel syndrome doesn’t make you sob spontaneously throughout the day or want to stay in bed all day.
Major depression does. And I told her that — both pre-antidepressant and post-antidepressant.
Despite the antidepressant’s marvelous effect, she continued insisting that she didn’t have clinical depression.
It’s important that a person with depression have insight into their situation, rather than deny it. Otherwise, they won’t be as amenable to treatment.
I explained to my mother numerous times that her depression was present before the pain from the carpal tunnel syndrome developed, and before her shoulder pain developed, and that physical pain that’s localized would not make her completely shut down, lose interest in things that were once pleasurable, and have feelings of wanting to go off into the woods and die. “Only depression can do that,” I’d say.
I’d continue: “Since you’ve been taking this antidepressant, you’ve had no complaints of your whole body hurting. That’s all disappeared since you’ve been on Cymbalta. The drug has suppressed your perception of your shoulder pain, which is why you no longer cry when you have a pain attack.”
Several times my mother wanted to go off the antidepressant, but I kept reminding her about the key points:
“The reason you feel so good now is because you’re ON the drug. You have to stay on it until everything blows over, until you are completely out of the woods. It’s helping you through all of this.”
Keep reminding your depressed loved-one: “The reason you feel so good is because of the antidepressant. The drug is working. Go off it and you’ll relapse.”
My mother found it hard to believe that if she stopped taking the antidepressant, she wouldn’t continue feeling so good.
If your depressed loved-one announces they’re ready to stop taking their antidepressant, and they haven’t been on it for long, and any stressors that triggered or aggravated their depression are still present — then never be afraid to tell him or her the raw truth:
“If you stop taking the drug, you will relapse. You will sink back into that ugly dark hole and your entire body will feel crummy all over again. You’ll be crying and feeling like you’re dying.
“You won’t know how to smile or feel joy. Think of how wretched and miserable you felt before you began taking the antidepressant.
“You’ll return to that hell hole if you stop taking the drug. You absolutely must stay on this medication for a while, and then when everything blows over and you’re stabilized, THEN we will get you off of it. Trust me.”
This kind of talk sunk a little more into my mother with each time I gave it. Eventually, she was diagnosed with hypothyroidism, and must take a thyroxine pill every morning.
All evidence points to the depression being secondary to the hypothyroidism. An underactive thyroid can cause many symptoms including clinical depression.
My mother lost weight because the depression minced her appetite; suffered hair loss; and often complained of feeling cold even though everyone else felt fine — and nobody picked up that these two latter symptoms suggested early hypothyroidism.
And then the depression swept in with a 1-2 punch, even though there were subtle signs of its beginning for weeks beforehand.
“I feel so great now,” my mother told my brother, after being on the thyroxine for a while, and still taking the antidepressant, “that I no longer need these drugs. Why can’t I stop taking them?”
My brother responded: “The reason you feel so great is because you are taking two medications: thyroxine and Cymbalta. If you stop taking them, you’ll go back to square one, and it may take a whole week to get you back to where you are now. The reason you feel so good is because you are on two medications.”
At that point, my mother finally realized that she needed to stay on the antidepressant for a little while longer, and that the thyroxine pill will be very long-term.
Because it’s apparent that the depression is secondary to the hypothyroidism, and because the thyroxine’s effects are now fully kicked in, my mother is now in the process of tapering off the antidepressant, which eventually was switched to Effexor due to an insurance coverage change.
(Original publication date: January 2010)
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: freepik

Minimize Daily Hair Fall: 8 Hacks to Prevent Hair Loss

Simply changing the way you do things in your daily life will minimize hair loss.
Use Your Fingertips
The first way to reduce the number of hairs that fall out of your head every day is to use the pads of your fingertips—not your nails—to wash your hair.
Though rubbing in good with your fingernails feels great, the sharp edge of fingernails can tear hair out of its follicles.
The soft pads of your fingertips will be gentler to the roots. And don’t rub and scrub; instead, massage and caress.
I might add that hairs will be needlessly pulled out as you wash your hair if you have the slightest hang nail. Make sure your nails are filed smooth before washing your hair.
A nail need not be hanging to yank a hair out of its root. Check your nails before washing so that they don’t snag any strands.
Wringing out Water
When it’s time to wring the excess water out, do not wring close to your scalp. Grab the hair further away, then wring below that point.
How to Use a Towel
Do not rub your scalp with the towel. Simply place the towel over it and press your hands to it firmly for several moments, then wrap it up.
Charging Your Phone
Be very aware of little things that can cause needless loss of hairs.
Recently I was placing the charger into my cell phone, and a strand of hair somehow got between the charger connector and the insertion point in the phone.
As I inserted, the strand was yanked out of its root. I know that’s only one strand, but little ridiculous things like this every day add up.
Removing Bobby Pins and Clips
To minimize hair loss, carefully and patiently remove clips, bobby pins and any other gadget or trinket in your hair.
Make sure that the tips of bobby pins are smooth and round. Not all bobby pins are alike.
Some bobby pins are very difficult to remove without taking some strands with them.
Scarves, Hats, Etc.
When removing something from your head (ear muffs, hats, bandanas, anything), remove slowly and carefully.
If some strands begin getting yanked, you’ll have time to reverse this situation if you remove the item in very slow motion.
Scalp Itching
Be very cognizant of mindless scalp scratching throughout the day.
When scratching, do not use your fingernail. Instead, gently massage the itchy part with the pad of a fingertip.
Lying Down
Never lie down with a part going down the center of the back of your head.
If your head is against something while your body is horizontal or even slightly elevated, this will tend to pull the strands in the direction that the parting makes them go in.
In other words, if you’re wearing pig-tails, do not take a nap in them, let alone go to bed with them still in. You’ll even feel the pulling if you do.
There are other ways yet to minimize daily hair loss, but I thought I’d provide less commonly-written-about tips that you don’t normally come across.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, Ronald Plett

Common Cause of Cardiac Arrest: Pulmonary Embolism

Far more people die every year from a pulmonary embolism than you think.
These blood clots in the lungs may cause cardiac arrest, and often, the cause of death is listed as just that—cardiac arrest.
When a person dies, their heart stops.
When a person’s heart stops, they die (when they can’t be resuscitated, of course).
But what causes cardiac arrest?
In many cases, it’s a pulmonary embolism — a most unrecognized lethal medical condition.
“Yes, it is often an unrecognized killer, frequently because the picture may be dominated by coexisting conditions such as those that are associated with slowing of blood flow to many parts of the body, especially the veins of the lower extremities,” says Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths and Tricks: A Physician’s Advice.”
Dr. Tavel continues, “The variety of predisposing conditions can include debilitating diseases forcing prolonged bed rest, post-surgical states and congestive heart failure.”
A pulmonary embolism originates from a blood clot in a vein (usually in the lower leg, but it can also be behind the knee, the upper leg or pelvic area).
Every year in the U.S., 60,000 to 100,000 people die from a PE
In about one-fourth of all cases, sudden death is the first symptom.

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/8photo
Source: cdc.gov/ncbddd/dvt/data.html

PVCs: DANGEROUS or BENIGN? LOOMING HEART ATTACK or NOTHING?

PVC stands for premature ventricular contraction.
It creates the illusion of an extra heartbeat, especially if there are two or three in a row.
And sometimes, it feels as though the heart has skipped a beat. This makes some people believe they’re about to have a heart attack.
Frequent premature contractions can produce tremendous anxiety.
“A PVC is a premature ventricular contraction, which means the beat is originating in the ventricle, not the atria (normal site of origin),” explains Yaser Elnahar, MD, a cardiologist with Hunterdon Cardiovascular Associates in NJ.
“Rare [occasional] PVC’s are very common and are not dangerous.
“Frequent PVC’s or runs of PVC’s can be very dangerous or even fatal when it becomes ventricular tachycardia.
“If a person has frequent premature ventricular contractions or runs of PVC’s, the cardiologist usually tries to make sure there are no blocked arteries as the cause. If the arteries are fine then we look for other causes.”
Below are links to articles about PVCs with answers from cardiologists.
Do you experience heart palpitations that literally go on for hours?
Does this occur on an almost daily — or even everyday — basis?
Dr. Pilar Cohen discusses the very unnerving nature of daily heart thumps that last hours.
Do you lift weights or do some form of strength training?
If so, have you felt your heart flutter or go ba-boom during a set?
It’s one thing to have heart palpitations prior to a big lift — the anxiety of performing the lift safely, or, the excitement of possibly pulling off your personal best in that deadlift — can make your heart flutter.
But what if you’ve been detecting palpitations in the midst of a weightlifting set? Dr. Ronald Scheib discusses this problem.
Ever notice that sometimes when you have a PVC episode, it makes you cough?
There’s actually a reason for this; it’s not your imagination, and it’s explained by Dr. Sameer Sayeed.
PVCs are frightening because they can make you think you’re about to have a heart attack.
Or, they can make you wonder if your heart’s going to stop beating any moment, and the fluttering is just its way of conking out, kind of like a car engine sputtering before it goes dead.
But let’s get to the bottom of this. Can a premature ventricular contraction cause a heart attack?
Or can a palpitation be a warning that a heart attack is coming?
Dr. David N. Smith discusses PVCs and heart attacks.
 Dr. Elnahar has publications in the Journal of Atrial Fibrillation, the Journal of Clinical Medicine and Research, Reports in Medical Imaging, and more.
Dr. Elnahar has publications in the Journal of Atrial Fibrillation, the Journal of Clinical Medicine and Research, Reports in Medical Imaging, and more.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}