

Why Don’t More Heart Surgeons Do Off-Pump Bypass?

Why don’t more heart surgeons perform off-pump (beating heart) surgery?
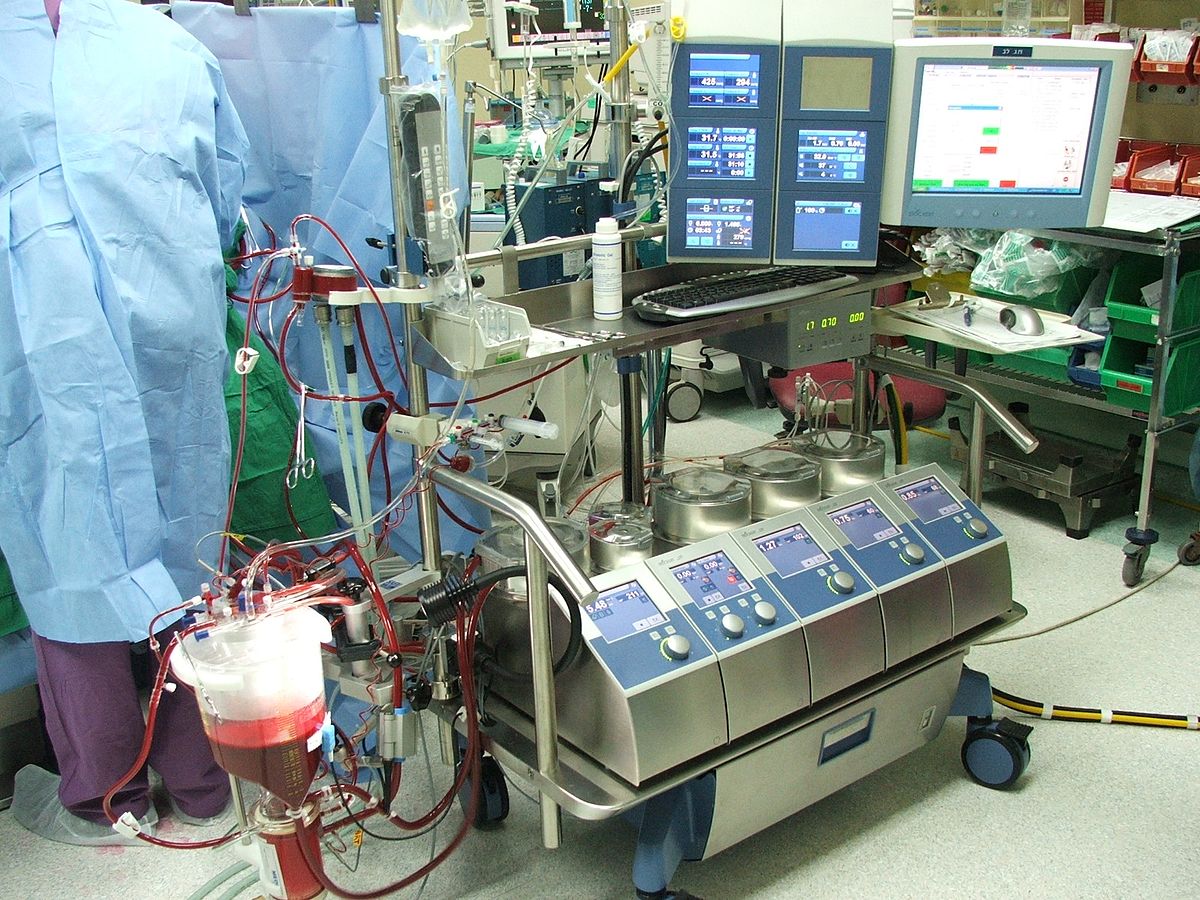
Off-pump heart surgery carries less risk of stroke and other serious issues when compared to on-pump heart surgery (i.e., operations that use the heart-lung, or cardiopulmonary bypass, machine).
I wondered why, in this day and age, off-pump surgery isn’t the standard for heart surgeons; why is it still the exception.
Coronary artery bypass grafting surgery is known as CABG.
“I have performed 80 percent of my CABGs off-pump for the past nine years with a dramatic reduction in blood utilization, stroke and renal failure,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
With beating heart surgery, post-operative depression occurs less frequently.
Dr. Fiocco continues, “The medical literature has a mixture of articles saying off-pump is better, off-pump is the same as on-pump, and even some that say off-pump is worse.
“Bottom line, in the hands of skilled and experienced off-pump surgeons, the results are better.”
Why don’t more cardiothoracic surgeons do beating heart procedures?
“The reason that only 25-30 percent of cases nationwide are performed with the heart beating is because it is technically more demanding,” explains Dr. Fiocco.
“It also requires very skilled assistants and dedicated anesthesiologists.
“Most surgeons do not have the patience to work their way through the learning curve to become skilled enough to approach the majority of cases off-pump.
“It is a challenging technique, but I feel very strongly that off-pump surgery will become even more important to learn as the population ages more and more.”
Who benefits most from this kind of surgery?
“Elderly patients see the greatest benefit from off-pump surgery, while a patient less than 60 probably benefits very little,” says Dr. Fiocco.
Can you elaborate?
“Age is only important as it relates to the disease state of the patient. Most younger patients tend to be healthier, less likely to have kidney, lung or vascular disease.
“Elderly patients are more likely to have renal insufficiency, COPD, history of stroke, calcification of the aorta, etc.
“These are the patients who see a marked risk reduction with off-pump CABG.
“That being said, there are some 80-year-olds who are healthy and I have no problem doing on-pump, and some 50-year-olds who are sickly and worrisome.
“But, in general, the younger are healthier and will tolerate either method.”
What kind of patients would probably do better with the heart-lung machine method?
“Off-pump surgery requires manipulation of the heart to visualize all areas,” says Dr. Fiocco.
“This is remarkably well-tolerated in most, but some patients develop a drop in blood pressure or EKG changes severe enough that they must be placed on-pump.
“Patients with a large heart, thick heart muscle due to high blood pressure, and cases that are true emergencies are usually the ones which can’t be performed off-pump.”

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ igorstevanovic

What if Coronary Bypass Patient Keeps Eating Junk Food?

How long do the grafts from coronary bypass surgery last if the patient continues eating a junk food diet?
Is coronary bypass surgery a green light to continue eating a junk food diet, and how long will the surgical bypass grafts last if the patient won’t quit his junk food diet?
About half a million coronary bypass surgeries (aka CABG) are performed in the U.S. every year, and you can believe that out of this gigantic number, a substantial amount of patients continue with their junk food diet after the surgery.
“Many factors determine how long CABG grafts will last,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
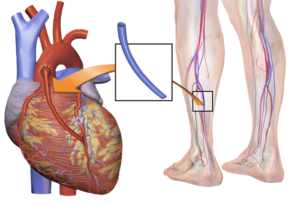
“The internal mammary artery graft (IMA) is superior to saphenous vein grafts (SVG), with a patency greater than 95 percent at five years and likely at 10 years.”
The saphenous vein comes from the leg. The patency for the SVG is 82 percent at five years, and 65 percent at 10 years, according to a small study. Dr. Fiocco says there are problems with these numbers.
“First, this is a sample of patients; not everyone returns to have their grafts looked at, which used to require cardiac catheterization, but now can be done with CT scan,” says Dr. Fiocco. The CT angiogram will reveal any dangerous narrowing of the arteries.
Dr. Fiocco continues, “Second, this sample includes those who lead a heart healthy lifestyle after surgery and those who didn’t, so the smokers and junk food eaters certainly bring these numbers down.
“Thirdly, a closed graft does not necessarily mean a failed surgery or the need for another operation.
“If you have CABG x 4 or 5, and one graft closes, chances are you are doing fine and won’t need any other intervention.”
There have been no extensive studies on just how damaging a junk food diet (or smoking) is on a revascularized heart.
But do we really need research to know that if a patient continues with a bad diet after coronary bypass surgery, he will shorten the life span of his bypass grafts?
The junky diet is what got him in trouble in the first place (along with any other heart-harmful variables such as smoking, lack of exercise and mismanagement of diabetes).
Dr. Fiocco explains, “Diet and exercise, along with smoking cessation, will improve the longevity of the grafts, but to put a number on it is difficult since the quality of the vein, quality of the artery being sewn to, and the technique are all important as well.
“I tell my patients that they will at least get 10-15 years out of bypass surgery if they follow a heart healthy lifestyle.”
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Coronary Bypass Surgery Cause Orthostatic Hypotension?

Can orthostatic hypotension be caused by coronary bypass surgery?
If you’re wondering if orthostatic hypotension can be caused by coronary bypass surgery, you’re not alone.
“Hypotension after surgery is a common problem and takes several different forms,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Orthostatic hypotension means the blood pressure drops when going from a sitting or lying position to a standing position. This may be accompanied by lightheadedness or dizziness.”
In some cases of orthostatic hypotension, the patient will start blacking out and even completely faint.
However, an all-out fainting episode can be arrested if the patient takes a seat.
The tricky thing is that sometimes, once a fainting spell begins unfolding, the patient will not be able to self-correct the situation, and thus will fall to the floor.
This can have devastating consequences if the head takes the brunt of the fall.
Dr. Fiocco continues, “The major causes are dehydration, over-medication (too much antihypertensive med) and a poorly understood third cause felt to be related to vascular tone and/or hormone levels (thyroid/cortisol).”
Immediately following coronary bypass surgery, a patient actually retains fluid, and is given diuretics to drain the fluid – unless the patient’s kidneys have been acutely damaged from the coronary bypass surgery (diuretics impose stress on the kidneys).
Longer-out from coronary bypass surgery, when there is no longer edema (fluid retention), and the kidneys have rebounded, the patient may still be experiencing orthostatic hypotension – from dehydration.
Lingering effects of the general anesthesia, and/or the heart-lung machine that was used during the coronary bypass surgery, could temporarily alter taste, making water consumption unpleasant.
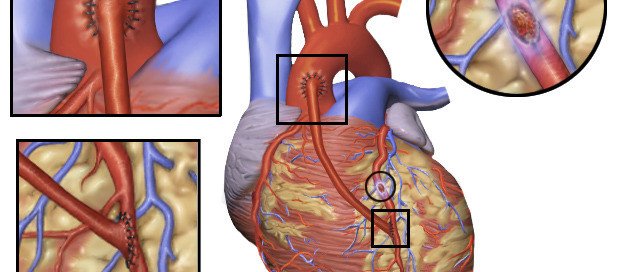
Coronary bypass surgery. Shutterstock/Medical Communications, Inc.
“Obviously, medication adjustments can be made by eliminating certain meds or decreasing the dose,” says Dr. Fiocco.
For instance, Lopressor (used to help heart rhythm after coronary bypass surgery) can cause low blood pressure or dizziness.
Amiodarone, another drug commonly given after coronary bypass surgery, can cause low blood pressure.
Dr. Fiocco says that adjusting medications solves the overwhelming majority of orthostatic hypotension cases.
“The vascular tone/decreased hormone patients tend to be hypotensive, whether sitting or standing.
“These patients may require an IV medication to support their blood pressure while in the hospital until the vascular tone returns and/or the hormones are replaced. This may prolong the hospital stay to as long as 5-6 days.”
So just what is vascular tone?
Dr. Fiocco explains, “Everyone has a certain degree of vascular tone. Medications to treat high blood pressure are designed to decrease vascular tone or relax the blood vessel wall which consists of, among other things, smooth muscle.
“Relax the muscle, the vessel dilates and blood pressure comes down. Why this occurs after surgery, particularly coronary bypass, is unclear.
“Likely it is multifactorial involving general anesthesia, pain medication, exposure to various drugs in the OR and maybe most important, preoperative medications.
“Rarely, it can be caused by hypothyroidism or hypoadrenalism (lack of steroid production by the adrenal glands).”
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Does the Heart-Lung Machine Affect Sense of Taste?

Does the heart lung machine (cardiopulmonary bypass) affect sense of taste?
The heart lung machine is used during cardiac surgery so that the surgeon can make repairs on a completely still heart (no pumping), but can the heart lung machine cause a change in taste perception of the patient?
Some controversy surrounds use of the heart lung machine (“on-pump” surgery), as it has been suspected as a cause of neurological problems in a small percentage of coronary bypass patients – problems that were non-existent before their operations.
It is not unheard of for a coronary bypass or other cardiac procedure patient, whose surgery included use of the heart lung machine, to post-op complain of taste problems.
“Change in taste is most commonly due to a disturbance in the sense of smell, known as the olfactory system,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital, one of the nation’s top 50 heart hospitals.
“The heart lung machine may play an indirect role in altering taste. Most commonly patients complain of a) metallic taste b) tastes bad and c) no taste.”
Food may taste like cardboard or be extremely bland, and water may have an unappealing taste.
Interestingly, certain foods may taste just fine post-op to the coronary bypass patient who reports a change in taste.
“The heart lung machine’s contribution to this is likely its propensity to cause edema or swelling,” continues Dr. Fiocco.
“This can occur throughout the entire body, including the brain, thus affecting the olfactory system (smell) which, as noted above, will alter the sense of taste.”
However, if you’ve recently had coronary bypass or other cardiac surgery, and were connected to a heart lung machine (cardiopulmonary bypass), and … if you’ve noticed a change in the way food or beverages taste … this alteration isn’t necessarily the result of the heart lung machine.
Dr. Fiocco explains, “Separate from the heart lung machine, but related to bypass surgery, is the change in taste associated with general anesthesia as well as the side affects of many medications.
“The majority of patients resolve their taste problems within a few weeks without treatment other than occasionally having to change or withdraw certain meds.”
In conclusion, if you have had coronary bypass surgery, and are having difficulty eating due to a change in taste, keep reminding yourself that the diminished or unpleasant taste sensation is temporary.
Also keep reminding yourself that following coronary bypass surgery, you need to eat like an athlete, because your body has been subjected to significant (though controlled) trauma, and is in desperate need of nutrients, particularly protein, for the healing process.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Emergency Quintuple Bypass Surgery: What to Expect
Here’s what goes on the day you’re told a family member needs emergency quintuple bypass surgery after an angiogram shows severe blockages in five major coronary arteries.
My mother was wheeled into the OR for quintuple bypass surgery two or so hours after she was told she needed the operation, and two hours after I was informed.
Imagine my shock when the worst-case scenario that I had played out in my mind had been the need for a balloon angioplasty or a stent or two.
Events Leading up to the Emergency Quintuple Bypass Surgery
My mother had chest pain two days after she had complained of shortness of breath. The first ER visit netted a “likely” diagnosis of gastroesophageal reflux disease.
The second ER visit two days later revealed an elevated troponin level, and as a result, the ER doctor (a different one this time) strongly recommended admission to the hospital.
The admission would hopefully expedite my mother’s original plans (which preceded the shortness of breath incident) to undergo a treadmill stress test.
Next day she had an echocardiogram (ultrasound of her heart). The cardiologist and internal medicine doctor said that the result was “abnormal,” and that the treadmill stress test would be unsafe.
Instead, the cardiologist recommended a catheter angiogram.
My mother refused and wanted to go home. “It would be unsafe to send you home,” said the internal medicine doctor. This doctor spent quite a bit of time convincing my mother to stay at the hospital.
My mother was mad that the catheter angiogram couldn’t be done that day, and that in order to get it, she’d have to stay another night at the hospital.
Furthermore, after reading about possible complications of a catheter angiogram, my mother refused to take the exam.
While my mother was reviewing the waiver, I was on the phone with my father, who was at home recovering from back surgery he’d had nine days prior.
He was reporting that both his legs were swollen. He told me to try to track down his surgeon to get advice, even though I insisted I drive him to the ER (he was restricted from driving) — the same ER that my mother had been in the day previous.
I tracked down the surgeon who then called my father and instructed him to go to the ER.
So I left my mother with the urging that she undergo the catheter angiogram — which by then we were told they could probably do it that day.
The 40 minute drive home took forever. Then it was back to the ER — another 40 minutes away, during which my cell phone rang: My mother reported that she was on the way to get the catheter angiogram.
Once my father was settled in the ER waiting to go to the ultrasound room, I went to the catheter angiogram floor to seek out my mother.
Shocking News
The internal medicine doctor was urgently walking down the hall and spotted me. “Oh, there you are; I’ve been looking for you and trying to call you.” (My cell phone didn’t receive well in the ER.) The doctor was not smiling. “It’s about your mother.”
I assumed there was a complication from the invasive procedure. The doctor said, “Your mother has significant disease. Her main arteries are almost completely blocked. She’s gonna need bypass surgery. Hold on…” the doctor put a hand on my arm and went off, answering a page, while my bug-eyes followed her.
Soon afterwards I met the cardiothoracic surgeon who’d be performing the operation; one by one he named the arteries that needed bypassing. I counted five by the time he was done.
He then said my mother needed a mitral valve replacement. He said a “massive” heart attack was imminent.
I asked, if my mother went home instead, could she possibly have a fatal heart attack within a week?
The surgeon, cardiologist and internal medicine doctor all in unison said “Yes” and nodded their heads.
Preparation for Emergency Quintuple Bypass Surgery
My mother was wheeled out of the catheter angiogram lab, very sedated, on a gurney that appeared to weigh 1,000 pounds.
She was taken to the surgery prep room, people bustling around her. My father had no idea what was going on, wherever he was at the moment.
Someone went down to get him. He was wheeled up to the prep room, having not been told that his wife could have a heart attack any moment and was being prepped for quintuple bypass surgery.
He was wheeled to my mother’s side and she mumbled, “I’m going to have bypass surgery.” His mouth fell open.
My mother completely recovered from the quintuple bypass surgery, which involved the heart-lung machine.
My father didn’t have a blood clot; the swelling in his legs was from inactivity.
Anyways, hope this account helps you understand what goes on the DAY someone is told they need emergency quintuple bypass surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus
How Common Is Depression after Heart Bypass Surgery?

Depression after heart bypass surgery isn’t just about feeling depressed over clogged arteries, but the depression can have other related causes.
How expected or common is depression after coronary bypass surgery?
The University of Pittsburgh School of Medicine study showed that coronary bypass patients who had depression after surgery, fared a lot better with a phone-based, nurse-led care team, than did people who did not receive this added care to their heart surgeon’s standard rehab care protocols.
Study findings appear in the Journal of the American Medical Association.
However, 20 to 25 percent of patients experienced depression following coronary bypass surgery, says this outdated study that was published in 2009.
How Truly Common Is Depression after Heart Bypass Surgery?
“Patients have reported depression and memory loss after heart surgery for many decades, and initially was thought to be a result of the unnatural state of being on the heart lung machine,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“The latest data shows that depression and memory loss after heart surgery are directly related to your preop mental state,” says Dr. Fiocco.
“In other words, these patients have undiagnosed memory loss or depression coming into the surgery, and it becomes amplified post-op.
“With today’s techniques and the approach that stresses to the patient that the surgery is performed for them to return to their normal life, new-onset depression is very rare.”
Possible Cause of New-Onset Depression After CABG
Depression following CABG has been shown to impede quality of life and increase the risk of re-hospitalization.
An apparently new-onset depression that develops after coronary bypass surgery may be explained by several factors:
- Patient’s family isn’t supportive; not giving the emotional or physical support that was expected.
- There was pre-existing depression, but it had gone under the radar. The surgery has only amplified it.
- Patient becomes “bummed out” due to what lies ahead: weeks of rehab, weakness, sore chest, having to take new medications, missing work and activities, etc.
There’s nothing about CABG itself that directly causes changes in the brain that lead to depression.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2009/11/091116192345.htm

What to Expect Hours after a Quintuple Bypass Surgery

Here’s what to expect hours after quintuple bypass surgery — and it’s not pretty.
Forget what you’ve seen on TV shows; expect the patient to look hideous.
My mother underwent emergent quintuple bypass surgery; we had only two hours to digest this shocking information; about two hours lapsed between the time I learned that a heart attack was imminent, and the time that she was wheeled into the OR.
I was told that the coronary bypass surgery would take about six and a half hours (she also had a mitral valve replacement).
My mother was wheeled into the operating room at 7 pm. At 10:30 pm, at home, I received a call that everything was going well so far, and that the first incision had actually been made at 8 pm.
At 3 am the surgeon called and said my mother had been sutured up 30 minutes prior and that there had been no complications. He said that we could stop by and see her at around 9:00 or 10 am.
What to Expect Hours After a Quintuple Bypass Surgery
We arrived about 12 noon, and the nurse told us that just a half hour prior, my mother had been extubated (breathing tube from the general anesthesia removed; she had only then begun coming out of the anesthesia).
Her face was slightly swollen, eyes closed, body immobile. Both arms and legs were swollen.
She was responsive to our presence in that she began moaning upon learning we were there but did not open her eyes.
She was able to squeeze our hands. At times her eyes opened just a bit, but were not focused.
The moans didn’t sound too good, and the nurse said they were moans to signal she was in pain.
Even though my mother had been closed at 2:30 am, and it was now noon, she had, essentially just come out of the general anesthesia and thus, appeared to be very drugged and out of it.
She spoke a few unintelligible words to the nurse, that the nurse understood; a request for more pain medication.
Above my mother was a monitor, and all around it was equipment with various tubes, and tubes went into her.
Thick tubes came out from under her legs, and pink liquid was draining through the tubes into a container.
This pink liquid was coming from her lungs. Another tube was draining urine into a urine bag.
At all times a nurse was sitting in the room at a computer monitoring my mother’s vitals.
As the day wore on, my mother’s connection to what was going on around her improved slightly.
So you can expect all of that or something very similar in the hours following a quintuple (or lower CABG) bypass surgery.
My mother was not able to carry on a conversation and was not able to hold her eyes open in a focused way.
She had absolutely no interest in eating, though she was taking ice chips, and drinking a little ice water through a straw.
She did not leave the bed once, even though the nurse did adjust the incline of the bed.
By evening, my mother was still out of it, but also acknowledged our presence.
How a patient responds, or their level of awareness, in the hours after quintuple bypass surgery will depend on their age.
Elderly people tend to “come out of it” more slowly and are far more likely to have delirium from the general anesthesia. (This is true for any type of major surgery.)
If your loved-one is scheduled for coronary bypass surgery, don’t expect much interaction or conversation the same day post-op; the patient (depending on age and comorbidities) will want to just sleep, or if awake, will much rather want to listen to you than interact.
Coronary bypass surgery is a major trauma to the body that requires a lot of procedures, anesthesia and other drugs, and thus, recovery from the anesthesia may take many hours, all throughout the day and evening.
• The patient’s temperature and blood pressure will be taken frequently and so will blood sugar.
• A respiratory therapist will come in at regular intervals
• The patient will be encouraged to do breathing exercises to open up the lungs; this is actually the standard for any surgery post-op, not just heart bypass surgery.
The ICU scene of post-op quintuple (or lower CABG) bypass surgery will look alarming, but remind yourself that the presence of fancy-looking equipment and an entanglement of tubes simply mean modern medicine at work.
And by the way, the hours following CABG will probably seem like minutes to the patient.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rocketclips, Inc.
Coronary Bypass Surgery: What Patient Looks Like Right After
After coronary bypass surgery, what exactly does the patient look like?
What should family members expect to see when they walk into the ICU where the patient just arrived after undergoing coronary bypass surgery?
There are many variables when it comes to coronary bypass surgery (aka CABG).
My mother underwent a seven-hour operation that included mitral valve replacement, and she had five coronary arteries bypassed.
But I don’t think the way my mother looked in the ICU the day that the CABG was completed would have differed had the operation lasted only four hours.
Expect to see the following in a patient the day post-op coronary bypass surgery, and don’t be alarmed:
Swollen Legs
Swollen Arms
Swollen Face
Of course the legs will be swollen; that’s usually where the graft-vein is taken from. This is trauma to the legs and will cause fluid buildup.
The entire body is severely traumatized during CABG, and this includes the kidneys, which when normal, prevent fluid buildup in the body. Damaged kidneys will result in body-wide fluid retention.
A few days after CABG, my mother’s weight had shot up to 172. Pre-operation it was around 142. Her face was puffy and a bit discolored. The legs and arms were yellowish.
“Tubes are everywhere.”
You’ve heard this saying when someone describes a hospital patient.
You’ll think this upon seeing your family member or friend fresh from coronary bypass surgery, and all the tubes will be there while they are in ICU.
Tubing will include one for urinary output (leading to a bag on the floor) and one or two that are draining fluid from the lungs (leading to another bag).
In an episode of “The Golden Girls,” Rose is visited in her hospital room the day she has a coronary triple bypass.
If you see enough of these kinds of scenes, you’ll be that much more shocked upon seeing what it really looks like after a person has had CABG.
The “Golden Girls” scene was fake on every level. There wasn’t even an IV hookup!
Patient May Be Unresponsive
My mother’s CABG ended at 2:30 am.
It was around 12 noon when she was extubated … that is, the breathing tube from the general anesthesia was removed from her throat.
Extubation does not occur until the patient is conscious enough to follow breathing commands by the nurse.
If this didn’t happen till nine and a half hours after the CABG, then don’t be surprised if your loved-one still seems under anesthesia by the time you visit.
We visited shortly after extubation and my mother was non-conversational, could barely keep her eyes half open for more than several moments, and what few words she could say were feeble and slurred.
I’m inclined to believe that nobody just talks, like Rose did, the day post-op coronary bypass surgery.
Lots of Machines
You’ll see a lot of technology in the patient’s room and will wonder what it’s all for.
The machines are programmed to make beeping sounds when readings get to a certain point (or when medication runs low), such as blood pressure too low, heart rate too fast or heart rate fluctuating.
I will never forget the sound of the beep that signaled that my mother’s heart was “popping into” atrial fibrillation. This kept happening.
It got to a point where if I heard this same kind of beeping coming from another room, I’d get unnerved.
But after a while the occurrence became routine, and I became more desensitized to the beeping.
In summary, what a patient looks like right after, and even two or three days after, coronary bypass surgery is not pretty.
Expect lots of swelling, “thunder thighs” on a woman who, pre-surgery, had trim thighs, and arms “twice their normal size.”
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/BruceBlaus

Is 90s Too Old for Coronary Bypass Surgery?

Coronary bypass surgery is actually becoming more and more common in very old people.
Thousands of people in their 90s have had heart bypass surgery, also known as CABG.
People over 90 Years of Age Having Coronary Bypass Surgery
The American Journal of Cardiology has a paper endorsing coronary bypass surgery in people 90 and older. And this paper was published in 2007.
So more than ever today, your 90-something parent, grandparent or spouse may be a good candidate for CABG.
Look What the Study Says
The subjects for the study were 4,224 Medicare patients in their 90s who underwent heart bypass surgery between 1993 and 1999.
The patients were followed up for five years after their CABG procedures.
Interestingly, the women in the study had better survival rates than did the men.
However, this may have been because the women, who comprised 50 percent of the CABG patients, were more likely to spend time rehabbing in a nursing home as a transition, than were the men.
Can Just ANY Person 90 or Over Get Heart Bypass Surgery?

“When I first began doing cardiac surgery, we looked at 80 year olds as too old for surgery,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Now we operate on them all the time. I have operated on several 90+ year olds — but they must be robust, active and without dementia.
“Physiological age is much more important than chronological age.”
Carefully selected people in their 90s can benefit quite a bit from heart bypass surgery.
Suppose someone is 92 but has well-functioning kidneys, normal blood pressure without medication, and the only thing wrong with their heart is that the main arteries are 99 percent blocked.
Now let’s suppose we have a 75 year old who also has 99 percent blockages.
But in addition, this person requires medication for blood pressure control — and has moderate chronic kidney failure secondary to chronic heart failure.
The 92 year old will make the much better candidate for CABG.
Emergency Bypass Surgery
Another point to consider is if the heart bypass surgery is determined necessary on an emergent basis, versus as a planned treatment option for severe coronary artery disease.
In the case of an emergent basis, the elderly patient may be told that a massive heart attack is imminent without the CABG procedure.
According to the American Heart Association and the American College of Cardiology, a patient should not be considered too old for coronary artery bypass surgery based strictly on age alone, because potential long-term benefits must be weighed against the risk of the procedure.
Thus, a person who’s 95 but in otherwise good health (e.g., no diabetes, nonsmoker, healthy body weight) may actually be a better candidate for heart bypass surgery than a 70-year-old smoker who’s obese and diabetic.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: sciencedaily.com/releases/2008/02/080202124039.htm

Survival Rates of Elderly Bypass Patients after Heart Attacks

An elderly person suffers a heart attack and undergoes coronary bypass surgery.
How long are they expected to survive on average?
Is the bypass surgery even worth it for a very elderly person?
Heart bypass surgery in the elderly following heart attacks is becoming more common, but there has been little research into the mortality rates for this population.
Coronary bypass surgery is also known as revascularization.
A study in the Canadian Medical Association Journal (2010) reports that coronary bypass surgery in the elderly after a heart attack can improve survival rates — but the study forecasts the improvement out to one year.
There isn’t a whole lot of data on the impact of coronary bypass surgery on the elderly who have suffered a heart attack.
The researchers in this particular study wanted to investigate the trends in the use of revascularization and medication prescriptions in the elderly, over a span of 10 years.
The research involved over 29,000 patients at least 80 years old.
This is one of just a few investigations into long-term mortality developments in the elderly who’ve had a heart attack.
First author of the study, Maude Pagé, explains, “We found that the rate of one-year mortality after a heart attack decreased from 48.4% in 1996 to 30% at the end of the study in 2006.”
It’s important to note that the data may be influenced by the fact that elderly patients have been arriving at hospitals sooner over the years.
Nevertheless, the data indeed reflects the increasing use of coronary bypass surgery for people who once were considered too old for revascularization.
Coronary bypass surgery is becoming more common in people even over the age of 90, with favorable outcomes.
“There is great physiologic variability in the older group and the published results of surgery in the elderly do not support prejudice based on age,” says Dr. Mark Katlic, of Geisinger Health System.
“There is no age in isolation that contraindicates surgery, although ageism exists. Many groups have shown that excellent results are attainable with compulsive attention to detail.”
Risk factors for heart disease, which can become severe enough to require coronary bypass surgery (revascularization) go well-beyond the highly publicized obesity, smoking, lack of exercise and emotional stress.
Here are additional risk factors for heart disease: poor sleep, which includes excessive sleep; excess belly fat, despite thin limbs; having a hostile or argumentative nature; poor oral hygiene; and having panic attacks (at least in postmenopausal women).
The need for coronary bypass surgery does not occur overnight. It takes years to develop.
Thus, it would seem that the need for revascularization could be prevented in many people if they began heart disease screening early on in their adult life, rather than waiting till they were elderly to get things taken care of.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}