

Frozen Shoulder Symptoms vs. Arthritis, Plus Treatment

Find out the difference between frozen shoulder and arthritis symptoms, and how to treat frozen shoulder without surgery.
The medical term for frozen shoulder is adhesive capsulitis, and it can be misdiagnosed as arthritis due to the similarity of symptoms.
In frozen shoulder, the tissue around the joint is chronically inflamed; this causes a thickening and tightening in the affected area.
Symptoms of Frozen Shoulder
Significant pain and restrictive movement. These symptoms are also common with other musculoskeletal conditions of the shoulder—such as arthritis.
The right diagnosis may require extensive investigation into one’s medical history.
“Adhesive capsulitis involves idiopathic [unknown cause] inflammation of the shoulder joint capsule, causing pain and decreased shoulder motion,” says Jessalynn Adam, MD, who specializes in primary care sports medicine with OrthoVirginia.
“There are three phases: freezing (the shoulder is painful and stiff), frozen (the shoulder is no longer very painful but motion is significantly restricted), and thawing (shoulder motion gradually returns to normal). This can be quite a prolonged process, up to 26 months.”
Is arthritis sometimes misdiagnosed as frozen shoulder syndrome?
“Perhaps, but age and other health conditions can help to differentiate the two,” says Dr. Adam.
“Frozen shoulder or adhesive capsulitis typically affects middle-aged women between the ages of 40-60.
“It is more common in those with autoimmune conditions such as diabetes, thyroid dysfunction, atherosclerotic/heart disease and Dupuytren’s contracture [a hand condition].”
Painful and Stiff Don’t Always Mean Frozen Shoulder
A report in the 2011 Journal of the American Academy of Orthopaedic Surgeons states that people who have a painful and stiff shoulder are often diagnosed with “frozen shoulder.”
But many things can cause motion loss in a joint.
Details of Frozen Shoulder Symptoms
- Inability to sleep on the affected side due to pain
- Movement so restricted that dressing is difficult, and other things as well like hair care such as shampooing.
- Pain will often decrease once the motion becomes quite restrictive, but pain will bite when the patient makes a sudden movement beyond the confinements of the stiffness.
This is because of microscopic tearing of the scar tissue.
Symptoms of Arthritis
When one tries to move the shoulder, there is often a ratchety or grinding sensation, which is not present with frozen shoulder syndrome.
An X-ray can show arthritis.
Treatment
“Physical therapy focused on capsular stretching, cortisone injected into the shoulder joint to reduce inflammation and pain, rest, time,” says Dr. Adam.
The stretching should be gentle and progressive over a period of weeks, even months sometimes.
“Most cases respond well to these treatments,” says Dr. Adam.
“Refractory cases can be treated with a high volume injection or manipulation of the joint under anesthesia.”
Surgery is a very last resort, but is rarely needed.
 Dr. Adam specializes in the care of athletes and active individuals of all ages, offering prevention, diagnosis and treatment of sports and exercise injuries. Dr. Adam’s care focuses on muscle injuries and biomechanics.
Dr. Adam specializes in the care of athletes and active individuals of all ages, offering prevention, diagnosis and treatment of sports and exercise injuries. Dr. Adam’s care focuses on muscle injuries and biomechanics.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/wavebreakmedia
Source: sciencedaily.com/releases/2011/09/110907132100.htm
Lisinopril Can Cause Blackouts and Here’s Why
Yes it’s true that the blood pressure drug Lisinopril can cause you to pass out.
That’s a tough situation to be in: hearing you have high blood pressure but that the medication for this can cause a blackout.
So imagine being told that you need a drug such as Lisinopril to lower your high blood pressure (or increase the “squeezing” ability of your heart) — but that this drug can also cause you to black out as a side effect.
“Yes, Lisinopril can cause blackouts if the person is very sensitive to the medication, meaning their blood pressure drops significantly in response to the medication, and such a precipitous drop can cause one to suddenly black out,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
It’s also possible that a person can seemingly be compatible with Lisinopril for a very long time — until the state of their body becomes compromised, making them more vulnerable to blacking out or fainting.
An example of that incompatibility would be recent major surgery.
This can make the body more sensitive to Lisinopril, causing a big drop in blood pressure when the patient quickly rises to a standing position — leading to a fainting episode or feeling like the room is “going black.”
How common is fainting from Lisinopril?
“This is not that common with Lisinopril, but can happen especially if the person is dehydrated or not eating or drinking enough, or is already on other BP medications.”
There’s no way to predict ahead of time with certainty whether a given patient will have this particular side effect.
Reducing the Chance of a Blackout
To reduce fainting risk on lisinopril at home, you should stay well-hydrated, first of all. One way to ensure this is to get a very large thermos and fill to the top with water at the start of the day, with the goal of finishing all the water by bedtime — in addition to drinking water with your meals and snacks.
Next, be sure to rise slowly from sitting or lying positions; avoid sudden standing.
Also, limit alcohol (better yet, see if you can quit drinking altogether; it’s not good for the blood vessels), and monitor blood pressure regularly.

Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/forma82

Can Ejection Fraction Be Increased without Drugs?

What can you do to increase ejection fraction if you don’t want to take medications that might cause fainting?
“There are really no other good ways of increasing ejection fraction other than medications,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“Exercise may help to raise ejection fraction, but over the long term is not as proven or effective as ACE inhibitors like Lisinopril or beta blockers such as Carvedilol, which can both cause blackouts.”
If you don’t yet have what would be considered an abnormally low ejection fraction, then what you can do is lead a lifestyle that’s designed to prevent your ejection fraction from getting low enough to necessitate drugs.
Medications do not cure low ejection fraction; there is no cure. Low ejection fraction can lead to congestive heart failure.
Prevention or maximal delaying of this condition comes in the form of avoiding tobacco, engaging in rigorous cardio exercise and strength training, and sticking to an anti-inflammatory diet.

“Aldactone, which is an aldosterone blocking medication, is now also used to help increase ejection fraction after adequate beta blocker and ACE inhibitor doses are already being used,” says Dr. Sayeed.
“It usually does not cause blackouts and may be an option used alone if they cannot tolerate the other two meds.” Aldosterone is a hormone secreted by the adrenal glands.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rocketclips, Inc.

Constant Chest Pain & No Other Symptoms: 8 Causes

A cardiologist explains eight conditions that can cause constant chest pain but no other symptoms.
What can possibly cause constant chest pain and no other symptoms?
The most common cause is angina, says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
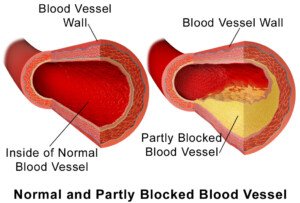
Angina is chest pain as a result of coronary artery disease.
Dr. Sayeed explains, “If the pain is constant, there is likely a severe flow-limiting coronary artery lesion that is causing persistent inadequate blood flow and ischemia [impaired oxygen supply] to a portion of the heart, resulting in constant chest pain which will usually not abate unless medication is administered or percutaneous intervention as in a stent or angioplasty is performed.
“Or if enough time passes, that portion of the heart will either scar over and the pain will go away, or collateral circulation will develop and the pain will be relieved.”
Collateral circulation is when new coronary vessels develop and transport blood.
If you think you have angina, do NOT assume it will eventually scar over or collateral circulation will solve the problem. You may need a stent or even bypass surgery.
Other causes of constant chest pain without other symptoms:
Pericarditis—inflammation of the sac that surrounds the heart.
This “can cause a constant chest pain that is sometimes resolved with high dose NSAIDS or Colchicine, but sometimes is not relieved and can be constant until the inflammation of the pericardium subsides over time,” says Dr. Sayeed.
“Another cause of constant chest pain is musculoskeletal chest pain. This can be due to inflammation or soreness of the chest muscles themselves, similar to what occurs in other muscle groups of the body.

Shutterstock/Zeljko Matic
“Or it can be due to inflammation of the joint between the ribs and breast bone, causing an arthritis type pain of these joints similar to other joints of the body, resulting in constant chest pain that may or may not be relieved by NSAIDS or other pain meds.”
This last condition goes by the name of costochondritis, and it’s hardly unheard of in the bodybuilding world.
“Another cause of chest pain that tends to be more common in women is nerve related and involves the nerve fibers innervating the chest and the heart,” says Dr. Sayeed.
“These can become oversensitive and cause severe chest pain that cannot be explained by most cardiac tests, as these people often have a normal angiogram and stress testing and no muscle or chest wall or rib-breast bone joint tenderness.
“They are often helped by a pain management specialist.”
More Causes Yet
Dr. Sayeed continues, “Other causes of constant chest pain can be hiatal hernia which is when the stomach herniates [enters] into the chest cavity.”
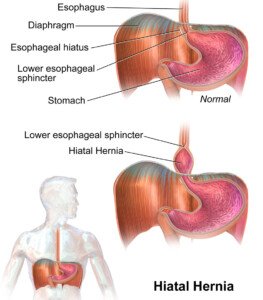
BruceBlaus/CC
The next condition shouldn’t be a surprise, what with all the TV ads about it: gastroesophageal reflux disease (GERD), “due to reflux of gastric acid into the esophagus, causing lower chest pain.”
Next on the list is an esophageal spasm. The esophagus is actually a muscle (though not skeletal muscle).
These spasms tend “to cause very painful constant chest pain.”
Finally, Dr. Sayeed says, “Certain lung conditions causing excessive coughing will also cause constant chest pain.”
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ANN PATCHANAN

Chest Pain Caused By Muscle Spasm from Stress

Yes, stress and anxiety can cause chest muscles to spasm, resulting in scary “chest pain.”
Chest pain has many causes, including a heart attack in progress, clogged coronary arteries, and muscle spasms induced by stress or anxiety.
“Yes, in extreme cases of stress and anxiety, the chest muscles can tighten just like other muscles in the body in a very anxious and stressed-out person,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“The chest muscles when they do spasm can cause wavering chest pain that can sometimes be mistaken for chest pain related to the heart, and can make people panic and make a trip to the ER.”
If this seems to be happening to you, get a complete exam by a cardiologist to make sure that any symptoms you’re having are not related to your heart.
Stress and anxiety can also cause chest pain as a result of a condition called angina pectoris:
The anxiety or stress increases the body’s oxygen demands, forcing the heart to pump harder.
“Due to constricted arteries (because they’re clogged with plaque), oxygen flow is compromised, resulting in “chest pain,'” says Dr. Sayeed.
COMPARISONS
“The differentiation between muscular and real chest pain can be made by pressing on the chest muscles which may be tender or may be relieved with pressure, whereas this would not occur with real chest pain,” explains Dr. Sayeed.
So next time you experience this symptom, see what happens by stretching your pec muscles.
This can be done by placing both forearms against the outer portion of a door frame and leaning forward.
Another thing to do is to flap the arms back and forth while holding them in a horizontal position, palms facing forward. These motions may make the symptom disappear or diminish.
However, Dr. Sayeed adds, “Also, having the person move or twist their upper body and their arms can sometimes worsen such spasm pain, whereas real cardiac chest pain would not change.”
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Robert Kneschke

Cause of a Stabbing Severe Chest Pain but All Tests Are Normal

Wait till you find out the likely cause of sharp, stabbing chest pain when all your heart tests keep coming back normal.
If you’ve been having sharp, stabbing or otherwise severe chest pain, but the doctors “can’t find what’s wrong” after giving you all sorts of tests, don’t assume nothing is wrong.
That’s because … something probably is wrong.
Probable Cause of Severe Chest Pain when Tests Come Back Normal
“This type of stabbing, ripping chest pain with normal tests is seen with acute pericarditis, especially in younger people,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“This is an inflammation of the sac that surrounds the heart, and when it gets irritated classically causes stabbing chest pain,” continues Dr. Sayeed.
Acute pericarditis can be missed.
“Oftentimes, lab tests, EKG, chest x-ray, echo are all normal, particularly very early in the course,” says Dr. Sayeed. The symptoms can be anywhere from mild and brief up to a day or two, to more severe and long-lasting up to several months.”
The sharp stabbing pain may be in the middle of the chest (behind the breastbone or sternum) and/or on the left side. Of note, the pain isn’t always of a piercing or stabbing nature. It may also be dull or aching.
In either case it may radiate to the left shoulder and even the neck. The discomfort, wherever it is located, may get worse when you inhale deeply, cough or lie down.
Other symptoms may be swelling in the stomach or a leg, weakness or fatigue, and shortness of breath which may be worse upon lying down.
If symptoms last longer than three months, the situation is considered chronic.
Treatment for Acute Pericarditis
Dr. Sayeed says, “It is usually treated with high dose NSAIDS for one month. ” A NSAID is a non-steroidal anti-inflammatory drug. If not treated in a timely manner, it’s possible for this condition to result in a fatal heart arrhythmia or permanent scarring of the pericardium.
Though a person may prefer that any sharp or stabbing chest pain be the result of pericarditis rather than a heart attack, one must never take the mindset of “It’s just pericarditis.”
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Does a Zero Calcium Score Always Mean a Healthy Heart?

The coronary calcium scoring procedure is very accurate at predicting the likelihood of the presence of heart disease, but does this mean that a result of zero automatically means you can’t possibly have any heart disease?
“Yes, even if the calcium score is zero, one can still have some form of heart disease,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“A calcium score of 0 usually means that there is no significant coronary artery disease, or there may be coronary artery disease in the form of a soft non-calcified plaque that can still rupture and cause a heart attack.”
The test that can show this soft, non-calcified plaque is the CT angiogram.
If you have soft plaque, it won’t necessarily be built up enough to restrict blood flow in your heart (and cause chest pain).
The type of plaque that restricts blood flow is the hard, calcified type.
Thus, if a person has angina (chest pain from “clogged” arteries restricting blood flow), this doesn’t mean they also have a lot of soft plaque too; in fact, there’s no correlation.
A person can have a calcium score of 1,000 and chest pain from exertion, yet have very little soft plaque.
He may never have a heart attack — unless the hard plaque builds up enough to literally obstruct the vessel, blocking 100 percent of the blood flow through it.
This isn’t a rupture. A rupture of soft plaque means a piece of it has broken off and has lodged in what can be an otherwise clear vessel, blocking blood flow.
Imagine a pea inside an otherwise clean straw. Imagine that the pea-sized blockage broke off from a larger mass of the “pea” further upstream from that point, in a wider vessel.
“Even though there may be a minor buildup of soft plaque, it can still rupture,” says Dr. Sayeed.
“A zero calcium score only tends to rule out significant coronary disease, but it doesn’t mean that the structure of the heart is normal or that the pump function or the valvular function of the heart is normal,” says Dr. Sayeed.
“These could all be a problem and yet the calcium score can be 0 and be misleading.”
An echocardiogram will reveal cardiac structure, pump and valvular function.
“Even if the calcium score is 0 and no soft plaques are obviously detected, there may still be vulnerable plaques that are too small to be seen and can cause the so-called healthy person heart attack or sudden death.”
What can you do to reduce soft plaque or stop the progression of soft plaque?
BruceBlaus
- Green tea supplementation
- Magnesium citrate supplementation
- Krill or cod liver oil supplementation (high doses)
- Avoid manmade sugars as much as possible.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/goodluz

Can Resting Pulse in 90s from Stress Harm the Heart?

Find out what can happen if stress is causing your resting heart rate to be in the 90s.
Have you noticed that whenever you take your resting heart rate, it’s in the 90s, even though you’ve been at rest, have not smoked, have not ingested a lot of caffeine and are negative for hyperthyroidism or anemia (which both cause high resting heart rate)?
Frequently being in a state of anxiety or chronic stress can cause the resting heart rate to often register in the 90s.
Anxiety and stress trigger the body’s “fight or flight” response, which elevates heart rate as part of the body’s way of preparing to deal with perceived threats.
When this occurs often enough, it can lead to a persistently high resting heart rate.
The body remains in a heightened state of arousal, causing the heart to beat faster even when you are at rest.
Can this cause harm to your heart, even though otherwise you’re healthy?
“Resting heart rate in the 90s is still usually considered normal,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“The Mayo Clinic defines a normal heart rate as between 60 and 100. So being in the 90s is still considered to be normal and likely won’t harm the heart.”
But isn’t a slower resting heart rate better?
“Of course, if possible, it is always better to have a lower resting heart rate if possible, closer to the 60 goal,” says Dr. Sayeed.
“This is due to the fact that higher heart rates tend to cause increased production of inflammatory molecules and reactive oxygen species which can damage the heart, and a higher heart rate tends to cause more mechanical stress on the heart.”
If you can’t avoid situations that cause stress, or are prone to feeling a lot of anxiety, even to trivial triggers, you can fight against a resting pulse in the 90s by consuming a lot of fresh vegetables and fruits, which are high in antioxidants, and these will help neutralize the reactive oxygen species.
Another way to help bring the resting pulse down from the 90s is to regularly engage in rigorous or even moderate-intensity cardio exercise.

Shutterstock/Liderina
“In someone with coronary disease or heart disease already present, higher heart rates can lead to ischemia (blocked oxygen supply) and further damage to the heart,” says Dr. Sayeed.
When you engage in consistent aerobic activity, your heart becomes more efficient at pumping blood.
This efficiency means that with each heartbeat, your heart will pump a larger volume of blood, so it won’t need to beat as frequently to circulate the same amount of blood throughout your body.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She is also a former ACE certified personal trainer.

Can Angina Occur at Rest but Not During Exercise?

Find out if it’s possible to have angina at rest but not during or resulting from exercise or physical activity.
You may know that it’s possible to experience angina during exercise or physical exertion, but not at rest, since cessation of the activity brings down the body’s oxygen needs, imposing less burden on the heart.
This is called stable angina.
However, unstable angina is when an episode can occur at rest, even during sleep.
“In general, if someone has angina at rest, this angina will only get worse with exertion because the heart is beating faster and needs even more oxygen which it is not getting” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“There are rare instances where angina at rest may go away with exercise, and this could only happen if the heart were to recruit more collateral blood supply with exercise that might increase blood supply.
“But in general, this is usually extremely rare and not seen.”
But there is a specific condition that can cause angina while at rest, which is not related to coronary artery disease (plaque buildup), heart valve problems or chronic heart failure. It’s called Prinzmetal’s angina.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Korawat photo shoot

Why Resting Heart Rate Speeds Up Later in the Day

A cardiologist explains what causes resting heart rate to speed up as the day goes on.
“The resting heart rate is the lowest at night while sleeping as well as during the first minutes after awakening, provided the person did not wake up abruptly from a dream or jump out of bed,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Take your pulse first thing in the morning, before exiting bed or eating anything.
“It is in the calm lazy waking type of day. The resting heart rate will not increase by too much over the course of the day, but will be higher than what it was during sleep or first wakening due to mainly physical activity, stress, anxiety, circadian rhythm, etc.,” says Dr. Sayeed.
“Caffeine in fact at doses in regular coffee that people drink will actually lower resting heart rate due to its blood pressure increasing effects.
“High doses of caffeine such as in energy drinks and maybe huge cups of coffee will increase resting heart rate as will nicotine.”
There is no heart disorder that causes the pulse to become fast as the day or evening wears on.
Cardiac conditions that cause a rapid heartbeat do not care what time of day it is. So don’t worry if your pulse becomes elevated only in the evening.
Free-floating anxiety, which is when a person persistently has elevated adrenaline levels due to frequently feeling anxious, nervous or fearful, will cause resting heart rate to climb over the course of the day, maybe topping out at about 20 BPM more than what it was in the morning.
How to Help Control an Evening Elevated Heart Rate
Stress management should be implemented. So should an inventory of things that usually happen to you later in the day.
You may find that stressful situations tend to concentrate later on or in the evening, thus jacking up resting heart rate.
Thirty minutes of rigorous exercise will do wonders to help neutralize stress hormones.
If you’re already exercising throughout the week, make sure that your workout time is actually dedicated to working out, rather than telling yourself, “I got my exercise cleaning up the kids’ rooms today.”
Examples of dedicated time for vigorous exercise includes brisk walking outdoors that includes hilly areas; jogging in a park; a fitness class; and a weight or resistance workout.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}