

Does DVT Risk Increase with a Cast or Splint?

Wondering if your risk of deep vein thrombosis goes up if you must wear a cast or a splint?
“Any kind of immobility, which slows down the blood flow in the legs, will increase the risk of DVT,” says Dr. Paramjit “Romi” Chopra, MD, founder of the Midwest Institute for Minimally Invasive Therapies (MIMIT), an interventional radiology and endovascular therapy practice.
“When we walk, our calf muscles act as pumps to work against gravity and pump blood from the legs back to the heart,” explains Dr. Chopra.
The German Institute for Quality and Efficiency in Health Care (IQWiG) conducted a study on young athletes — who, by the way, are not immune from a deep vein thrombosis.
Young athletes with a cast or splint are at increased risk for deep vein thrombosis, especially if they’re sitting for extended periods on a bus or airplane traveling with their team.
After all, the cast or splint forces a considerable degree of immobilization, even if the cast only goes from the ankle to below the knee for a broken ankle.
The limited movement from the leg, due to the cast or splint, can also increase risk of deep vein thrombosis forming in the pelvis.
What Should You Do?
So if you end up with a cast or splint on your leg or a portion of your leg, what should you do, to minimize developing a deep vein thrombosis?
Get back on your feet and move around as soon as possible. Of course, this is easier said than done when you have an injury.
The next defense is medication: anticoagulant drugs, also known as blood thinners, which reduce clotting ability in the blood.
Blood thinners do not bust up the clot (that’s another class of drugs known as “clot busting” or thrombolytic drugs).
But they can prevent pre-existing clots from getting bigger, and of course, blood thinners go a long way in preventing the formation of new deep vein thromboses.
Ditch the Cigarettes + Other Preventive Measures
Another way to reduce the risk of deep vein thrombosis while you’re stuck in a cast or splint is to quit smoking if you’re a smoker.
Next, if you have high blood pressure, get it under control asap.
Ask your orthopedic or sports medicine physician to recommend some exercises you can do with the leg that has the cast or splint.
For instance, if only the lower part of your leg is in the contraption, you can do quite a bit of exercising with that leg.
- For example, get on all fours.
- Bring the knee of the affected leg towards your chest, then extend the entire leg out straight behind you.
- Bring the knee back in, and so on, for 10-20 repetitions. Switch legs.

Freepik, yanalya
Another exercise is to be on all fours but extend the leg out to the side.
If the entire leg is in a cast, lie on your back and lift the leg up and down (if your doctor clears you for this).
Or, while standing on your good leg, swing the casted leg from the hip, or make circles with it.
Do these exercises every so often to reduce the risk of deep vein thrombosis.
Dr. Chopra combines his Eastern roots and 30+ years’ Western experience to unify the best of both worlds at MIMIT to treat venous disease, peripheral artery disease and musculoskeletal disease.
combines his Eastern roots and 30+ years’ Western experience to unify the best of both worlds at MIMIT to treat venous disease, peripheral artery disease and musculoskeletal disease.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sources: sciencedaily.com/releases/2009/07/090723113523.htm; mayoclinic.com/health/deep-vein-thrombosis/DS01005/DSECTION=treatments-and-drugs
Do ALL Pulmonary Embolisms Come from a DVT?
The common-held belief among physicians is that pulmonary embolism is always from a DVT, a blood clot that forms in the legs or pelvis.
The DVT may break away and end up in a lung, causing the potential to kill a person.
The belief, then, has been that pulmonary embolism and deep vein thrombosis should coexist in the majority of patients, since, allegedly, only part of the blood clot in the leg breaks away, rather than the entire clot.
A report in Archives of Surgery says something very interesting.
The report concerns a study involving 247 trauma patients who had scans done of their lungs, legs and pelvis.
Forty-six of these patients had pulmonary embolus. And 18 percent had deep vein thrombosis.
However, seven of the patients had both pulmonary embolus and deep vein thrombosis.
Were there differences between patients with pulmonary embolus plus deep vein thrombosis, and patients with PE without deep vein thrombosis? No.
The study authors concluded that there is little evidence that pulmonary emboli always come from a DVT of the peripheral veins.
Cadaver studies have shown that usually, only part of the blood clot dislodges and travels elsewhere. The study authors further state that many pulmonary emboli indeed form in the lungs.
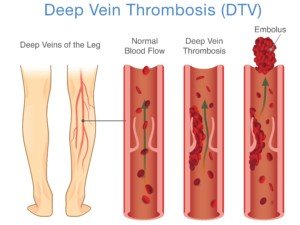
Where are all the places in the body a deep vein thrombosis may form?
“DVT is the general term, meaning a thrombus in any deep vein including the veins in the lungs,” says Steve Elias, MD, FACS, a vein specialist with Englewood Health in NJ.
Shutterstock/solar22
“DVT in the legs is the most likely source, but DVTs in unusual places such as the lung, ovarian veins, veins in the brain, etc., should make the doctor more suspicious for an underlying cause: cancer, clotting problems.”
Every year in the U.S., 100,000 to 180,000 people die from a pulmonary embolism.
Every year, 600,000 Americans are hospitalized for a pulmonary embolism!
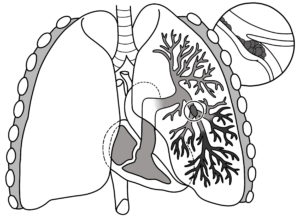
Pulmonary embolism
Symptoms include sharp pain in the chest, difficulty breathing, shortness of breath and coughing up blood.
 Dr. Elias is a leading name in venous disease, minimally invasive vein disease therapy and clinical vein and wound research. Dr. Elias lectures about all aspects of venous disease nationally and internationally.
Dr. Elias is a leading name in venous disease, minimally invasive vein disease therapy and clinical vein and wound research. Dr. Elias lectures about all aspects of venous disease nationally and internationally.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sources:
sciencedaily.com/releases/2009/10/091019172329.htm
sciencedaily.com/releases/2011/03/110305105233.htm

DVT from Air Travel: Truth or Hype?

Is deep vein thrombosis from air travel exaggerated?
DVT from long air travel times is not likely in healthy people, says the German Institute for Quality and Efficiency in Health Care (IQWiG).
The IQWiG reveals some intriguing findings, based on analysis of millions of air travelers.
For people on a flight longer than six to eight hours, only two to five, out of every 10,000 travelers, developed a deep vein thrombosis that resulted in symptoms.
What about flights under 4-6 hours? The researches uncovered no convincing evidence that flights under this time frame put people at increased risk for deep vein thrombosis.
Nevertheless, nobody knows if they’ll be that two to five out of 10,000, so to lower risk of deep vein thrombosis, the researchers say to wear compression stockings – but put them on at least two hours prior to your flight, and they should stay on during the whole flight.
What if You’re not so Healthy and Have Risk Factors for DVT?
Though there may be a little hype relative to healthy fit air travelers, it’s certainly not a case of overreaction for flyers with DVT risk factors:
- Smoking
- Obesity
- Old age
- Lack of exercise
- Sedentary lifestyle
- Recent joint replacement or abdominal surgery
- Pregnancy
- Family history of blood clots
“DVT is the occurrence of blood clots forming in the venous system, usually the lower extremities,” says Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths and Tricks: A Physician’s Advice.”
“Such clots are fairly common [while on the ground] and most often are produced by slowing the venous blood flow in these extremities, which can occur in a variety of situations such as sitting for prolonged periods, as can occur during a long air flight,” explains Dr. Tavel.
“Although clotting is unusual even under this circumstance, it can be avoided by frequent moving of the legs, flexing of the leg muscles and walking about.
“The main danger presented by these clots is their breaking away from the veins of origin to be carried by normal blood flow to the lungs, where they can suddenly block flow to portions of the lungs, a process called pulmonary embolus or PE.
“If the blocked artery is sufficiently large, it may cause serious damage and even death.”
Precautions Against DVT Are Easy
If you’re on a long airline flight, make a point of moving your legs periodically — whether you’re as fit as a fiddle or have health ailments.
Stretch your legs out if you can. If you’re cramped, then knock them together; go up and down on your toes; and lift your legs at the hip area (flex the hips).
But the best way to keep blood circulating efficiently, so that it doesn’t clump together and form a deep vein thrombosis, is to just get out of your set and walk up and down the airplane’s cabin.
Even if you don’t have symptoms of a DVT (cramp, pain, swelling, warmth or redness in a leg), you should get up at least every hour.
After all, about half of deep vein thromboses don’t cause symptoms.

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: sciencedaily.com/releases/2009/07/090723113523.htm
Which Is Better for CABG: Radial Artery or Saphenous Vein?

What’s better for coronary bypass surgery: a vein from your leg or an artery from your arm?
In coronary bypass surgery (aka CABG), the saphenous vein from the leg is typically used for the grafting procedure.
“Radial artery has been championed as a bypass conduit two or three times during my 20+ years of practice, and then falls out of favor due to graft closure or spasm,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“As the medications have improved to prevent spasm, again — the radial artery is making a small comeback,” continues Dr. Fiocco.
“This artery is only used as a graft to arteries with 90-100% narrowing; anything less and graft closure incidence increases.
“Comparing to saphenous veins is difficult due to variations in vein quality (is the vein dilated, are there varicosities, or is it pristine?).
“The radial artery can be an excellent conduit in the right circumstances, but overall is likely equivalent to a good quality saphenous vein.”
Coronary artery bypass grafting is the most common surgical procedure in the United States.
Study Pitting Radial Artery Against Saphenous Vein for CABG
A study shows that the radial artery from the forearm, wrist and hand, when compared with the saphenous vein, does not result in a better outcome as far as angiographic patency (open, unobstructed graft).
It has been believed that grafts from arteries are better conduits than grafts of the saphenous vein, because grafts from the left internal mammary artery have worked well for bypassing the heart’s left anterior descending artery.
It’s estimated that around six percent of CABG patients receive radial artery grafts.
For this study, over 700 patients were involved, who underwent elective coronary bypass surgery.
The one-year angiographic patency of the saphenous veins and radial artery grafts were compared in the patients.
The investigation was headed by Steven Goldman, MD, of the Southern Arizona VA Health Care System and the University of Arizona Sarver Heart Center.
For the left anterior descending artery, the left internal mammary artery was the graft of choice.
Remaining arteries that needed to be bypassed received either the radial arterial grafting or the saphenous vein graft.
At the post-CABG one-year mark, the angiographic patency was measured.
Was there any significant difference in the one-year graft patency between the saphenous group and the radial artery group? No.
There also wasn’t any difference, when comparing the two groups, regarding adverse events.
Here is what the study authors write: “Although most clinicians assume that compared with vein grafts, arterial grafts have an improved patency rate, there are little multi-institutional prospective data on radial artery graft vs. saphenous vein graft patency.”
If you have a coronary bypass surgery scheduled, do not hesitate to meet with your surgeon and ask questions.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: sciencedaily.com/releases/2011/01/110111165011.htm

Which Lowers Stroke Risk More: Off Pump or On Pump CABG?

Stroke is a real risk during and following coronary bypass surgery — which may be on or off pump.
There are actually four kinds of CABG, but which one has the lowest risk of stroke?
The four kinds of CABG are:
1) Off-pump, or “beating heart,”
2) On-pump with beating heart,
3) On-pump with a stopped heart,
4) On-pump with hypothermic circulatory arrest (the body is cooled; the heart is stopped; circulation is at a near standstill).
The risk of stroke is present in all four coronary bypass surgery strategies.
“There are many articles that show a decreased stroke risk with off pump CABG,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“This is thought to be due to less manipulation of the ascending aorta — no need for cross-clamp, cannulation, and no need for the unnatural state of being on the heart/lung machine,” explains Dr. Fiocco.
“Conversely, there is data that shows no difference in stroke rates between off and on pump.
“This may be due to patient selection, surgical technique and even the degree of postop anticoagulation.
“Our own data shows a decrease in stroke with off pump surgery to less than 1%. Oddly, it is not 0% with off pump.”
What about beating heart surgery plus the cardiopulmonary bypass (pump)?
A 2011 issue of the Journal of the American Medical Association reports on a study of over 45,000 patients who had CABG between 1982 and 2009.
On pump with a beating heart showed to have the lowest risk of stroke.
Over the past 30 years, says this study, the risk of stroke from CABG procedures has decreased.
The study that’s in JAMA reported that, of those 45,000-plus patients, 705 (1.6%) had a stroke.
Of these 705 patients, 58% had their stroke post-surgery, and 40 percent had their event during their coronary bypass.
The study identified stroke risk factors during and post-CABG as being:
Stroke history, older age, atrial fibrillation (abnormal heart rhythm) prior to the coronary bypass, and type of CABG: on-pump with the hypothermic circulatory arrest.
This is the type of CABG that my mother underwent, and, no pun intended, it was quite chilling to hear the doctor describe how he was going to perform this surgery (a quintuple bypass).
My mother did not have a stroke; the surgeon had informed me that the risk was “one to three percent.”
In the study, the on-pump with hypothermic circulatory arrest had a stroke rate of 5.3%.
The lowest rate (zero percent, actually) was for the on-pump with beating heart.
The second lowest rate (0.14%) was for off-pump. And for on-pump with stopped heart, it was 0.50 percent.
So why has the incidence of stroke decreased during the CABG or post-operatively?
The researchers attribute this to better preoperative assessment, improved anesthesia and surgical techniques, and post-surgical care.
The overall picture, however, is that stroke risk is lower with off pump CABG (beating heart) than with on pump (stopped heart).
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: sciencedaily.com/releases/2011/01/110125172309.htm

Is Same Day Angiogram, Bypass Surgery, Valve Replacement Safe?

Can angiogram, bypass surgery and valve replacement be done in the same day?
And if so, how life-threatening could this trio be?
Coronary angiogram, coronary bypass surgery with heart valve replacement, all in the same day — it was done with my mother.
In the same day she had a coronary angiogram, coronary bypass surgery and mitral valve replacement.
The catheter angiogram is an invasive procedure that carries the following risks: cardiac arrest, blood clot, arterial damage and infection.
The angiogram is the gold standard for detecting blockages in coronary arteries as a result of heart disease.
If the blockages are extensive enough, a surgeon will deem the situation an emergency and want to operate as soon as possible.
Otherwise, delaying the coronary bypass surgery by even a few days can put the patient at risk if a heart attack is imminent.
“Your mother is stabilized,” I was told by the internal medicine doctor after I learned she needed quintuple bypass surgery.
She had undergone an angiogram and the worst I had expected was the need for a stent or balloon angioplasty.
Imagine my horror when the internal medicine doctor said, “She’s going to need bypass surgery.”
I was a bundle of nerves as I waited in the corridor after the doctor went back into a restricted area.
Soon, I was told that the surgery would be sometime next week; it was now Friday, and I was concerned that in the interim, she’d have a heart attack.
I didn’t feel too confident that the heparin drip and supplemental oxygen would be very preventive.
Neither did the cardiothoracic surgeon; next thing I knew, a doctor told me that the surgery would be “this evening.”
This spared me the anxiety of having to wait several days for it and fear that during that several days’ wait, a heart attack would come.
I was also informed that she had mitral valve regurgitation and would require a tissue valve replacement; the tissue would be from a pig.
I asked if there was any danger in performing the coronary bypass surgery so soon after the invasive angiogram, and I was told that there was no great danger there (I don’t recall the specific words, but the translation was: no great danger).
It’s not uncommon for someone to undergo coronary bypass surgery the same day as a catheter angiogram.
This is called emergent coronary bypass surgery; the image shows vessels so severely blocked, that the physician determines that a heart attack can happen at any time, and thus, decides to perform the operation as soon as possible.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ChaNaWiT

Does the Heart Lung Machine Cause Cognitive Impairment or Not?

The heart-lung machine used in coronary bypass surgery is a two-edged sword.
The cognitive problems that are associated with it have led to the name “pump-head” to describe some patients who — seemingly — are in a permanently worsened cognitive state since their coronary bypass surgery.
“Although there may be temporary cognitive impairment after open heart surgery, this resolves over several weeks,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“It is difficult to determine if this is only related to cardiopulmonary bypass, but more likely is due to multiple factors.
“Sleep deprivation, narcotic pain meds, change in environment, and the stress of this physical and emotional trauma all are likely contributors.”
What about alleged cases of permanent worsening of mental faculties that were noted only since the bypass operation?
Dr. Fiocco explains, “Long-term cognitive impairment is rare and almost always associated with preop subtle cognitive loss that has gone undiagnosed — and is brought to light by this stressful event.”
There simply has not been any way to determine just how many patients — with perfectly intact cognitive function prior to cardiopulmonary bypass — ended up permanently cognitively impaired after the procedure.
For all we know, there may be patients who experienced that temporary post-surgical cognitive impairment that Dr. Fiocco mentions — and it lasted perhaps around two months.
But in the course of the last month, by sheer coincidence, the patient began showing the first early signs of dementia — which would have occurred even without the heart surgery.
But due to the coinciding timeline, the dementia (or “cognitive impairment”) is blamed on the heart-lung machine.
In such a patient, just as the temporary effects of the surgery and all of its associated stressors are beginning to resolve, the first signs of dementia are kicking in, overlapping.
This scenario is entirely possible because so many CABG patients are over 65.
Many may die (of any cause) before a formal diagnosis of Alzheimer’s disease is made.
Absence of this diagnosis strengthens the argument that the heart-lung machine can cause permanent cognitive impairment.
Nevertheless, it’s a hardcore fact that for many patients, the post-op period includes mental impairment to some degree.
A Research Study
A research team set out to see if minimizing surgical trauma to the heart’s aorta during bypass surgery would cut down on the post-op cognitive problems.
The study results appear in the Journal of Thoracic and Cardiovascular Surgery (Jan. 21, 2006) and was conducted by Wake Forest University School of Medicine.
Beginning in 1992, the team from Wake Forest has been investigating the cognitive problems that proceed coronary bypass surgery when the heart-lung machine is used.
For the study, 237 patients were involved. Some patients had the coronary bypass surgery with the heart-lung machine plus standard manipulation of the aorta (cross-clamp), while others had the same operation except a single clamp was used.
The single clamp moves the aorta less than does the cross-clamp.
Surgery without the heart-lung machine was also in the comparison.
The patients received psychological tests before their operations, then 3-5 days after, then 3-6 weeks after, and then six months after.
The Results
One week after the operation, at least 60 percent of the subjects in all three groups (1: heart-lung machine with cross clamp; 2: heart-lung machine with single clamp; 3: no heart-lung machine and thus no aortic clamping) had neurological deficits.
After six months, group 1 had the highest percentage (57 percent) of remaining neurological deficits.
Group 2 and 3 had percentages of 30 percent and 32 percent, respectively.
Wake Forest’s researchers’ monitoring techniques track particles — emboli and gaseous bubbles — that make their way to the brain during standard coronary bypass procedures. The emboli are believed to be the cause of the deficits.
The people who did not have the heart-lung machine during their bypass had much fewer emboli than subjects who had the heart-lung machine plus the cross clamping.
Keep note that this is an older study, but even today, there is still speculation when it comes to the heart-lung machine.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: sciencedaily.com/releases/2006/01/060123165002.htm

Beating Heart vs. Heart Lung Machine in Bypass Surgery

If you need bypass surgery you might wonder about having it done without the heart lung machine and instead with the “beating heart” procedure.
The absence of the heart lung machine is called off-pump or beating-heart bypass surgery, and research has shown that it reduces the problems that are associated with the heart lung machine.
A 2007 Journal of Cardiac Surgery reports that off-pump procedures are a safer option than heart lung machine procedures and reduce complications.
Off-pump surgeries also reduce hospital stays and costs, cut the need for blood transfusions and have been shown to reduce respiratory dysfunction.
But does this mean that off-pump heart bypass has advantages over cardiopulmonary (heart lung machine) bypass?
“I once was performing 80% of my CABG case off pump, but have cut back to 10% because the data just doesn’t support it as beneficial,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“Logically, one would think that eliminating the heart lung machine and all that goes with it (large cannula in the aorta, clamping the aorta, etc.), the patient would have fewer complications, but that is not the case.
“It is now reserved for those who are sicker, e.g., COPD, kidney insufficiency, calcified aorta, etc.
“There is clearly a benefit in those patients, but the low risk patient doesn’t seem to benefit.
“Also, it is technically more demanding, so most surgeons shy away from it.”
Prepping for Cardiopulmonary Bypass
In order for the heart-lung machine to be used, certain things must be done to the patient’s body.
For example, the heart is bathed in high-potassium fluids that stop the beating.
Tubes from the heart lung machine are connected to the heart, and the blood is rerouted into this device.
The blood comes in contact with the membranes of a porous plastic (where it is believed the blood may pick up micro-particles that eventually end up in the patient’s brain, causing cognitive problems).
But the blood must be routed this way to be oxygenated. It’s also cooled to around 82 degrees before being pumped back into the patient’s body.
The patient’s body temperature is also dropped. It is believed that after surgery is completed, quickly rewarming the patient’s body poses higher risk of cognitive damage than does gradually rewarming it.
That all sounds like a tremendous amount of prep activity, but the overall picture is that on-pump heart surgery is less tedious to carry out than is off-pump.
The heart lung machine does increases risk of stroke two to four percent, and can induce kidney damage, plus heighten risk of post-op infections.
Though earlier studies have linked the heart lung machine to residual post-op cognitive issues, newer research shows that the greatest predictor of post-op cognitive issues is the patient’s pre-surgical mental state, says Dr. Fiocco.
Your Surgeon Has Probably Never Performed Off-Pump Heart Surgery. This Is Not a Shortcoming.
The beating heart technique was pioneered way back in 1965 by a Russian surgeon, but not received with open arms in the States.
However, in the mid-1990s, the off-pump procedure was revisited due to development of new tools that stabilize small areas of the heart, permitting the surgeon to create bypass grafts.
At around 1996, just one percent of cardiothoracic surgeons were trained in off-pump surgery.
As of around 2004, nine percent of coronary bypasses were done without the heart lung machine.
Though beating heart bypass surgery is still not the norm and not considered standard, it’s been performed on over 45,000 people worldwide as of 2001.
And as scary as the heart lung machine sounds, the big picture is that the vast majority of the hundreds of thousands of patients every year in the U.S. who undergo on-pump surgery have successful outcomes.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Pfree2014
Sources:
ucdmc.ucdavis.edu/news/beating_heart.html
noblood.org/news-hot-topics-such-hepatitis-c-sars-aids/1258-heart-bypass-surgery-method-assessed-beating-heart-results-more-failed-grafts.html
sciencedaily.com/releases/2007/01/070131155322.htm

Sleep Requirements Following Coronary Bypass Surgery (CABG)

How much sleep should you get during recovery from coronary bypass surgery?
A healthy amount of sleep is so very important following CABG: coronary artery bypass grafting surgery.
“Most patients have difficulty returning to their normal sleep patterns for several weeks after surgery,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“It is easy to fall asleep, but difficult to stay asleep for more than three or four hours in a row.
“This is caused by many factors, including post-op discomfort, anxiety, and an overall feeling of fatigue, causing napping during the day and therefore fewer consecutive hours of sleep at night.”
My mother had quintuple bypass surgery, and she slept a lot (in the hospital as well as at home) following the CABG procedure.
Of course, a ton of sleeping will occur in the first few days following coronary bypass surgery, partially due to lingering effects of general anesthesia, plus side effects of painkillers.
Once the patient is in the cardiac wing for continuing recovery from bypass surgery, a lot of sleeping may continue to occur, if for no other reason that there’s not much to do in a hospital room between brief periods of walking therapy and attention from medical staff, unless you have a steady flow of visitors.
Dr. Fiocco continues, regarding once the CABG patient is home: “Also, many patients find it easier to sleep in a reclining chair compared to the bed (easier to get in and out), which may also limit sleep at night.
“These sleep issues are almost always self-limiting and resolve in several weeks without intervention. Occasionally a sleeping pill is necessary but only for a limited time.”
Dr. Fiocco also points out: “The trauma of major surgery combined with the emotional aspects of cardiac surgery lead to significant fatigue, which likely begins with loss of sleep before the surgery due to the anxiety leading up to the operation.”
In my mother’s case, there was little time for pre-surgery anxiety because she had only two hours’ notice of the bypass surgery!
And upon being told she needed emergent bypass surgery, she was already sedated from the preceding catheter angiogram procedure.
Dr. Fiocco says that the uncomfortable hospital bed doesn’t exactly encourage quality sleep, nor do the “interruptions for vital signs and blood draws, and sleeping in a strange environment.”
The CABG patient may be quite exhausted while in the hospital, but unable to sleep for significant chunks of time due to the various distractions (medical procedures, visits, even noisy floor cleaning machines in the corridor).
“Sleeping more than 10 hours/day may be a warning sign of depression, but it is more likely to be expressed in a lack of motivation to walk, read or get out of the house and begin normal activities,” says Dr. Fiocco.
The coronary bypass patient should listen to his or her body, follow cardiac rehab protocols (which will be supplied in booklet form) and keep in continuous contact with the post-surgery cardiac care team.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/gpointstudio
Can CABG (Heart Bypass Surgery) Disrupt Thyroid Function?

Can thyroid levels be affected by heart bypass surgery?
The thyroid controls metabolism. And metabolism is a lot more than how many calories per hour your body burns at rest.
“Metabolism is the process by which cells utilize oxygen for their performance in the human body,” says Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital, one of the nation’s top 50 heart hospitals.
Thus, it’s intuitive that coronary bypass surgery could somehow affect thyroid function in some patients.
“The simple answer is yes and likely in everyone, although only rarely is it of any clinical significance,” says Dr. Fiocco.
“Any patient in a stressful environment may have hypothyroidism based on laboratory measurements, but the majority resolve with the withdrawal of the stress (i.e., ICU, severe pain, cardiopulmonary bypass).”
Hypothyroidism means underactive, or low, thyroid: This gland isn’t producing sufficient amounts of the hormone thyroxine, which gives instructions to the body to carry out various functions.
Dr. Fiocco continues, “As far as the patient is concerned, they should be sure that their thyroid function is normal leading into the surgery, and then any small change due to the stress of surgery will not be a problem.”
A blood test that is given pre-surgery, as part of a workup to make sure that the patient can withstand the surgery, will reveal if thyroid levels are low.
Low thyroid is treated with a daily dose of bioidentical hormone replacement (to replace thyroxine).
When the dose is right, a blood test will show a TSH (thyroid stimulating hormone) numerical value that’s within a normal range.
A person with low thyroid may end up needing coronary bypass surgery (almost half a million CABG procedures are performed yearly in the U.S.), and pre-surgery, the patient’s TSH level may be normal.
However, post-surgery, even though the patient continues to take the oral dose of hormone replacement, the TSH level may not be normal; it may be off a little bit — enough to cause some symptoms that are typical of hypothyroidism.
“Yes, coronary bypass surgery can suppress the conversion of T4 to the active T3, making the thyroxine less effective,” says Kent Holtorf, MD, a thyroidologist and founder of Holtorf Medical Group.
T4 is another name for thyroxine, and T3 is triiodothyronine.
“The problem is that the TSH does not go up, but rather, down, so the tissue hypothyroidism is not detected by standard testing based on the TSH,” continues Dr. Holtorf.
“A TSH over 5 typically means that the thyroid is low, but with CABG, there are low thyroid levels with a normal TSH.”
“The significant physiologic stress associated with bypass will lower TSH production, which lowers T4, but more importantly, it reduces the T4 to T3 conversion inside the cell and increases reverse T3, which blocks the thyroid effect.
“Both these complications are extremely common and very treatable with supplemental T3, but it is rarely done because they are misdiagnosed as normal thyroid based on a normal TSH.”
So is a disruption in the so-called thyroid levels uncommon or common?
The best answer is to know the symptoms post-CABG that are suspicious for a thyroid issue.
Dr. Holtorf says, “The major symptoms of low thyroid levels post-CABG are heart failure and arrhythmias, such as atrial fibrillation, post-operatively.
If a patient has been pre-surgically receiving treatment for low thyroid, could coronary bypass surgery render their preexisting Synthroid or Levothyroxine insufficient?
Dr. Holtorf says, “Yes, it is especially a problem with those with preexisting thyroid dysfunction and on T4-only preparations.”
Symptoms of low thyroid include unexplained weight gain, feeling cold when nobody else does, unusual hair loss, fatigue and exercise intolerance.
However, hypothyroidism symptoms can also include: constipation, excessive sleepiness, elevated cholesterol, joint pain and stiffness, a puffy face, hoarse voice, muscle weakness, heavier than normal menstrual bleeding, depression, confusion, irrational thinking and memory problems.
If a person who, prior to coronary bypass surgery was normally upbeat and well-grounded, turns out to be uncharacteristically depressed, irrational and sluggish after surgery (taking into consideration the timeline for healing and emotional adjustment), the patient should have his or her TSH and T3 levels checked for possible low thyroid.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
 Dr. Holtorf has published a number of endocrine reviews on complex topics in peer-reviewed journals on controversial diseases and treatments.
Dr. Holtorf has published a number of endocrine reviews on complex topics in peer-reviewed journals on controversial diseases and treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}