

Stools & Poops: Shape, Color, Texture Can Reveal Disease

Stools – no, I don’t mean the high circular chairs in bars – but poops. How well do you know your poops?
If you’re reading this, chances are pretty good that you’ve examined your poops more than once.
Take it from me: Once you examine your stools, it won’t gross you out; it will become very tolerable.
Doctors realize that stools can be very telling of a person’s health, and strong indicators of all sorts of disease, including cancer.
Poops come in so many kinds of shapes, textures and colors.
They can be oily or greasy, hard, come out like pebbles or long ribbons, be soft, full of undigested food, laced with blood, very foul smelling, be floaters or sinkers…
Here are several BM articles featuring a gastroenterologist’s expert answers.
Causes of narrow stools other than colon cancer
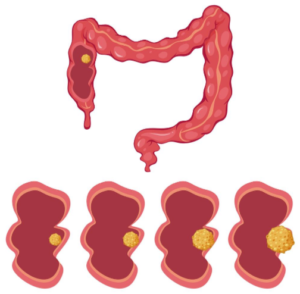
Source: Vecteezy.com
Is there a way to tell the difference between stools from irritable bowel syndrome and colon cancer?

When stool color might mean cancer

Are stools that are thin and long common with IBS?

 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Mouth Symptoms and What They Mean

Mouth symptoms can have tons of causes, and yes, some include cancer.
The mouth can experience a wide range of issues, some benign and others potentially life-threatening.
While many people worry about oral cancer, particularly linked to smoking and heavy drinking, it’s important to recognize that other conditions, like melanoma, can also affect the mouth.
Oral melanoma is extremely rare but shows that this often-deadly form of skin cancer can arise even in the darkets of places.
Melanoma in the mouth can present as unusual spots or lesions, often going unnoticed until they cause significant symptoms.
Dry Mouth

Shutterstock/Tyler Olson
Excessive mouth dryness, not linked to hydration levels, can be uncomfortable and misleading.
Even if someone feels the urge to drink water, they might not be genuinely thirsty, but rather, experiencing a sensation akin to having cotton wads between their teeth and inner cheeks.
This feeling can stem from various causes, including the side effects of certain medications, which can reduce saliva production and lead to a dry, cotton-like sensation.
Another possible cause is a yeast infection in the mouth, which can contribute to dryness and discomfort.
Addressing the underlying cause, whether by adjusting medication or treating an infection, is essential for relief.
If your dry mouth has come on suddenly, here’s information on that: sudden-onset dry mouth.
Metal Taste

Having a persistent taste of coins or nuts and bolts in one’s mouth is a lot more intolerable than the cottony dry feel.
A persistent taste of coins or nuts and bolts can be quite unbearable.
This awful metal taste can significantly impact quality of life, making eating and drinking less enjoyable.
A number of conditions can cause a metal taste in one’s mouth.
Salty Taste

When you eat salty foods, you should not continue to have a salty sensation on your tongue once the food is long-gone eaten.
Whether it’s pretzels, crackers, fries or vegetables that were heavily salted, there should not be a lingering salty taste on your tongue.
But if you’ve been experiencing this, there are causes and solutions.
Coughing

Shutterstock/Aaron Amat
You have no cold, no nasal drip, no flu, so why do you keep coughing — like every few minutes?
Well, ask yourself if you’ve been subjected to much more anxiety than usual. Why stress can cause constant coughing.
Unexplained symptoms involving the mouth or throat should never be dismissed.
These symptoms can indicate underlying health issues that require prompt attention.
Many people are reluctant to see their doctor about a “bad taste” in the mouth or a cotton-like sensation.
But if it’s enough to make you wonder; if it’s enough to distract you or impair the quality of your recreational time — then it’s certainly important enough to bring to your physician’s attention.
Depending on the underlying cause, the treatment could be fairly simple with quick results.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Having Menstrual Problems? What Should You Do?

Sometimes, menstrual problems make women wish they were born a man. Can a baby ever really be worth all this trouble?
Well of course, for those whose maternal instincts are driving at them.
But it’s an undisputed fact: Periods Are a Pain!
Some women are literally disabled for two or three days, curled up in bed with a hot water bottle, dreading every time they must exit their bed and use the toilet.
Menstrual cramps can be so agonizing that a woman will forego eating and drinking water, no matter how hungry or thirsty, just to maintain her tight ball of a position with the heating pad.
Oh, of course, she’ll definitely get up to upchuck, but then promptly get back into her defensive position.
When period pain hits like this, you have no choice but to ride it out and let it run its course.
- Missed Periods and Mental Stress: The Connection
- Why is there blood in your cervical mucous after menstruation ends?
- Why You Have Menstrual Cramps Mid-Cycle
One of the problems that many women experience with their monthly cycle is the persistence of abdominal cramping after the end of their period.
A normal cycle does not cause its associated cramps to continue when the bleeding stops.
It could be a coincidence that the aching continues, being caused by something unrelated to the monthly cycle.
Another common issue is prolonged bleeding during menstration.
It may seem like your period is extra long, but what might be going on is another, unrelated cause of the prolonged vaginal bleeding.
If the bleeding (not residual spotting of old blood, but actual bright red bleeding) goes beyond seven days, you need to find out why this is happening.
Though this is not normal, this doesn’t mean the cause is a serious medical problem, either.
But a check by your doctor will determine what’s behind this sign so that the cause can be treated promptly.
Many women wonder about a somewhat reverse situation: spotting a week before their period starts.
Ideally, you’ll want to see a gynecologist who has a special focus on menstruation for any of your concerns and especially worries or new symptoms.
A gynecologist specializing in menstruation typically has deeper expertise in diagnosing and treating menstrual disorders, such as irregular cycles, heavy bleeding, painful periods (dysmenorrhea) or conditions like polycystic ovary syndrome (PCOS) or endometriosis.
These specialists are more likely to stay up-to-date with the latest treatments and research specific to menstrual health.
In contrast, a general gynecologist provides broader care for a range of reproductive health issues, such as routine Pap smears, contraception and pregnancy-related care, but may not have the same level of expertise or experience in managing complex menstrual issues.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Fluttering and Thumping Heartbeat Scaring You?
What can be scarier than a heart that suddenly flutters or feels like its rapidly quivering?
This makes you feel like a heart attack is seconds away.
Not too many things are more frightening than a suddenly fluttering heartbeat.
Some people get so fixated on their heartbeat that they take frequent pulse checks throughout the day, documenting their resting heart rate, and trying to detect abnormal beats or rhythms.
This kind of obsession can cause continuous anxiety and sap joy from living.
However, the more you know about heartbeats, the more control you’ll feel; knowledge is power!
Here is a sampling of some of my heartbeat articles:
- When to worry about a fluttering heartbeat
- What causes a thumping heartbeat and how to solve this problem
- Do you get heart palpitations while strength training?
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
When a Headache Means Serious Trouble vs. Benign
Pain in the head or a sudden bad headache or even a medium one that won’t go away is one of the most frightening symptoms.
That’s because the head contains the brain!
And anything involving the brain is not to be taken lightly.
But you should also know that not all headaches have their origins in the brain or head.
Some do originate from a so-called pinched nerve in the neck, or muscle tension in the neck area.
But others do mean that a serious problem is going on with the brain.
Headaches: Leading Reason People See Doctors
“Headaches are quite common and usually do not mean anything serious,” says Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths, and Tricks: A PHYSICIAN’S ADVICE.”
“They can be dull and throbbing, sharp and pinpointed, and can last for a few minutes or a few days,” continues Dr. Tavel.
“By far, the most common type headache is brought about by emotional tension, and these are called tension headaches.”
These originate in the neck and shoulder muscles, and sometimes the muscles of the head. The brain is not involved in these types of headaches.
“They can happen to anyone, at any time, any place,” says Dr. Tavel. “There is good news about headaches in general: They are very common and usually have a benign cause.
“A typical headache may last for only a few hours. Or even several minutes.”
Migraines: Trouble Coming, but Still Benign
The pain can be a level 10 on a 1 to 10 scale, but these are benign in that they aren’t life threatening.
“Migraine headaches are less common and usually follow a characteristic pattern,” says Dr. Tavel.
And that pattern often consists of a pulsing or throbbing pain, rather than steady. It’s often on one side of the head as well.
There may be a nauseous feeling with the pain that can lead to upchucking.
The patient may have considerable sensitivity to light and/or sound.
The pain may go on for days and incapacitate the sufferer.
In addition, the sufferer may have an “aura” or warning signal just before the onset of a migraine.
The warning sign may be in the form of a sudden blind spot in one’s vision, flashing lights or one-sided facial tingling.
Dr. Tavel points out that some medications may be helpful, but also that the sufferer should see a doctor about different migraine treatment options.
“The right medicines, combined with self-help remedies and lifestyle changes, may help.”
When Headaches Mean Serious Trouble
“But what if you are experiencing headaches that won’t go away and do not respond to typical treatment?” says Dr. Tavel.
Another consideration is the presence of concurrent symptoms like loss of appetite, slurred speech, being off balance or one-sided weakness.
Concurrent symptoms, depending on their nature, can signal that a headache’s cause is serious.
“A sudden headache of severe pain that occurs after a head trauma may be a symptom of a more serious medical condition,” says Dr. Tavel.
Namely, this would indicate bleeding in the brain: a subdural hematoma or a subarachnoid hemorrhage.
“Any time a head injury results in a headache [even mild], consult a physician as soon as you can.”
Seek Medical Attention ASAP for the Following Signs

Freepik.com
Stiff neck and fever. A harmless tension headache may come with neck discomfort.
These types come on gradually rather than with a bang.
So if the pain level is ultimately a 7, it didn’t start out as a 7.
The tension type typically begins subtlely, sometimes at a 0.5, then progressing to a 1, then 2, and gradually rising in pain level score.
Or, it can start as a 2. And it’s gradual from that point on as it gets worse.
The discomfort can be bad enough to keep a person in bed.
However…“a sudden, severe headache with a very stiff neck and a fever and/or sensitivity to light may mean a serious situation that requires prompt medical attention,” warns Dr. Tavel.
This could mean a migraine but it could also signal a rupturing brain aneurysm.
The hallmark descriptor for a rupturing brain aneurysm is SUDDEN AND SEVERE — like a clap of thunder.
Numbness or weakness. “Either of these symptoms with a headache, especially with another like problems walking, could indicate a serious condition; see a doctor right away,” says Dr. Tavel.
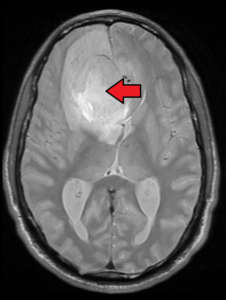
Brain tumor. Credit: James Heilman, MD
These symptoms could be caused by a brain tumor, either malignant or benign. A stroke could also cause these symptoms with head pain.
Other accompanying signs that are suspicious for a serious cause behind a headache are partial loss of or blurred vision, confusion, and very obviously, convulsions, seizures or loss of consciousness.
A headache that’s accompanied by any level of confusion, let alone loss of consciousness or seizures, likely means a serious disease or serious result of an injury.
The three most likely causes would be:
• Brain tumor
• Brain bleed
• Blood clot (ischemic stroke)
There are other origins of headaches not mentioned here, but one last origin deserves some attention: sinus.
The sinus headache can hurt as much as a tearing aneurysm.
Usually an infection is the cause, and compared to a brain tumor or aneurysm, this sounds pretty benign. But an infection needs to be promptly eradicated.
A much more serious sinus-related cause for a headache, however, is a tumor (cancerous or benign) in the nasal or surrounding cavities. These usually cause additional symptoms and are very rare.

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Causes of Diarrhea Include Cancer and Benign Conditions

Diarrhea has so many causes including parasitic worms living inside your intestines.
Ewwww! But that’s highly preferable to cancer, right?
Should you fear cancer every time you have diarrhea?
A Little Bit About Parasites in the Intestines
Intestinal parasites are relatively uncommon in the U.S. compared to developing countries, but millions are still affected.
The CDC reports that infections like pinworm, Giardia and tapeworms occur, with pinworm being the most frequent in kids.
Giardia causes about 1.2 million U.S. cases annually (CDC, 2023).
Adults in the U.S. may be at higher risk for intestinal parasites if they frequently travel internationally, consume undercooked meat or contaminated water, garden without gloves or neglect handwashing.
Close contact with infected kids, poor food hygiene and exposure to untreated recreational water also increase susceptibility to infection.
Causes of Diarrhea After Food Intake
Are you struggling with having to run to the loo with diarrhea after having something to eat? This is called post-prandial diarrhea.
Is diarrhea your only new symptom?
If diarrhea is the only problem you’ve been having — in other words, no stomach pain, no nausea, no fatigue, no unexplained weight loss — you might still be wondering if diarrhea can ever be the only symptom of colon cancer.
Whitney Jones, MD, a gastroenterologist, addresses that topic.
Orange Diarrhea?
The normal color of stools, even very loose ones, is some shade of brown.
It’s normal if they have a greenish appearance. This can reflect recent food intake.
It can also reflect swift transit through the colon. Again, this is normal.
What may be concering, though, is if diarrhea is orange.
Edward Paredez, MD, a gastroenterologist, discusses several serious causes.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Chest Pain, Vomiting, Heart Attack, Anxiety: How Are They Related?
Chest pain with sudden nausea leading to vomiting, along with sudden sweating and/or shortness of breath can mean a heart attack either in progress or soon about to happen.
“The vagus nerve provides connection between the gut, the heart and the brain,” says Sendhil Krishnan, MD, a board-certified adult general cardiologist with advanced subspecialty training in interventional cardiology.
“Over-stimulation of this nerve, such as during a heart attack [or imminent heart attack], can lead to feelings of anxiety with the commonly described ‘sick to my stomach feeling.’ This can also lead to nausea and vomiting.”
My mother was having shortness of breath and had upchucked.
I urged her to go to the ER because I had read somewhere that vomiting for no reason in a person at high risk for heart attack can actually mean a heart attack in progress or about to come.
She was discharged from the ER — after various tests turned out normal — with a diagnosis of acid reflux.
But three days later … she was on the operating table undergoing quintuple bypass surgery and mitral valve replacement.
Heart Attack Suspicion in Elderly People with Chest Pain
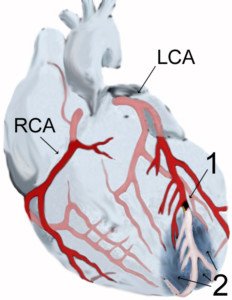
Depiction of heart attack. Credit: J. Heuser
The index for suspicion of a pending heart attack in the typical elderly person with chest pain or sudden shortness of breath at rest should be very high.
To this day I will never know why the emergency room physician leaned much more towards the idea of some kind of digestive issue rather than a heart attack waiting around the corner.
Two days after her ER discharge, my mother then had complained of chest pain.
I took her back to the ER where she was then admitted after a blood test turned up abnormal — but not abnormal enough to diagnose a heart attack.
The next day a catheter angiogram revealed dangerous blockages in five arteries, and she went under the knife several hours later.
Anxiety has been noted as a sign of a looming heart attack, but more striking is that of vomiting.
It was that vomiting — even though it was just a little bit — that really tipped me off that something was wrong with her heart.
“I am also an interventional cardiologist which means I perform catheter-based interventions on patients having acute heart attacks,” says Dr. Krishnan.
“Again, there is involvement of the vagus nerve which can lead to this response of nausea and vomiting which is mediated through a reflex known as the Bezold- Jarisch reflex.”
Why hadn’t this symptom tipped off the emergency room doctor?
I had told him about it. He was more convinced that it was acid reflux!
Screw acid reflux! Ultimately, three physicians all told me that if my mother did not undergo quintuple bypass surgery immediately, she’d likely suffer a massive heart attack within a week.
Trust Your Gut Instinct
“For patients it’s important to note that sudden onset of nausea and vomiting associated with chest pain, sweats, shortness of breath or a sense of impending doom really may be the start of an acute heart attack, and they should seek medical attention immediately,” says Dr. Krishnan.
 Dr. Krishnan is with Pacific Heart & Vascular, where you can view his videos on heart disease and healthy living. He has numerous publications and often speaks at local and regional events.
Dr. Krishnan is with Pacific Heart & Vascular, where you can view his videos on heart disease and healthy living. He has numerous publications and often speaks at local and regional events.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Cancer Symptoms Can Masquerade As Harmless Condition
Cancer is so ruthless that its symptoms can fake a person, even a doctor, into thinking that its symptoms are being caused by a harmless condition–especially when the symptoms come on very small and gradually.
Many symptoms of cancer are also symptoms of many benign conditions.
And many symptoms of a malignancy are also signs of other conditions that are life-threatening.
An example is a hoarse voice. A person’s first thought might be throat (laryngeal) cancer, or that of the lung.
However, a hoarse voice can also be a result of something as harmless as an infection or acid reflux.
It can also mean a thoracic aortic aneurysm, which is life-threatening.
Burping
Excessive burping can be a sign of cancer. Now certainly, few people would ever wonder about this, because burping has always been associated with lacking manners or performing the loudest one at a party.
Burping has also always been tied to eating too much or too quickly, drinking too much carbonated soda or gulping air with each bite or sip of beverage.
But actually, ongoing burping with no explanation (e.g., inhaling a lot of air while gulping soda) is cause for concern — especially if there are other symptoms such as abdominal pain.
IBS vs. Colon Cancer
Unfortunately, the symptoms of these two conditions overlap significantly.
What further aggravates this fact is that there is no clinical test or exam that verified IBS.
IBS is a diagnosis of exclusion. This exclusion includes a colonoscopy.
So in order to get a diagnosis of IBS, you’ll need to undergo numerous tests including a colonoscopy — because the signs of this benign condition and colong cancer are nearly identical.
A Changing Mole
Does a changing mole have you petrified that this could be melanoma?
Actually, melanoma isn’t the only reason that a mole would begin showing changes.
Nevertheless, if you’ve noticed any kind of changes in a mole’s appearance, you should immediately make an appointment with a dermatologist.
With that said, there are several benign circumstances that can “change” a mole.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Lightspring
How Likely Will Esophageal Cancer Come from GERD?
People with chronic GERD may know this can cause Barrett’s esophagus leading to esophageal cancer.
“Risk of GERD developing into esophageal cancer is very low,” says Dr. Maxwell Chait, MD, gastroenterologist at ColumbiaDoctors Medical Group in Westchester County, NY.
Dr. Chait adds, “It depends on the development of Barrett’s esophagus. Ten to 15 percent of people with GERD will develop Barrett’s esophagus in their lifetime.
“The risk of Barrett’s going on to esophageal cancer is less than 1 percent per year: 0.4 to 0.5 percent.”
What is Barrett’s esophagus?
It’s when repeated exposure of lower-esophagus cells to stomach acid results in damage to these cells.
Though the odds of developing esophageal cancer in one who has Barrett’s is very low, as stated by Dr. Chait, the patient still needs regular monitoring to detect any precancerous cells in the esophagus. Treatment at this stage will prevent development of the cancer.
Though many people with Barrett’s do not present with symptoms, here are the key signs: difficulty swallowing food, frequent heartburn, upper abdominal pain, chest pain and dry cough.
As you can see, these symptoms are also key signs of other unrelated ailments.
For example, the symptoms of just chest pain and cough can mean a thoracic aortic aneurysm.
The symptoms of difficulty swallowing food and a cough can result from laryngeal cancer.
The symptom of just difficulty swallowing food can mean many things.
The symptom of only upper abdominal pain can mean pancreatitis.
Chest pain by itself can mean a host of problems including a heart rhythm disorder, heart disease, imminent heart attack, emotional stress and soft tissue strain near the sternum from exercise.
Don’t try to diagnose yourself if you haven’t yet been diagnosed.
See a physician for appropriate tests until the problem is found.
If GERD and Barrett’s esophagus are closely managed, esophageal cancer can likely be prevented.

Dr. Chait’s practice interests include digestive conditions such as colon cancer, gastrointestinal endoscopy and internal medicine. He has authored numerous publications in reputed journals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Kateryna Kon

Calf Pain Only When Walking: Likely Cause

Have you been experiencing mysterious calf pain only when you walk?
Perhaps it’s in one calf, or maybe it’s in both.
Nevertheless, this area never hurts while you are seated or sleeping.
It’s only when you walk that the pain kicks in. What’s puzzling is that you haven’t done anything recently to incur any discomfort such as running extra hard or spending all day climbing hills.
The problem may very well be peripheral vascular disease (PVD).
“Peripheral vascular disease typically causes achy, crampy pain in a certain muscle group supplied by a certain artery,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Dr. Gashti adds that the location is “most commonly calf muscles, after walking a certain distance.”
“The hallmark of pain caused by PVD,” continues Dr. Gashti, “is that it is very reproducible.
“Since the arterial occlusion is a constant, meaning the blockage is there every day, patients complain of experiencing calf pain EVERY TIME they walk from point A to point B.”
Dr. Gashti gives the example of a person who walks every day to a bus stop, and every time feels calf pain.
If the problem has been going on for a while with no let-up, and if the person has risk factors for PVD like smoking, high blood pressure, high cholesterol and diabetes, “then the chances are that they have PVD.”
Persistent pain in the calves should not be ignored. Below is an image of what chronic PVD looks like.

Chronic PVD. James Heilman, MD, CreativeCommons
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}