
Why Do Colonoscopies Normally Begin at 45? Why Not Sooner?

There’s good reason why 40 is that “magical” number for when a typical person should begin getting colonoscopies for colon cancer screening.
A colonoscopy is a minimally invasive procedure that can detect colon cancer, or precancerous polyps.
“Colon cancer is generally a disease of the elderly,” says Mitchell S. Cappell, MD, Chief, Division of Gastroenterology & Hepatology, William Beaumont Hospital, Royal Oak, MI.
“Nearly 95 percent of colon cancers occur in people more than 50 years old.
“This phenomenon is due to the fact that colon cancer generally comes from chance biochemical abnormalities, called mutations, in the genes (DNA) of individual colon cells.”
Colon cancer (like all malignancies) does not happen overnight; there are a number of stages of transformation that a healthy cell undergoes before it becomes a malignant cell.
In the case of colon cancer, a normal cell, due to accumulated mutations, will proliferate out of control, initially forming a benign polyp – which a colonoscopy can detect. On the spot, the physician removes the polyp(s).
If you don’t have screening for colon cancer, the polyp will continue growing and may sustain more mutations – enough to morph it into a malignant tumor.
Dr. Cappell explains that this disease “occurs mostly in the elderly because this sequence of changes, the accumulation of chance mutations, is a long process that takes many years.”
This doesn’t mean that people younger than 45 are immune to colon cancer.
Dr. Cappell adds, “About 2 percent of people developing colon cancer are younger than 40 years old.
“About 20 percent of people who develop colon cancer when less than 40 years old have special risk factors that place the patient at a very high risk of developing colon cancer.”
These risk factors are 1) familial polyposis coli (abbreviated as FPC), and 2) Lynch syndrome (also called HNPCC).
In FPC, patients have many benign polyps, and malignancy is likely because out of so many polyps, it’s inevitable that one or more will become malignant.
In Lynch syndrome, the patient develops just a few benign polyps, but these particular polyps have an intrinsically high risk of morphing into colon cancer.
“Patients less than 50 years old generally do not undergo screening for colon cancer because they have much lower risks than patients more than 50 years old,” continues Dr. Cappell.
If someone is diagnosed with FPC or Lynch syndrome, he or she will be urged to have colonoscopies beginning at a much younger age.
Just how young can a person getting a colonoscopy be?
Dr. Cappell says, “Patients with a close blood relative with familial polyposis coli need colonoscopy at a young age, during their early teens, to diagnose or exclude this disorder.
“Likewise, close blood relatives of patients with Lynch syndrome need early colonoscopy beginning in their mid-20s.
“Patients with a family history of colon cancer in first degree relatives (e.g., mother or father) should generally undergo colonoscopy at age 40 years or earlier.”
So if you’re 25 and have no family history of this dreadful disease, and do not have Lynch syndrome or FPC, this does not give you the green light to practice lifestyle habits that are risk factors for colon cancer, such as:
1) a sedentary lifestyle, 2) a meat-based diet, 3) eating lots of processed meats, 4) diet low in fiber, high in “bad” fats, and 5) smoking and heavy drinking.
You have no green light because, as Dr. Cappell explains, colon cancer (in the absence of Lynch syndrome or FPC) is decades in the making, and how you treat your body during your younger years influences your risk of developing the disease.
Dr. Cappell says, “In summary, colon cancer usually occurs in patients more than 50 years old, and colon cancer is unusual in patients less than 50 years old. However, no age group is immune from colon cancer.
“I saw and diagnosed one patient with incurable colon cancer at age 20, a few weeks before his planned wedding.”
Symptoms of this Common Disease
Constipation, diarrhea, and especially with a recent dramatic shift in bowel movements (such as from regular bowel movements to constipation); blood in the stools (may be bright red, or tar-like); abdominal pain; abdominal bloating; unexplained weight loss; unexplained fatigue; and appetite suppression.
Note: Having some of these symptoms doesn’t mean you have the disease.
In fact, the symptoms of irritable bowel syndrome can be very similar, though over time, in untreated colon cancer, the symptoms will get worse.
“Colon cancer may also present as anemia due to iron deficiency unexplained by blood loss during menstrual periods or by numerous childbirths,” says Dr. Cappell.
“Patients should routinely undergo screening colonoscopy at age 50 years even without symptoms or risk factors for colon cancer.”
Recommended Age to Begin Screening for Colon Cancer Drops in May of 2021
The U.S. Preventive Services Task Force (USPSTF) updated their guidelines in 2021 to recommend that individuals of average risk begin colon cancer screening at age 45.
This recommendation applies to people who are at average risk for colorectal cancer and doesn’t take into account any other risk factors like family history or genetic predisposition.

Dr. Cappell has been in practice for over 30 years.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Nasal Congestion Relief: Humidity vs. Dry Air

You’ll be surprised which turns out the winner between humidity and dry air when it comes to nasal congestion relief, and why.
The kind of air you breathe, in terms of how dry it is or humid it is, can significantly impact the perception of nasal congestion.
The feeling that you have congestion, or a stuffed-up nose, is not necessarily related to actual mucus buildup in the sinuses.
Rather, the sensation of a stuffy nose can originate from the airflow through the nasal passages.
“It’s very common for the nose to feel congested or blocked without mucus,” says Inna Husain, MD, an ear, nose and throat specialist with Community Healthcare System of Indiana.
“The lining and tissue of the nose can congest and decongest in response to inhalant allergies, but what most people don’t know is that it is also affected by non-allergic stimuli such as temperature.”
This can explain why your nose feels stuffed or blocked, yet no matter what you do, nothing comes out, even after irrigating the nose.
The Monell Chemical Senses Center
Monell Center researchers found that the sensation of nasal congestion relates to air temperature and the level of humidity.
So if you’re one of the 33 million people in the U.S. with a nose that feels blocked up, keep reading.
Perhaps you’ve seen a doctor and he couldn’t find any physical cause of your sinus congestion.
You may actually have a sensory-related issue.
When the feelings of nasal congestion are sensory-related, says the research, this opens doors for more targeted treatment.
One example of a targeted treatment is that of focusing on restoring the optimal humidity and temperature in a patient’s nasal airflow.
The Monell study had 44 healthy participants breathe air from three boxes and then rate any symptoms of a nasal congestion.
One box contained cold air; the second box contained room temperature dry air; and the third offered room air that was at normal humidity.
Which box produced the lowest report of sinus congestion? The cold air box.
Reduced nasal congestion was also perceived when the participants inhaled from the dry air box.
The room air, normal humidity box did not result in these perceptions.
In short, lower humidity was found to be associated with reduced sensations of nasal congestion.
Nasal cooling is influenced by the interaction of humidity and air temperature as air moves through the nose’s cavities, say the researchers.
“Cool sensors” in the nose detect the nasal cooling, and the detection can feel like easy breathing — or obstructed.
The researchers point out that if someone is in a desert, with all other things being equal, they should feel less congested than if in a jungle.
That’s becauuse a desert has low humidity. This means more evaporative cooling inside their nose, making the temperature of their nasal passages lower.
This creates the sensation of a greater airflow.
Additiona Reasons for a Blocked Feeling in Both Nostrils

Shutterstock/natali_ploskaya
“There is also a process known as the nasal cycle which is the spontaneous congestion and decongestion of nasal mucosa that cycles side to side,” says Dr. Husain.
“Also, nasal congestion or obstruction can occur due to structural reasons in the nose — for example, a septal deviation.”
 Dr. Husain is an otolaryngologist affiliated with Community Hospital, Munster, IN, Community Stroke and Rehabilitation Center, Crown Point, IN, and St. Catherine Hospital, East Chicago, IN. She received her medical degree from Southwestern Medical School at Dallas. Follow her on Instagram and TikTok.
Dr. Husain is an otolaryngologist affiliated with Community Hospital, Munster, IN, Community Stroke and Rehabilitation Center, Crown Point, IN, and St. Catherine Hospital, East Chicago, IN. She received her medical degree from Southwestern Medical School at Dallas. Follow her on Instagram and TikTok.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2011/10/111013184803.htm

Hearing Loss from Motorcycles: Engine vs. Helmet Wind

Which is worse for the motorcycle rider’s hearing: the roaring engine or the roaring wind?
Hearing loss is a real threat to the toughest motorcycle rider, and it seems as though the volume of wind noise gushing past a helmet has gotten much more attention than the volume of the bike’s engine.
“Both can be damaging to the ear — but surprisingly few motorcyclists realize the risk to their ears,” says Rivka Strom, AuD, CCC-A, chief audiologist at Central Hearing LLC in NY.
“Studies have shown wind noise to be high in level and increasingly louder as the speed picks up.
“Although there are helmets to protect motorcyclists’ ears, they are not always efficient at reducing necessary levels, and each one must be evaluated for effectiveness for the rider.”
A Study Shows the Loudness of Wind Against a Helmet Using Microphones
A study in 2011 by researchers at the University of Bath and Bath Spa University placed microphones at varying locations around a helmet that was on a mannequin’s head, to determine the precise location of greatest volume of wind noise (produced by fans for this study).
However, it had, by the time of the study, already been well-documented (e.g., McCombe) that the “whooshing” wind sound over a biker’s helmet as he speeds down roads will surely lead to some degree of hearing loss.
The greater attention to the helmet issue may be because few motorcycle riders would ever suspect wind rushing over a helmet as a possible cause of hearing loss.
Though the helmet wind volume may exceed a particular bike’s engine volume, this in no way invalidates the potential for motorcycle engines to play a prime role in hearing loss.
Consider that often, a biker will rev the engine while in idle. The biker gets plenty of loud-engine exposure without the noise of wind stealing the show.
So just how loud is a motorcycle’s engine?
University of Florida researchers revved up the engines of 33 different bikes:
About half delivered volumes over 100 decibels (a dB is a unit of sound volume). In fact, at 65 mph, a motorcycle’s engine can reach up to 116 dB.
The Occupational Health and Safety Administration warns that exposure to 100 dB is safe for only 15 minutes.
The University of Florida report says that nearly all the motorcycles that were tested reached “action-level noise, which in the workplace would require ear protection.”
A motorcycle enthusiast may think, “Well, what’s a little damage from my engine or helmet, what with all the rock concerts I attend?”
A rock concert can generate volume at 120 dB, which, according to OSHA, is safe at only seven and a half minutes of exposure!
The motorcycle rider may also figure why bother worrying about engine and wind noise, when he spends a lot of time using power tools?
Every bit of concern helps.
A motorcycle rider should wear earplugs. Custom-made work best and last a lot longer than store-bought ones.

Dr. Strom is a member of the American Speech Language and Hearing Association and has received several awards including Brooklyn College’s Excellence In Audiology Award.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources:
sciencedaily.com/releases/2011/07/110729175559.htm
ncbi.nlm.nih.gov/pmc/articles/PMC539364/ mcCombe
hear-it.org/page.dsp?page=3597
motorcyclecruiser.com/streetsurvival/0710_crup_motorcycle_hearing_protection/index.html

Baldness Increases Skin Cancer Risk; Bald Men Beware

Bald men need to be aware that, though bald may be beautiful, bald can also be deadly.
Though skin cancer that grows on the scalp comprises only 2 percent of all skin cancers, this is actually a significant percentage, because every year in the U.S., over a million skin cancer cases are diagnosed.
Two percent of one million is 20,000. If you’re balding, that figure is nothing to sneeze at.
“The top of the head (and back of the neck) is something many guys forget about,” says Adam J. Mamelak, MD, a board certified dermatologist and founder of Sanova Dermatology in Austin, TX.
According to the journal Dermatologic Surgery, a certain type of skin cancer of the scalp can be particularly aggressive.
This skin cancer is called squamous cell carcinoma, and about 250,000 Americans are diagnosed with it every year.
A balding and especially completely bald head is highly vulnerable to sun damage.

Freepik.com
In fact, according to the Journal of the American Academy of Dermatology, about 90 percent of visible changes to skin are incorrectly blamed on aging, when in fact, they are caused by sun damage.
So why is that bald head at such notable risk for skin cancer?
First of all, think of all the exposure a bald head or partially bald pate gets to the sun.
Secondly, people tend to subscribe to the idea that if you can’t see something, you don’t need to worry about it.
How many bald or partially bald people even occasionally take a look at their scalp, let alone inspect it on a monthly basis?
Other variables are at play here, because a bald man may be tall; how many family members are taller than him such that they can spot suspicious lesions on top of his head?
If the baldness is the type where sparse strands of hair are combed over the skin surface, the presence of the hair can mask much of the cancerous or precancerous lesions.
And here’s another variable: A man may think he has a full crop of hair on top of his head, when in fact, he has a nice bald spot there, one that exposes skin to significant amounts of sun.
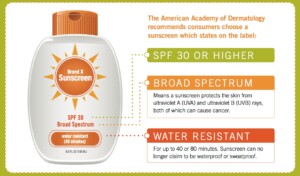
And if you are bald, and you faithfully use sunblock, when’s the last time you actually applied sunblock to your scalp, especially if you have sparse strands of hair over it?
“You can apply sunscreen to the top of the head,” says Dr. Mamelak. “It works well, just like it does on other parts of the body.
Sparse strands of hair, or the infamous “comb-over,” do not protect skin from cancer.
“Wearing a hat, however, is probably the easiest and best way to protect your head from harmful UV rays,” says Dr. Mamelak.
“A hat with a wide brim is even better, as it shades and covers the ears from sun damage.”
Does your primary care physician examine your scalp during annual physicals?
Request that your doctor do so, even if you yourself have been doing so (which should be monthly).
The layperson can miss an early squamous cell carcinoma, basal cell carcinoma and precancerous lesions.
In fact, precancerous lesions can be very faint and hardly visible. Have your partner inspect your balding pate on a monthly basis.

The light pink patch is a precancerous lesion. Source: Future FamDoc/CC
 Dr. Mamelak focuses on the full breadth of dermatologic care, from cosmetic skin solutions to advanced skin cancer removal. He’s founder of the Austin Mohs Surgery Center, which is dedicated to the treatment and management of skin cancer.
Dr. Mamelak focuses on the full breadth of dermatologic care, from cosmetic skin solutions to advanced skin cancer removal. He’s founder of the Austin Mohs Surgery Center, which is dedicated to the treatment and management of skin cancer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Razoomanet
Source: skincancer.org

Can a Mole Turn into Squamous Cell Carcinoma?

Normal mole under magnification
Can a normal mole ever turn into squamous cell carcinoma, which kills about 3,500 Americans every year and is considered the second-deadliest of all skin cancers?
It’s a good question: Is it ever possible for a squamous cell carcinoma to arise from a pre-existing typical mole.
“No, we do not usually see squamous cell carcinoma arising from a mole,” says Dr. Susan Weinkle, a board certified dermatologist with a private practice in Bradenton, FL.
Thus, as you may already know, the deadliest skin cancer, melanoma, comes from moles in about 25 percent of melanoma cases, but moles cannot turn into squamous cell carcinoma.
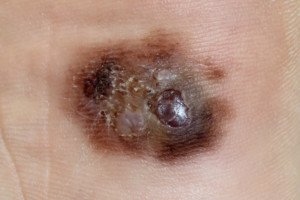
What does squamous cell carcinoma look like?

Squamous cell carcinoma. Shutterstock/Dermatology11
Dr. Weinkle explains: SCC usually appears as growing lumps, often with a rough, scaly, or crusted surface.
They may also look like flat reddish patches in the skin that grow slowly. They commonly occur on sun-exposed areas of the body such as the face, ear, neck, lip, and back of the hands.
Sometimes, they form in the skin of the genital area and they can also develop in scars or skin ulcers elsewhere.”
A precancerous skin condition called actinic keratosis can have the appearance of early squamous cell carcinoma.
Some dermatologists actually consider actinic keratoses and SCC to be on the same continuum, or, to put it another way, actinic keratosis is squamous cell carcinoma in its earliest form.
However, this is not the general consensus among dermatologists. If left untreated, most actinic keratoses will not morph into squamous cell carcinoma.
And when they do, it takes years for this to happen. If you’ve been diagnosed with actinic keratosis, don’t panic; don’t get alarmed.
Actinic keratoses are curable, and only rarely (5-10 percent) become squamous cell carcinoma, and that’s when they are left untreated.
And out of those that become squamous cell carcinoma, only 10 percent actually spread to other parts of the body – and those are the ones that are not caught early enough to be cured.
Most squamous cell carcinomas are slow-growing, and when they spread, it’s because the patient either:
1) became aware of it but brushed it off as a sign of aging or nothing to worry about, or 2) the tumor developed in a location that the patient didn’t readily see, such as behind an ear or on top of the head.
It’s important to check your moles every month, as well as non-mole areas of skin, for any suspicious spots or new lesions, including squamous cell carcinoma, and have a dermatologist check your skin annually.
 A skilled surgeon with 30+ years’ experience, Dr. Weinkle is also a Fellow in the American College of Mohs Surgery. She is past President of the American Society for Dermatologic Surgery.
A skilled surgeon with 30+ years’ experience, Dr. Weinkle is also a Fellow in the American College of Mohs Surgery. She is past President of the American Society for Dermatologic Surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Will Having Normal Moles Removed Prevent Melanoma?

Melanoma can arise from a pre-existing mole, so you might be thinking that it’s smart to have your normal moles removed to at least prevent the development of melanoma from these moles.
If you have many moles, the idea of having them electively removed will be even more appealing, since having many of these skin lesions is one of the risk factors for melanoma.
Having moles electively removed, out of melanoma fear, can also be referred to as “de-moling.”
However, “The principal always followed in medical care is according to Hippocrates’ oath, ‘First do no harm,’” says Maria M. Tsoukas, MD, PhD, Assistant Professor, Dermatology Section, University of Chicago.
In medicine and specifically in dermatology, we keep a very low threshold in clinical examination and in deciding which nevi need to be biopsied or removed.”
A nevus is the Latin term for mole, and nevi is the plural form. “Pending on each individual case history and clinical exam as well as family history of melanoma, we decide which moles need to be removed,” says Dr. Tsoukas.
“We are focused on clinically appearing atypical nevi that under microscopic examination may have some abnormal features; however, do not meet all criteria to be identified as malignant melanoma.”
A patient may be concerned about one or two particular moles, perhaps due to size (they’re bigger than all the others on the patient’s body), or maybe they stand out because they’re darker than the rest.
For peace of mind, the patient then decides to have the moles electively removed. After all, the mindset might be, I know I can’t prevent melanoma from arising anywhere in my body, but at least I can prevent it from developing in these two particular moles.
Insurance won’t cover the cost of this if the only reason is peace of mind or anxiety.
Reimbursement logistics aside, Dr. Tsoukas says that in medicine, management and intervention are justified based on certain criteria and facts.
Otherwise, somebody would have medical care or intervention randomly decided.
Another reason that a person may have a mole electively removed is because of its location; it’s difficult for the individual to examine the mole as part of routine monthly skin exams.
But what if you have a lot of moles peppered all over your body?
It’s not practical to have every one of these spots systematically cut out or even “shaved” off.
On the other hand, what if many of these moles are on your back, which compounds the difficulty in keeping track of them for possible changes?
How do you draw a “mole map” of the spots on your back, unless you have an elaborate set-up with mirrors that frees up your hands (for sketching) and provides a clear view?
What if your ability to draw spots in a “map,” that accurately aligns with what you see in the mirror, is in sad shape?
And add to that this: Elective removal of many moles will cost a pretty penny and create a lot of hassle due to bandaging and removal of stitches.
If you have many skin lesions, including normal looking ones, it’s wise to get a yearly full-body skin exam.
A dermatologist will address moles that are clinically benign, those that show atypical features, and those that should be removed and biopsied.
“In addition,” says Dr. Tsoukas, “dermatologists use the mole mapping technique which combines photography, dermoscopy and a body map file created and saved electronically for each patient.”
In addition to the skin exam, your dermatologist will explain additional risk factors for melanoma, which include skin type, family history of melanoma, sunburn history, age and even history of medications you’ve taken. You will also learn about sunscreen protection.
Dr. Tsoukas’ clinical interests include diagnosis and management of patients at high risk for skin cancer, cutaneous oncology, laser surgery and aesthetic dermatology.
clinical interests include diagnosis and management of patients at high risk for skin cancer, cutaneous oncology, laser surgery and aesthetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Suspicious Mole? Get Biopsy; Don’t Rely on Handheld Lenses

Only a biopsy has the final word on whether or not a worrisome mole contains melanoma cells or is entirely a melanoma.
That suspicious mole should be biopsied, even if your dermatologist says it “probably isn’t” melanoma after viewing it through a handheld lens known as a dermoscope or dermatoscope.
Though statistically, chances are in your favor that the questionable mole is benign, you should still get a biopsy.
“Whether you feel uneasy or your doctor is recommending a biopsy for a suspicious spot, it’s important to get the spot checked,” says Dr. Gretchen Frieling, MD, Triple Board Certified Boston Area Dermatopathologist.
“When you feel nervous about a spot, you can consult your skin specialist who will assess the spot and recommend a biopsy,” continues Dr. Frieling.
“If the doctor feels the spot may be something else, they can advise you accordingly. But when it comes to melanoma, the benefit of getting tested and finding the condition in time outweighs any risk of being overly cautious.”
Though melanoma has gotten a lot of media attention over the years, and coverage seems to be increasing, it’s still rare for moles to transform to melanoma.
However, about two-thirds of melanoma tumors arise in areas of skin where there was no pre-existing mole.
At Frontiers in Optics 2010 (Oct. 24-28), Duke University scientists presented a new technique for aiding dermatologists in helping to differentiate normal moles from melanomas, by using high-resolution snapshots of moles that appear suspicious.
About 25 percent of dermatologists use a dermatosope for routine checks of a patient’s moles.

Dermatoscope. Shutterstock/LightField Studios
Certainly, you can imagine how long it would take for a routine skin inspection if the doctor used the dermatoscope to inspect every one of a patient’s 150 moles. Some people have even more moles.
On the other hand, some doctors don’t use this tool even for patients with a small number of moles.
It’s perfectly okay for the patient to request that the practicioner use this special magnifying device.
But this special lens is not a diagnostic tool. Though it enables the doctor to see things that he can’t with the naked eye, it’s still no match for a biopsy.
My doctor took me by surprise during one of my annual skin exams by saying, “You have a mole on your upper arm that gets my attention, and I’d like to get a biopsy on it.”
This was after she examined it with the dermatoscope. (The biopsy was done – entire mole removed).
She said a few times that it was “probably benign,” but you’ll want your doctor to always be ahead of the wave. My mole turned out to be benign.
In short, a mole that gets even only the attention of the patient should be biopsied. Trust your gut.
Cancerous changes can take place too deep within the mole to be seen with the handheld lens, though there are cases in which the physician not only can clearly see cancerous signs with the instrument, but with the naked eye as well.
However, there are times when even a biopsy nets disagreement among doctors.
So what about that study?
The Duke researchers proposed a two-photon microscopy technique that infuses a small quantity of energy into the two kinds of pigments that are found in skin: pheomelanin, and eumelanin.
The energy redistributes to yield high-resolution images of the pigments’ distributions, indicating possible melanoma or not.
“No one has been able to look at where different melanins are organized in skin,” says the lead researcher in the report. “This opens up a whole new pathway of looking for melanoma.”
At any rate, whenever you have a mole removed, even just for cosmetic purposes, insist upon a biopsy, just to play safe; a normal looking mole may end up being melanoma after all.
 Dr. Frieling’s website is gfacemd.com. In addition to 15+ years of experience in dermatology and dermapathology, Dr. Frieling provides advanced micro-enhancement techniques to optimize the health and beauty of her patients’ skin.
Dr. Frieling’s website is gfacemd.com. In addition to 15+ years of experience in dermatology and dermapathology, Dr. Frieling provides advanced micro-enhancement techniques to optimize the health and beauty of her patients’ skin.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Albina Glisic
Source: sciencedaily.com/releases/2010/10/101020194811.htm

Mole Removal with Laser Causes Regrowth of Moles

If you want a mole removed with a laser, the mole might grow back.
Traditionally, the idea is that a laser beam will penetrate the mole’s surface area to disintegrate any abnormal cells, and the expectation is that any remaining cells will be absorbed by the body.
But there’s a problem: Laser light can rejuvenate skin cells, and this includes mole cells.
In fact, not only can laser treatment cause moles to grow back, but it can also cause a regrowth of other skin deviations that a person believes will be removed with laser treatment.
“The latest research conducted on the effectiveness of lasers, and its use for mole removal, revealed laser treatments stimulated growth of moles, warts, and skin tags, causing many to reappear after removal,” says Dr. Geoffrey Rappert, a member of the American Board of Dermatology, speaking in a hospital interview, as presented in a news release.
This doesn’t mean that every single laser mole removal treatment results in the spot growing back.
It means that sometimes the mole grows back. “This has to do with the way laser light gently donates energy or waves of photos causing rejuvenation of the cell,” says Dr. Rappert.
Another Reason a Mole Grows Back After Laser Treatment to Remove It
“The only way to [completely] remove a mole is surgically,” says Adarsh Vijay Mudgil, MD, double board certified in dermatology and dermatopathology, and founder of Mudgil Dermatology in NY.
“Lasers can reduce/eliminate pigmentation (they target melanin, not the melanocyte itself).”
A melanocyte is a specialized cell in the skin that produces the pigment in a mole. The pigment is called melanin.
“Moles that are treated with laser have a very high rate of recurrence, because if the melanocyte itself remains viable, it can resume the production of melanin,” says Dr. Mudgil.
Why then, settle for laser treatment?
Even if your desire to have a pigment spot removed is purely cosmetic, or for convenience (e.g., the mole keeps getting rubbed by clothing), you may as well rely upon more effective, sure ways of treatment: freezing or excision by a dermatologist.
And, if you’re going to have a mole removed, it’s always smart to have it biopsied, even if it looks normal.
I once read about a very young woman who, for cosmetic purposes, had a large mole on her shoulder removed.
Apparently, the doctor removed only the superficial portion, leaving behind portions of the growth beneath the skin.
Because this was a cosmetic procedure, the patient was satisfied because the pigmented area was no longer visible. But this didn’t mean the melanocytes were no longer there.
They were. And what remained there in the young woman eventually morphed into melanoma skin cancer.

Melanoma. Laurence Meyer, MD. cancer.gov
At the initial visit just to have the spot removed, the doctor threw away the portion he had removed, instead of sending it out for a routine biopsy.
He didn’t use laser removal for the mole; he cut it out, but didn’t go deep enough.
At Kaiser Permanente, if you go in to have a mole removed purely for cosmetic purposes, they will automatically send it to the pathology lab for a biopsy, even if it looks normal.
Yes, this will create an additional out-of-pocket expense to patients, but it can be life-saving.
The woman who had the shoulder mole removed eventually died from her melanoma.
It has been speculated that had her doctor sent the removed portion to be biopsied, that the early stages of melanoma could have been detected.
 Dr. Mudgiltreats infant to geriatric patients, and is versed in all aspects of medical, surgical and cosmetic dermatology. He has published extensively in the medical literature plus has lectured at numerous national meetings.
Dr. Mudgiltreats infant to geriatric patients, and is versed in all aspects of medical, surgical and cosmetic dermatology. He has published extensively in the medical literature plus has lectured at numerous national meetings.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock, Ekaterina Vidyasova
Source: prweb.com/releases/mole-removal/treatment-options/prweb868604.htm

Mole Mapping at Home: Melanoma Screening Techniques

Learn how to produce a very reliable mole map at home for melanoma screening.
I have been “mole mapping” for three years and have learned along the way some excellent mapping techniques, for melanoma screening.
The technique I will describe has one caveat; you must be able to illustrate.
If a mole is on a part of your body that allows you to visually inspect it while your dominant hand draws it, this is a great mapping technique.
I was once watching a mole on my upper inner thigh, and decided to draw it. I held a magnifying glass over it, and with my dominant hand, drew and rendered what I saw.
In order for illustrative mapping to be reliable, you must be able to capture the mole’s nuances, subtle tone variations and other details – and draw them to an enlarged scale.
I drew the mole a lot bigger than its actual size (which was about 2 millimeters).
I drew another one that was on my lower abdominal region (it actually turned out to be a seborrheic keratosis, which can look very much like a mole; it had changed in appearance so I drew it).
The drawing should be a rendering, not merely a line drawing.
This way you can monitor for changes in color tone variation. Another reason to render is because often, the tone variation is gradual or gradated, rather than with a definitive demarcation.
With an illustration at hand, every time you check the mole, you don’t have to wonder if you’re imagining that a certain part of it is darker; or if the darker part of it has spread to fill up more of the mole; or if a darker or lighter part of it has changed shape or spread to take up more of the mole.
Because all you need to do is refer to the illustration, and you can see exactly how the spot appeared last time you checked it, and match the drawing up to what you’re now seeing.
Another way to illustratively do mole mapping is to imprint in your mind what the particular spot looks like.
This is applicable for moles that are located in areas that make it impossible to draw them.
I had one on the back of my neck that I thought was changing, so I imprinted it in my mind: border shape; the shape of the darker portion of it; any gradations.
With a ballpoint pen I drew it enlarged to scale and rendered it. I then monitored it based on this illustration. Soon after, a dermatologist said it was a seborrheic keratosis (these can change).
Being an illustrator also means you can measure whether or not a tiny mole is getting bigger. A “birth mark” on my shin had taken on a reddish tinge, but it was not bigger.
In anticipation that it might be getting bigger (since it was changing colors), I drew this little spot with a pencil to its exact size, on the edge of an index card.
I then could place the stiff edge of the card perpendicular to my shin, against my shin, just a tiny bit away from the mole, which then enabled me to make an accurate visual size comparison.
To add even more accuracy, I drew a spot next to the first drawing that was a little smaller, and one on the other side that was a little bigger.
I’d compare the mole to the middle drawing and it was a spot-on duplication of the size and shape (1 millimeter). After a few days, I noticed that the mole was a hair bigger than the original drawing!
I then lined the mole up with the larger rendition, and they matched in size! This was objective proof that the mole had increased in size!
So, not only had this previously solid brown spot taken on a reddish tinge, it had increased in size.
I had it removed and biopsied. Diagnosis: lentigo simplex (translation: irritated sun spot). The dermatologist’s nurse told me that it had probably been inadvertently rubbed or scratched, even maybe in my sleep.
What a Doctor Says About Moles
“A mole which is reactive to scratching or irritation, and does not have the cardinal signs of melanoma is still considered a benign lesion,” says Dr. Joshua Fox (not my dermatologist), founder and director of New York and New Jersey-based Advanced Dermatology P.C.
“It is benign and not dangerous in any way, even if it were to have some characteristics of the appearance of melanoma.
“It may require symptomatic treatment and observation; however, it will not be treated as melanoma.”
Mole mapping should include, when possible, drawings of your moles, for optimizing melanoma screening.

In 1987 Dr. Fox founded the AAD Melanoma and Skin Cancer Prevention Program in Queens, NY. He has been chief of dermatology of several major teaching hospitals including Mt. Sinai Hospital of Queens.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Small, Tiny Moles Turn Into Melanoma?

Can melanoma come from small, tiny moles?
Do you believe a mole can never turn into melanoma as long as it’s small or tiny?
If, during your monthly skin exams for cancer, you’ve decided to skip past your small, tiny little “birth marks” – you’re making a big mistake.
Historically, the rules for self-screening for melanoma have been to pay attention to the ABCDs of mole inspection, in which the “D” stands for diameter.
And typically, the diameter to be suspicious of is anything larger than 4 millimeters, or “the size of a pencil eraser.”
That got me thinking, because what’s so magical about 4 or 5 millimeters such that any mole smaller would be resistant to turning into melanoma?
“When I was training in dermatology in the mid-1970s, the ‘rule’ was that if a mole was less than 4 mm in diameter (one-sixth of an inch), then it couldn’t be a melanoma already,” says Neal Schultz, MD, a dermatologist with a private practice in the NYC area, and founder of dermTV.com.
“We now know that moles as tiny as 1 mm (1/25th of an inch) can already be a melanoma.”
I saw two red melanomas on a 27-year-old man’s forearm that were about 1 millimeter or so.
However, they had not sprung from pre-existing spots or “birth marks.”
Can a pre-existing, normal mole, that is small … say, around 1 millimeter … ever transform into melanoma?
Dr. Schultz continues, “People often wonder whether melanoma arises from normal pre-existing moles, or whether they arise ‘de-novo,’ meaning just from a single melanocyte (pigment cell) in the skin, which then becomes cancerous and goes crazy.”
Between 2003 and 2007, 150 melanomas that Dr. Schultz had diagnosed were analyzed in the laboratory for a retrospective study.
It turned out that 23 percent of the cancers were shown to have originated within a precancerous spot – and this included 1 millimeter moles.
“But then you have to understand that when a melanoma is really advanced and far developed, even if it develops in an abnormal mole, it may have destroyed the original mole.
“So the 23 percent number is a minimum, but not a maximum, since some of the melanomas that I diagnosed may in fact have arisen in moles, which the melanoma completely destroyed, and therefore there is no way on knowing that in fact, it started in a mole.”
Pay close attention to your small birth marks, brown spots, freckles, sun spots, what-have-you.
Just because a pigmented lesion is very small doesn’t mean that the DNA in it is resistant to the mutational changes that lead to melanoma.
If a tiny little “birth mark” seems to be getting bigger or darker, have a dermatologist look at it.
Interestingly, whether or not small moles can ever turn into melanoma has not received any fine-tuned verdict by the medical community.
Dr. Schultz says that some physicians believe “melanomas never arise in preexisting benign moles, and other physicians such as myself believing that as many as 20-25 percent of melanomas arise in preexisting benign moles, which in my view is substantiated by studies such as the one I mentioned.”
Many patients have reported that they’d been aware of a mole for years, appearing stable, and then one day they noticed that the spot was changing – with the diagnosis ultimately being melanoma.
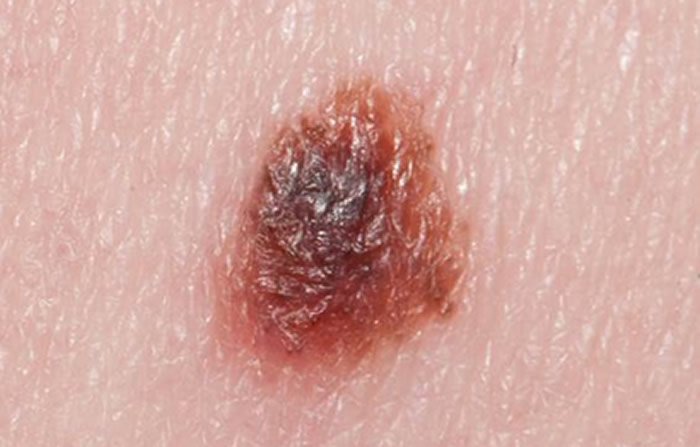
Melanoma under magnification. Shutterstock/Nasekomoe
So we know that melanoma, in the minority of cases, comes from pre-existing pigmented spots.
Many of these pre-existing lesions, in these cases, have always appeared normal, and were unchanging for years, present since childhood or birth.
Then the patient one day realizes that the spot’s been looking darker, or seems just a little larger.
- The big question, then, is what percentage of melanomas-from-pre-existing-moles comes from spots that were only 2 millimeters small originally?
- Only 1 millimeter?
- Only just a tiny speck?
This data has not been established. Nevertheless, by all means, during your monthly skin exams for anything suspicious or questionable, do not dismiss any tiny moles that you know have “always been there.”
This is especially true if you’re not sure that the little speck has always been there in the first place, which is why it’s a very smart idea to create a map of all your skin’s lesions.
This way, you can use it as a reference point every time you examine your skin for signs of melanoma.
 Dr. Schultz has been treating his patients’ dermatologic conditions for 30+ years, with particular emphasis in skin cancer prevention and treatment, acne treatment and laser surgery.
Dr. Schultz has been treating his patients’ dermatologic conditions for 30+ years, with particular emphasis in skin cancer prevention and treatment, acne treatment and laser surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}