

Can a Changing Mole Be Benign or Is It Always Melanoma?

We’ve been scared by the media about changes in moles, and skin cancer, a la, “If you notice any changes in a mole, see a doctor immediately, as this could mean skin cancer.”
And you should, because ruling out skin cancer is very easy for doctors to do. Usually, a changing mole, or one that appears to have changed, is not skin cancer.
I’m telling you this so that if you notice a changing mole, you don’t panic and think you’ll die.
But again, I stress, if a mole has changed, see a doctor as soon as possible, just to play safe.
The procedure to determine skin cancer is so easy to perform, that there really is no excuse for skipping the doctor appointment. Changes in a mole have a variety of causes.
“Irritated moles commonly change,” says Jason R. Lupton, MD, board certified dermatologist practicing in the San Diego, CA area.
“They may get irritated from clothing, rubbing on waistbands for example, rubbing on surfboards! (common here in San Diego), rubbing on jewelry — these may get irritated and itchy and become red or crusted as a result.”
(A red or “crusting” mole can also be a sign of skin cancer.)
Dr. Lupton continues: “Also, moles in areas like the axilla (underarms) may become irritated form rubbing/friction.
“Moles may become ‘halo nevi’ — these are moles that develop a ring of light color around them. Although most are benign, these should always be evaluated to ensure they are not melanomas.”

Halo nevus (mole)
If you are pregnant, moles may “may become darker or larger as a result of hormonal changes, or from stretching of the skin — due to growth or an enlarging abdomen,” says Dr. Lupton.
“Typically good signs are if multiple moles are getting darker/bigger simultaneously rather than just one particular mole.”
Do you have acne? Dr. Lupton explains, “Patients with acne may have moles that ‘appear’ to change — either from an underlying cyst or pimple that imparts a swelling or redness to the mole temporarily.
“This can be differentiated from a changing mole due to the relatively short time period of change.”
Moles have a life span, and over a long period (years), they may “simply change and evolve over time — become smaller, lighter and some actually seem to disappear.”
Finally, Dr. Lupton says, “Contact causes for ‘mole changes’ are also quite plausible, as certain chemical or caustic contacts may impart irritation or redness to the area, making a mole look different.”
 Dr. Lupton specializes in skin cancer prevention and treatment plus minimally invasive cosmetic procedures including mole removal, skin rejuvenation, wrinkle reduction and acne treatment.
Dr. Lupton specializes in skin cancer prevention and treatment plus minimally invasive cosmetic procedures including mole removal, skin rejuvenation, wrinkle reduction and acne treatment.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/wavebreakmedia

Do the Big Moles on Your Child’s Back Have You Worried?

Lots of big moles on your child’s back can be intimidating to look at.
With all the heightened awareness over the past decade of moles, melanoma and skin cancer, it’s only natural that you’d be unsettled at all the large moles on your child’s back.
Your worry, unfortunately, is not unfounded.
Your fear that one of those weird looking moles on your child’s back might turn into cancer (melanoma) is, unfortunately, legitimate, especially if there is a large number of them.
Leading dermatologist Dr. Joshua Fox discusses moles in children, including big ones on their backs.
Are you worried about all those big moles on your child’s back? Most people are born without “birth marks.”
Research shows that every beach vacation gives rise to a 5 percent increase in the appearance of small moles on a child.
Dr. Fox says, “The development of new moles is of concern, because the higher the number, and the more irregular moles, the greater the risk for developing melanoma, the most dangerous of the skin cancers.”
What about big moles on my child’s back?
Dr. Fox is founder and director of New York and New Jersey-based Advanced Dermatology P.C.
I asked him (for purposes of this article) specifically about large moles all over a child’s back: Does this reflect excessive sun exposure?
My teen nephew has many big, funny-looking moles all over his back, and he is almost always shirtless on summer lake vacations and tropical vacations.
Dermatologists call moles “nevi” (rhymes with Levi, as in Levi jeans), and the singular form of nevi is “nevus.”
Odd looking or atypical nevi are called dysplastic nevi, and they can resemble melanoma. Having dysplastic nevi is a risk factor for melanoma.
Dr. Fox says that most nevi are not worrisome, but as a parent you should monitor your child’s skin for any changes in nevi or new nevi. This will be challenging if your child has a lot of spots, like my nephew.
If your child has a lot of moles on his back or elsewhere, it would be very smart to pursue serial digital dermoscopy as a way of tracking all the nevi.
Relationship between moles on child’s back and sun exposure?

Shutterstock/ Guenter Albers
“Many dysplastic nevi seem to occur in areas in which the child received severe sunburn on one or more occasions,” says Dr. Fox. “It often matches the clothing distribution.
“In addition, there is a genetic relationship to melanoma. Only about 1 percent of infants are born with a mole.
” For those children who have many nevi, we encourage parents to check their child’s moles monthly to detect changes.”
If you notice a new “birth mark” on your child, keep visual track of it. “Normal looking new moles are not suspicious,” says Dr. Fox. About one-third of melanomas arise in a pre-existing nevus.
“By the time most people reach adulthood, they have between 10 and 40 moles,” says Dr. Fox.
A lot of sun is another risk factor for melanoma, and maybe as a parent you’re not overly concerned about your child developing melanoma since this is extremely rare in kids.
However, older age is a risk factor for melanoma, and childhood sun exposure can lay the groundwork for melanoma risk decades later!
In other words, parents should see the big picture: Their child’s risk of melanoma when their “kid” is 40 years old!
If you’re inspecting your child’s back moles (or elsewhere) for the first time and notice that some look funny, this doesn’t mean melanoma.
Get familiar with the nevi so that you can detect a changing or evolving nevus.
Follow your gut feeling and make an appointment with a dermatologist if your child has a suspicious looking skin lesion.
Concerning signs include irregular shape, jagged edges, red portions within the nevus or varying colors, larger than a pencil eraser, and of course . . . changing.
How often should I check the moles on my child’s back?
Every month, and inspect any area exposed to sun including the scalp and behind ears.
Draw a mole map and take photos and compare every month.
If this is overwhelming, pursue serial digital dermoscopy, which is ideal for kids and adults who have many moles on their back.

In 1987 Dr. Fox founded the AAD Melanoma and Skin Cancer Prevention Program in Queens, NY. He has been chief of dermatology of several major teaching hospitals including Mt. Sinai Hospital of Queens.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Albina Glisic

Are Most Funny Looking Moles Normal & Benign?

A dermatologist speaks about strange or weird looking moles.
Have you discovered a funny looking mole on your body and wonder if it’s melanoma?
The aggravating thing about finding a strange looking spot is when you’ve never done a skin exam for cancer before, and thus, you have no idea if the “birth mark” has always looked funny.
So now, you study the strange mole every day, wondering if it’s in the process of changing.
“Generally speaking, when moles have the following qualities, it can raise a concern for melanoma,” says Andrea Cambio, MD, board certified dermatologic surgeon, and medical director of Cambio Dermatology in Florida.
Asymmetry. One half of the lesion does not match the other in terms of color, size or shape.
Border irregularity. The border is jagged, scalloped, notched or not smooth, or “bleeds” into the surrounding skin.

Dysplastic mole. Cancer.gov
Color variation. It has different shades of blue, black, brown or red.
Diameter. Greater than that of a pencil eraser (6 mm).
Evolving. It is changing; it may be crusting, bleeding, itching, elevating, changing colors or getting darker (or lighter).
What if you’re viewing a funny looking mole for the first time? Has it always been that way? What did it look like a year ago? Was it even there a year ago?
What should you do?
Live in fear for the next few months as you keep an eye on the strange looking mole, wondering if it’s in the process of evolving?
Dr. Cambio explains, “Any mole can have one or more of these qualities and still be benign. A board-certified dermatologist is skilled at evaluating moles.”
If the spot appears suspicious to the physician, “it may need to be removed and sent for biopsy to differentiate a benign mole from a pre-cancerous or cancerous one.”
For peace of mind, it’s perfectly okay to request that the spot be biopsied. This can be a partial biopsy or removal of the entire lesion.
Don’t worry about scarring; it’s negligible and may be less noticeable than the pigmented growth that was removed.
A dermatologist may feel very certain that a strange mole is benign, but remember, absolute proof of this can only come from a biopsy.
Dr. Cambio adds, “The more atypical (dysplastic) moles an individual has, the more likely they are to develop a melanoma in their lifetime.”
These are funny or “ugly” moles that typically appear on a person’s back.

Dr. Cambio has extensive training and experience in all aspects of adult and pediatric dermatology, laser, skin cancer, dermatologic surgery and cosmetic dermatology.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Mikel Ugarte Gil

Trouble Breathing After Coronary Bypass Causes & Solutions

Trouble breathing or shortness of breath after coronary bypass surgery?
There are actually several causes for breathing difficulties following coronary bypass surgery (aka CABG).
“Shortness of breath is very common after coronary artery bypass grafting,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Primary causes include atelectasis (collapse of small air sacks in the lungs), and fluid within or around the lung.”
My mother, following her quintuple bypass surgery, had this exact problem.
The term “pulmonary effusion” came up when she was examined, and the fluid and partial collapse was detected with imaging tests.
She had bouts of “labored breathing” or “difficulty breathing,” that in part, could be explained by the atelectasis and effusion.
Dr. Fiocco continues, “Every patient has these issues after surgery to some degree. Atelectasis occurs due to poor inspiratory effort due to the pain of the incision.
“This improves with walking, deep breathing exercises and coughing.”
My mother was instructed to use a little gadget called an incentive spirometer.

BruceBlaus/CC
It’s not only given to coronary bypass patients, but anybody who needs bed rest following any kind of surgery … to encourage lung expansion, which will help prevent breathing difficulties and pneumonia.
The patient places the mouth on the spirometer’s mouthpiece and slowly inhales, while watching the device record a numerical value of how much air is being inhaled.
Coughing gets the lungs working; very important for coronary bypass patients to help with their breathing and prevent any problems.
A respiratory therapist will also visit the CABG patient, but despite these measures, the coronary bypass patient may still (and commonly) experience some trouble with breathing.
So what can be done, then, about the fluid buildup in the lungs after coronary bypass surgery?
Dr. Fiocco explains, “Fluid is removed with diuretics (fluid pill). They increase your urine output and draws fluid off the lungs.”
But what if the patient, following coronary bypass surgery, has renal failure?
My mother had “mild” renal failure, and hence, there was a period where she could not receive diuretics, because their effect (promoting urinary output) would stress the kidneys!
Solution? She was on fluid restriction until her creatinine level (measure of kidney function) was acceptable.
Over time the fluid buildup in her lungs disappeared, and her lungs eventually appeared normal on imaging.
A coronary bypass patient, however, can end up with so much fluid that it really makes breathing difficult, and frequently.
Dr. Fiocco says, “Occasionally, so much fluid accumulates around the lung that it must be drained with a catheter.”
My mother’s surgeon actually mentioned this as a plan if a follow-up CAT scan were to show that the fluid was still present.
“Rarely, fluid collections around the heart can cause shortness of breath requiring drainage,” adds Dr. Fiocco.
“Even more rare is a pulmonary embolus, or blood clot to the lung which is treated with blood thinners.”
Finally, a possible cause of trouble breathing after coronary bypass surgery, especially when the previous mentioned issues have been ruled out, is plain anxiety.
My mother’s cardiologist reported to me that there were a few instances in which she complained of labored breathing, and visibly had trouble with normal breathing,
But once the doctor had her engaged in conversation unrelated to her CABG, her breathing appeared perfectly normal. He told me this was anxiety related.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Diarrhea, Changes in Poop Appearance from Microscopic Colitis

“Change in bowel habits” is commonly listed as a symptom of colon cancer, but this doesn’t mean that microscopic colitis can’t also cause a change in poop habits and appearance.
Your stools and bowel habits can indeed change from microscopic colitis.
So if you’ve been noticing a change in bowel habits lately, sudden diarrhea or a change in the so-called stool caliber — don’t automatically fear this might be colon cancer.
It may very well be microscopic colitis.
“Typically patients experience watery, chronic diarrhea that can last for months or years.” Alan Gingold, DO, a board certified gastroenterologist with Central Jersey Ambulatory Surgical Center.
“It does tend to be intermittent, and the diarrhea can come and go.
“Why patients get diarrhea in this condition is not fully known, but likely the chronic lymphocytes or collagen deposition causes inflammation and scarring, which prevents adequate absorption of water from the colon — leading to diarrhea.”
I developed symptoms of microscopic colitis some years ago.
It first began with sudden-onset diarrhea. I didn’t think anything of it and didn’t even really look at it, because this began happening in the days leading up to my period, and I’ve had premenstrual diarrhea in the past.
However, I noticed that every time I had a bowel movement, it was in the form of diarrhea, and several times a day.
After my period started, I knew something else was going on, and being the health-conscious person I am, I became alarmed.
The diarrhea was liquidy and presented with a light brown color, sometimes with a greenish tinge.
Normally, my diarrhea is a milk chocolate color and colors the toilet water brown; it’s messy.
But this particular diarrhea was swift and “clean,” creating a pile of very loose, scruffy, flaky stools at the bottom of the bowl, sometimes a few pieces floating in the toilet water.
This diarrhea did not look like diarrhea I’ve had in the past.
It would be another 24 days before I was diagnosed with microscopic colitis. In the meantime, the diarrhea seemed to mostly be a reaction to eating.
Soon after eating, I’d feel a churning in my gut: the formation of yet more diarrhea.

Shutterstock/George Rudy
At one point, within 20 minutes after eating a generous amount of brownie and milk, I let loose a lot of diarrhea, and it seemed as though the entire snack went right out the other end.
The diarrhea always contained particles of undigested food.
Spinach (a lot, actually); grapes; sunflower seeds; and different-colored particles such as bits of broccoli and tomatoes.
The diarrhea was more prevalent on days that I consumed a lot of juice and fruit.
I backed off on these, but the diarrhea persisted, though not as much.
Taking an anti-diarrheal drug resulted in two days of nothing, and then I had formed stools, but they looked funny: light brown, scruffy and containing undigested food.
After this bowel movement, the diarrhea returned, and I’d also have very loose stools. The color was always light brown/tan.
Most of the stool pieces sunk in the toilet water, but sometimes there were floating pieces.
At one point a whole mess came out and every chunk stayed on top of the toilet water.
The diarrhea pieces ranged from liquidy to small pieces to bigger chunks, that — when I poked with a Q-tip swab, dispersed rather than maintained their form.
After cutting out fruit, juice and vegetables entirely, I began having loose stools.
But they continued to contain a lot of undigested food: rice, lentils and bits of tomato.
The stools were formed enough to maintain their form when I lifted them out of the water with a plastic spoon.
But they looked very different: light brown, sometimes with a greenish tinge and sometimes with an orange tinge.
The layered stools were greasy looking and appeared to be composed of several different substances, rather than all one uniform substance.
They ranged from normal size to small pieces, and the normal sized stools were pointy on both ends.
Early on in the microscopic colitis, I’d feel the stools or diarrhea forming in my gut throughout the night, and there were times it felt I had to go right then and there, but I stayed in bed.
Soon after getting up for the day, I’d have to relieve myself. But as days went on, it would be around noon before I had a movement.
The movements dropped to 1-2 stool releases per day, still odd looking. With more time, there appeared to be less undigested food in the stools.
Over the next several weeks the situation spontaneously resolved.
Microscopic colitis can only be diagnosed with a colonoscopy.
The doctor must collect tissue from inside the large colon for analysis — and the colonoscopy allows them to do this.
Microscopic colitis in my case resulted in a change in bowel habits, mild abdominal cramping and thirst in the middle of the night.
Patients may also feel bloating, nausea, have weight loss and transient joint aches.
If you suspect microscopic colitis, then remember that only a colonoscopy can detect this.
 Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, katemangostar

When Stool Color Can Mean Cancer

Ever had yellow, chalky, green or black stools?
What about reddish stools? Do you ever even look at your BMs? Certain colors of BMs or stools can be a warning sign of cancer.
“Brown, gray, tan or yellow are all caused by your environment – food you eat, beverages you consume and even the level of stress you are experiencing at that time in your life,” says Sander R. Binderow, MD, FACS, FASCRS, with Atlanta Colon & Rectal Surgery.
You should examine what’s in the toilet! It’s unsightly, but you need to know what your bowel movements normally look like in shape as well as color, since certain stool colors are associated with colon cancer.
The color of poop can indicate what’s going on in your body. Poop can come in a variety of colors.
Any Shade of Brown Stools

This is normal.
Green Poop

Normal. Don’t panic. It’s not cancer. Bowel movements actually start out as green.
There are two chief causes of green poop: green foods, and quick transit time of the stools through the large intestine.
Leafy green vegetables, cucumbers, green food coloring and iron supplements can turn poop green.

Freepik.com, 8photo
Quick transit time doesn’t give bile enough time to break down completely, thus retaining stools’ original green color.
Yellow Poop
It’s not cancer. It’s fat in your bowel movement. Fatty stools also float.
Light Colored or White Stools
This indicates lack of bile in the bowel movements, possibly caused by a bile duct obstruction. Drugs for diarrhea can also cause a light color. But see a doctor, because a bile duct can be blocked by liver cancer.
Black or Tarry Stools
SEE DOCTOR. This can have serious as well as harmless causes.

Black or tarry stools
“If blood enters the gastrointestinal tract higher up in the stomach, small intestine or even higher up in the colon, the blood itself is digested before it exits the anus, and digested blood turns this tar or black color,” says Dr. Binderow.
“Black indicates blood being absorbed higher up in the gastrointestinal tract.” Black bowel movements can mean a bleeding ulcer, gastritis or esophageal tear from vomiting.
On the other hand, iron supplements can blacken bowel movements. So can anti-diarrheal drugs, black licorice and blueberries.
Red or Maroon Stools

SEE DOCTOR. This could mean several life-threatening medical conditions including colon cancer.
“Maroon is lower in the intestine, and red is even lower, but all need to be checked by a doctor,” says Dr. Binderow.
“There should be no blood in your stool. It could be hemorrhoids, but it could be more serious, so this should always be addressed with your doctor.”
Red in poop can also point to anal fissures, bleeding of the diverticuli, inflammatory bowel disease, and of course, colon cancer.
- If you see blood in your bowel movements, see a doctor promptly.
- Bleeding means something is WRONG.
However…your bowel movements may appear “red” and not have any blood in them.
Bright reddish stools can result from eating foods with red dyes like beverages, gelatin and popsicles.
Bright red poop can also be caused by red licorice, tomato juice, tomato soup and BEETS !

Shutterstock/Lepas
You wouldn’t think beets, with their dark purple color, could cause bright red stools. But extracted beet juice is one of the brightest reds you’ll ever see.
Beets give BMs more of a crimson “ribbon” around them that intertwines with them, versus literally changing their color.
“Clay” Color
“If the clay is a red clay, this again could be caused by blood in the stool,” says Dr. Binderow.

Clay grey stools
Liver and pancreatic cancer, not just colon, can alter the color of stools, making them a “clay grey.” See a doctor rather than wondering about it!
By being visually acquainted with your BMs, you can learn to distinguish between food-color-induced redness, and blood-induced redness.
Dr. Binderow explains, “Screening with your doctor could be through colonoscopy.
“However, if you are averse to getting a colonoscopy, there is a new noninvasive stool DNA screening test that can be done in one’s home and is available by prescription.”

Cologuard
Cologuard is a non-invasive screening test for colon cancer that uses the latest advances in stool DNA technology.
And that is the detection of altered (mutated) DNA from abnormal cells in a stool sample which could be associated with cancer or precancer.
 Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
,
Top image: Shutterstock/docstockmedia
Source: mayoclinic.com/health/stool-color/AN00772

Malabsorption Syndrome: Cancer, Other Causes, Symptoms Q & A

Are malabsorption syndrome and cancer necessarily in the same sentence?
- Do you fear you’re suffering from a malabsorption malady?
- Is there a way you can tell at home if you have this gastrointestinal ailment?
If you’ve been having these symptoms, you might think it’s malabsorption syndrome; you may then think, “Thank goodness it’s not cancer.”
However, what might be the cause of the syndrome in the first place?
Cancer is a possible cause, but not a likely cause.
There are numerous causes for malabsorption syndrome other than cancer.
These include bacterial overgrowth in the small intestine; chronic pancreatitis; celiac disease; surgical procedures; parasitic infections; and viral/bacterial infections.
Is a hallmark sign of this ailment oil droplets in the toilet water?
“Oil slicks and droplets are characteristic of patients with very significant and gross fat malabsorption,” says Ned Snyder, MD, Chief of Gastroenterology, Kelsey-Seybold Clinic, Houston, Texas.

“In some types of malabsorption, the primary substance that is not absorbed may not always be fat.”
“For instance, if one has disease of the terminal ileum or a previous surgical resection of this area, then B12 and bile salts will be malabsorbed, and the stool can be normal or liquid after meals, and the patient will be anemic.
“In celiac disease, the fat malabsorption may be modest and the primary presenting problems could be anemia from iron malabsorption or bad bones because of poor absorption of calcium and vitamin D.”
Do stools here have a typical, characteristic appearance?
“It really depends again upon what is malabsorbed,” says Dr. Snyder.
“There are many manifestations of malabsorption, and only a minority of cases have the classic features (stools that are greasy, oily, bulky, foul-smelling).

“In classic fat malabsorption in chronic pancreatitis (or pancreatic cancer), the stools will be light colored, voluminous, float, and be oily.”
“However, all stools that float do not represent malabsorption.
“Also, one can have mild fat malabsorption, and have normal stools.
“If the malabsorption is for carbohydrates or bile salts, the stools can be watery. Protein malabsorption is primarily manifested by muscle wasting, weakness, etc.”
Just how much undigested food will a person typically see in their stools with this condition?
“Undigested food is primarily seen in only the most gross cases of fat malabsorption,” says Dr. Snyder.
Are stools with this condition always loose and diarrhea-like, or can stools be solidly formed?
“If the malabsorption is selective for B12 or iron, the stool can be normal,” says Dr. Snyder.
“However, when fat or bile salts are malabsorbed, the stools will be loose.”
What percentage, if known, of malabsorption syndrome is the result of cancer?
Dr. Snyder explains, “Cancer is a rare cause, except in the elderly when cancer of the pancreas is the etiology of a small percentage of cases.”
(The pancreas is the organ most commonly associated with malabsorption.)
How uncommon is pancreatic cancer in people under 50?
“I can’t provide an exact figure, but pancreatic cancer is highly unusual under the age of 50.
“I suspect approximately 5-8 percent of patients are 50 years of age or younger.
“The mean age is 72, and the incidence of the disease begins to go up sharply in a linear fashion after age 50.”
What is the most common cause of the syndrome in young adults? In middle aged people?
In children? Dr. Snyder says, “Young adults: celiac disease; middle age: celiac disease and chronic pancreatitis; children: cystic fibrosis and celiac disease.”
Celiac disease: The body thinks gluten is an invader and thus mounts an immune response, which over time damages the intestinal lining.
Do the stools float all the time, or can they sometimes sink, with this condition?
“They can sink.” If a person suspects they have this, what should they tell their doctor? “Give a good history including a description of the diarrhea and weight loss, if any,” says Dr. Snyder.
“Gastroenterologists often go straight to colonoscopy with a history of diarrhea.
“Colon diseases can cause diarrhea but not malabsorption, so a colonoscopy will not turn out to be helpful sometimes.
“Patients should ask for evaluations of their small bowel and pancreas.”
What conditions can mimic this ailment?
Dr. Snyder explains, “Common diseases that can present like malabsorption but not usually associated with it include microscopic colitis, Crohn’s disease, ulcerative colitis, infection with giardia, and irritable bowel syndrome.
“Lactose intolerance is common and sort of a malabsorption problem due to a deficiency of the enzyme lactase and should be mentioned as well.”
 Dr. Snyder is a member of the American Gastroenterological Association and the American Society for Gastrointestinal Endoscopy.
Dr. Snyder is a member of the American Gastroenterological Association and the American Society for Gastrointestinal Endoscopy.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Robert Kneschke

Acid Reflux Symptoms Compared to Sinusitis

You think you have acid reflux but you may have sinusitis; or, you’re convinced you have sinusitis but it just might be GERD!
The symptoms of GERD or acid reflux and sinusitis, do indeed overlap, and one condition is often mistaken for the other by sufferers as well as physicians.
“GERD is technically the wrong term; it actually is laryngopharyngeal reflux (LPR),” says Jamie A. Koufman, MD, Director of the Voice Institute of New York and a leading authority on reflux disease.
“GERD refers to reflux into the esophagus, but not all forms of acid reflux disease.
“When the air passages are involved, medical specialists usually call it LPR, also often called silent reflux.”
So if you want to know how to tell GERD symptoms from sinusitis, the better question is:
How do laryngopharyngeal reflux symptoms compare to those of sinusitis?
Dr. Koufman explains, “Reflux can cause post-nasal drip and too much throat mucus, as can sinusitis; but more importantly, reflux can actually be the cause of sinusitis.
“LPR is called ‘silent reflux’ because the reflux can occur during the night; and when this occurs, the stomach contents (enzymes and acid) actually make it all the way up into the back of the nose, where they can cause problems with the sinuses.”

Shutterstock/Elen Bushe
Can a person have LPR and sinusitis, but with both conditions independent of each other, rather than one causing the other?
Dr. Koufman explains, “A person can have both conditions.
“However, reflux is more likely to cause sinus disease than sinus disease to cause reflux.
“As doctors become more aware that reflux can cause disease anywhere in the airway, including the sinuses, more people will receive treatment, which can prevent sinusitis.
“In other words, many reflux patients on long-tern anti-reflux treatment report that their sinus troubles vanish, too.”
How often is GERD misdiagnosed as sinusitis?
“LPR/GERD is often misdiagnosed as sinusitis, simply because of the post-nasal drip,” says Dr. Koufman.
“Too much throat mucus is one of the most common symptoms of LPR.”
What is the function of mucus? It creates a protective barrier for the nasal membranes, as well as the membranes that line the throat.
“When irritation is present from reflux, generally more mucus is produced, almost as if the body was trying to better protect itself,” says Dr. Koufman.
About half of Dr. Koufman’s patients, who have been diagnosed with sinus disease by other doctors, don’t have sinusitis.
She adds, “Unfortunately, sometimes I see such patients after they’ve had unsuccessful and ineffective sinus surgery.”
Why is GERD so often misdiagnosed as sinusitis?
“Reflux is misdiagnosed as sinusitis, even when special X-rays are obtained,” says Dr. Koufman.
“Thick lining inside the sinuses is actually not ‘sinusitis,’ but can be associated with reflux or even allergies.
“True sinusitis will show complete opacification of the sinus or even an air-fluid level.” Opacification means non-transparency.
The truth is, continues Dr. Koufman, that “many physicians assume that nasal/sinus symptoms are due to sinusitis simply because they are still unaware of silent reflux.
“After all, if a person doesn’t have heartburn or indigestion, it’s easy (easier) to overlook the diagnosis of LPR.”
So how is a diagnosis of LPR made?
One must make an appointment with an ENT (ear, nose and throat) doctor for a complete throat and nose exam.
Dr. Koufman adds that there is now a special test called pharyngeal pH-monitoring that detects acid in the upper area of the throat.
If you have symptoms that seem to be GERD or sinusitis, don’t try to self-diagnose; make an appointment with an ENT physician.
 Dr. Koufman has lectured nationally and internationally and is one of the world’s leading authorities on reflux. For 25+ years her pioneering research has focused upon acid reflux as it affects the voice and airway.
Dr. Koufman has lectured nationally and internationally and is one of the world’s leading authorities on reflux. For 25+ years her pioneering research has focused upon acid reflux as it affects the voice and airway.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/9nong
Source: refluxcookbook.com/authors

IBS (Irritable Bowel Syndrome) Stools vs. Malabsorption BM’s

Malabsorption that results in odd-looking stools can have a variety of causes, and IBS (irritable bowel syndrome) can also cause stools to appear less-than-normal.
You may be wondering if there was a way to distinguish between IBS and malabsorption stools.
“I do not think there is any good way to tell apart the stools of someone who just has IBS from other malabsorption conditions like celiac disease, cystic fibrosis, or even inflammatory bowel disease,” explains Pejman Katiraei, DO, FAAP, an integrative physician whose many areas of specialty include adult and pediatric IBS.
Cystic fibrosis is an inherited genetic disorder that primarily affects the lungs.
Other causes of malabsorption include lactose intolerance, soy milk intolerance, bacterial overgrowth, microscopic colitis, Crohn’s disease, surgical procedures, infections, medications and pancreatic cancer.
If you’re experiencing malabsorption, chances are that your stools will be extremely foul-smelling.
However, very foul-smelling stools don’t mean you have malabsorption, and the absence of a foul odor doesn’t automatically rule out malabsorption, either.
Dr. Katiraei continues, “Any of these conditions can show up in all kinds of different ways. As such, in my opinion it is never a good idea to make a diagnosis based on how stools look.
“You have to look at the whole picture (Is the person having fevers? Are they losing weight?).”
Malabsorption often causes weight loss and other symptoms such as cramping, bloating, gas and muscle-wasting.
However, the absence of these other symptoms does not rule out malabsorption.
Dr. Katiraei continues, “Once this information is combined with lab testing and even an endoscopy by a gastroenterologist, then you can safely say that it is IBS or not.
“In my opinion, it is dangerous for any person to make a guess as to what condition they have based on the appearance of their stool.”
What you can do, however, is get familiar with the caliber of your stools.
Most people will not look at, much less closely examine, their stools, as they think this is “gross.”
Rest assured, you can actually get used to viewing what plops into the toilet bowl water.
I certainly did after I developed microscopic colitis.
My stools took on all sorts of funny shapes and textures, including bulky, oily looking, foul smelling, with lots of undigested food intertwined in them.
Sometimes my poops floated, and they had lost their normal milk-chocolate color and were a spectrum of tans, often with a greenish tinge.
Sometimes they’d promptly disperse in the water if I poked them with a cotton swab, and they were never fully formed, meaning, they were what I called semi-diarrhea.
Nevertheless, it turned out that I did not have malabsorption, in that the gastroenterologist who performed my colonoscopy looked at the stool samples in a jar that I brought into the exam room, and he said I did not have malabsorption.
He drew that conclusion by looking at my BMs, but there are fecal-sample lab tests that can determine if you have malabsorption.
If you’re familiar with what your stools should look like when everything is in balance within your body, then you will definitely know when something doesn’t look right.
If you have IBS, get to know how IBS affects the appearance of your stools.
You can’t diagnose by looking inside the toilet bowl, but what you see inside the toilet bowl is enough information to determine whether or not to see a gastroenterologist.

Dr. Katiraei created Wholistic Kids and Families for people interested in learning how to raise a healthy child (and future adult) in a world that’s becoming increasingly polluted with toxins (chemical and emotional).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Sofi photo
Sources: Merckmanuals.com; .nlm.nih.gov/medlineplus/ency/article/000299.htm

Does IBS Usually Cause Thin Narrow Poops?

Do narrow stools have you fearful of colon cancer, even though you’ve been diagnosed with irritable bowel syndrome (IBS)?
If narrow or thin stools are common with IBS, then this may certainly provide more peace of mind in the person already diagnosed with this aggravating condition.
“Narrow stools can be common with IBS, and they may be very difficult to differentiate from colon cancer,” says Pejman Katiraei, DO, FAAP, an integrative physician whose many areas of specialty include adult and pediatric IBS.
“Depending on what is happening to a person’s gastrointestinal tract, a person suffering from IBS can have everything from severe constipation to watery diarrhea.
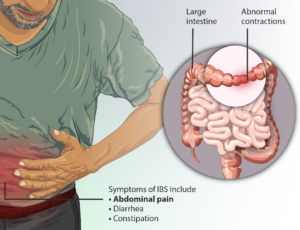
Irritable Bowel Syndrome. Source: myupchar.comen
“As such, there is no specific type of stool that would allow a person to know they have IBS over deadly conditions like the early stages of inflammatory bowel disease or even colon cancer.”
If you’ve already been diagnosed with irritable bowel syndrome (and the diagnosis should have been made after an entire battery of tests ruled out other possible causes of your GI distress such as colon cancer), then you can conclude that the presence of narrow or skinny stools is most likely a part of having irritable bowel syndrome.
However, Dr. Katiraei adds, “I would strongly encourage people suffering from gastrointestinal problems to be evaluated by a medical professional.
“Simple blood and stool testing can give important information that can be life-saving.”
So assuming, then, you’ve already been cleared of colon cancer, and have been diagnosed with irritable bowel syndrome, there is one critical element you must never forget:
Just because you’ve been diagnosed with irritable bowel syndrome, doesn’t mean that you’ll never get colon cancer!
A person with irritable bowel syndrome can still develop colon cancer, so get to know your IBS presentations very carefully and meticulously.
After all, the symptoms of irritable bowel syndrome and colon cancer strongly overlap and are virtually identical.
Have your apparent IBS symptoms changed lately?
Have you always had narrow stools, or are narrow stools only a recent occurrence after having irritable bowel syndrome for years?
Is there suddenly blood in your stools?
Have you had IBS for years, and are now suddenly losing weight for no reason?
Unexplained weight loss can also mean diabetes or overactive thyroid; get a thorough medical exam.
Do you have any other new symptoms that don’t seem to fit the bill for irritable bowel syndrome?
If you’re in doubt, then get another evaluation by your doctor.
Don’t assume you can’t have colon cancer because you have IBS.
Irritable bowel syndrome cannot morph into colon cancer, but a benign and malignant disease of the GI tract can exist simultaneously in the same person.
Dr. Katiraei created Wholistic Kids and Families for people interested in learning how to raise a healthy child (and future adult) in a world that’s becoming increasingly polluted with toxins (chemical and emotional).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}