

How to Get Relief from Fibromyalgia with Cymbalta
How does Cymbalta help relieve fibromyalgia pain?
You can get fibromyalgia relief with Cymbalta, a drug commonly prescribed for depression and also prescribed for panic attacks and anxiety.
You’ve probably seen the Cymbalta commercials, which begin with, “Where does depression hurt? Everywhere.”
Another of Cymbalta’s on-label uses is for the nerve pain of diabetes neuropathy.
There are a few ways in which Cymbalta relieves the pain of fibromyalgia, which is a pain disorder of the entire body.
Now, from an anecdotal standpoint, Cymbalta can bring on fibromyalgia relief by perhaps suppressing the patient’s perception of physical discomfort (which clinical depression will amplify).
This happened with my mother, but she didn’t have fibromyalgia; she had severe depression.
Coinciding with the depression were a few orthopedic issues, and while in a depressed state of mind, my mother complained that the orthopedic pain was excruciating.
Orthopedic discomfort indeed can be excruciating, but …. carpal tunnel syndrome?
Post-surgical discomfort from knee arthroscopy? (After my mother began taking Cymbalta, suddenly, the pain was no longer excruciating; it was merely inconvenient!)
Asking the Expert
How was it that an antidepressant like Cymbalta would end up with an on-label use for fibromyalgia relief?
“Pain management specialists prescribe Cymbalta for two reasons,” says Joe Wegmann, psychopharmacologist and licensed clinical social worker, author of Psychopharmacology: Straight Talk on Mental Health Medications.
“First, they are aware that that anyone with a chronic illness, especially a debilitating one like fibromyalgia, is at risk for depression.
“So physicians take this into account when treating fibromyalgia even if depression/anxiety is not present when treatment begins.
“Prolonged pain in anyone can cause changes in brain chemistry that can lead to depression.
“So physicians prescribe Cymbalta to cover for the depression that so often, at some point, develops in those with fibromyalgia.
“So brain chemistry does change as a result of this often debilitating physical illness.
“It’s impossible to separate the physical from the emotional; this is why depression rates are high in these patients.”
But even if a person with this disorder does not have depression, this SNRI antidepressant has been known to provide relief from the symptoms of discomfort associated with this condition.
Wegmann continues: “Another reason Cymbalta is prescribed for fibromyalgia is due to its powerful serotonin effects. Serotonin is a powerful vasoconstrictor, and since pain is linked to vascular vasodilation, Cymbalta’s constrictive effects help moderate pain.”
If your fibromyalgia is not responding to holistic treatments, and the pain is impossible to live with, your doctor may end up prescribing Cymbalta for pain relief.
 Joseph Wegmann is a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
Joseph Wegmann is a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

How to Get a Very Depressed Person Who Refuses to Eat to Eat

It’s really scary when severe depression prevents a person from wanting to eat; right before your eyes you see your loved-one wasting away from malnourishment.
Clinical depression can destroy appetite and cause a life-threatening issue of malnourishment, especially if the clinically depressed individual is elderly.
Not too long ago my mother developed a bout of clinical depression that is now under control with Cymbalta.
When my mother’s depression first began developing (it was a gradual process, not an overnight event), she commented that she “had no appetite.”
I didn’t take this seriously until I began noticing about two weeks later a visible loss of muscle.
My mother is of senior age, and it is dangerous for seniors, especially women, to lose muscle tissue.
It reached a point where I, and my father, had to prompt her to eat nearly every bite of food, and most of these prompts netted a refusal.
So how did I get my depressed mother to eat?
#1: Buy Walgreen’s “Balanced Nutritional Drink Plus.” Amazingly, I managed to get my mother to drink 1-2 cans a day. One can is 350 calories. Substitutes would be Ensure Plus or Boost Plus.

If you can get your depressed family member to consume two of these 8 ounce cans, that’s a good foundation of 700 calories for the day.
#2: When giving your depressed family member a beverage, include a straw. A straw guarantees more of the liquid will get consumed.
#3: Do not ask your depressed family member if they want something to eat or drink.
My father would ask this to my mother, and every single time, she’d say “No.” He’d then give up. BIG MISTAKE.
I decided to take the bull by the horns and instead of asking if my mother wanted to eat, I’d just bring the food to her mouth.
I strongly suggest that you don’t even TELL your depressed family member you’re going to give him or her some food or drink, because this will give them an opportunity to refuse.
Don’t inform them at all of your plan. JUST DO IT: Bring them the food.
When the food is in front of them, they are likely to take a bite or sip.
My mother has always enjoyed eggs. My father would ask her if she wanted eggs. She’d say no. He’d give up.
I insisted, “Don’t ask. Just make her the eggs. She’ll eat some once they’re cooked and in front of her.”
My father at first didn’t go along with this, but he eventually learned that it was true:
Once the eggs were actually prepared and placed before my mother, she’d eat some.
#4: Don’t be passive. Be kindly aggressive. Again, my father (along with my brother) one evening were enjoying salmon while my mother refused any food at all and sat withered in another room.
I gathered some salmon scraps and not only took a plate to her, but literally fork-fed her.
She consumed six forkfuls (about 15 grams of protein) that she would have never eaten had I not taken an assertive stand.
DO NOT BE AFRAID TO GET ASSERTIVE with your depressed family member who refuses to eat. It really works.
There were many instances in which I just verbally nagged my mother until she agreed to eat something, if for no other reason to get me off her back. Every bite counts. Every sip counts.
#5: When presenting your depressed family member with unexpected food (review #3), don’t just set it before them and walk away. Spoon feed them if that’s what it takes.
I spoon fed my mother pudding, chicken, and placed pretzels between her lips. I also placed cups to her mouth.
- Do not hesitate to make statements like, “If you don’t eat this, you may have to be tube-fed at a hospital.”
- I also told my mother, “I’m going to hover right over you until you drink this juice.”
These tactics worked, though often, my mother refused to finish the item. But hey, half a cup of juice is better than nothing.
Don’t assume that a depressed person who refuses to eat, absolutely will never eat while in bed.
I’d bring my mother quite a few nutrition cans with a bent straw, and while propped up, she drank the beverage.
She also ate eggs in bed while propped up; she didn’t ask for the eggs; I brought them to her and told her she was going to eat them.
#6: Don’t get concerned about nutrition; the issue is to just get calories into the depressed family member’s mouth, even if it’s junk food.
I was actually encouraging my mother to eat bacon and sausage — these have calories and protein.
BIG MISTAKE: Pointing out to a depressed family member who’s lost their appetite that something they’re suddenly interested in eating is not healthy.
#7: Do not make any comments within earshot of the depressed family member that might discourage eating.
Example: My father poured a can of soup into a pot. I removed another can from the cupboard: one for my mother, one for him.
He told me no, he was going to eat half the soup in the pot, while my mother would get the other half.
He said, “There is too much soup here for your mother to eat; I have to take half of it.”
This possibly gave my mother, in her depressed, vulnerable state of mind, the idea that she could eat only half the can.
She ended up eating half of what was in the pot because my father divided it into two bowls.
Had my father poured two cans in the pot, and then divided THAT into two bowls, my mother would have ultimately eaten more, even if she didn’t finish the bowl: 100 percent of half a can is LESS than 75 percent of one whole can.
#8: Sneak calories into the food. If I poured half a can of the Walgreens product into a paper cup, I’d then give her the remaining portion straight from the can and tell her it was “half full,” when in actuality, I had added a little milk to it.
#9: When your depressed family member, after eating at your insistence, says for the first time, “I’ve had enough,” or, “No more,” etc., this means they can actually take two or three more bites.
This was very predictable — but you’re the only one who has to know. Spoon/fork-feed those two or three more bites.
Thus, do not stop feeding your depressed family member after their first “Enough.”
The above tactics enabled me to get my mother to consume about 1,300 calories a day.
In order to get a depressed person, who refuses to eat, to consume this many calories, it’s essential to include, daily, two cans of the “Plus” Walgreens, Ensure or Boost products.
Secretly add a tablespoon of olive oil or chocolate syrup for even more calories.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Cymbalta for Pain and Depression: Helpful Information

Cymbalta is prescribed for depression and pain, and here is helpful information for people considering Cymbalta or who have already started taking this drug.
Cymbalta belongs to a class of medications called SNRI: serotonin and norepinephrine reuptake inhibitors.
When Cymbalta is prescribed strictly for pain (the patient does not have depression), what is the usual starting dose?
“Thirty mg a day for 3-6 weeks; if side effects are not a problem and pain persists, increase to 60 mg a day,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “From Fatigued to Fantastic!”
“Higher doses add significantly higher side effects but minimal improvement in pain relief over the 60 mg a day dose. Unlike most medications, Cymbalta tablets cannot be broken in half.”
I understand that getting off Cymbalta can be very troublesome.
Is this because many people quit cold turkey, or can it be difficult to get off it (withdrawal symptoms, discontinuation syndrome) even if it’s tapered (gradually decreasing dose)?
Dr. Teitelbaum: “Like all serotonin antidepressants (Prozac family), this is the case, and it can take months to taper off the medication.”
Is it true that a person’s body would necessarily build up a tolerance to Cymbalta, such that over time, the prescribed dose loses effectiveness, and then the patient must take a higher prescription? How common is this?
Dr. Teitelbaum: “Not very common.”
How would Cymbalta, at least a starting dose anyways, affect someone who does not have nerve pain, depression or anxiety? Would an SNRI produce exaggerated side effects?
Dr. Teitelbaum: “Likely make them hyper.”
It’s really fascinating how SNRI and SSRI (selective serotonin reuptake inhibitor) drugs work for depression, so here’s a basic chemistry lesson.
First of all, feeling depression is part of being human and having a higher-functioning brain. Depression can be caused by life events; side effects from medications; and for unknown reasons.
Depression can be mild, moderate or severe. For some depressions, there is an association between the level of serotonin in the brain and the presence of this mood disorder. The association is a reduced amount of serotonin.
However, researchers do not know whether this is cause or effect; i.e., does depression result in diminished serotonin, or does diminished serotonin cause depression?
And if the latter is the case, can stressful life events trigger this disruption of serotonin levels?
In the brain are neurons (nerve cells) that have receptor sites for neurotransmitters like serotonin.
After the receptor sites receive serotonin, a chemical process “destroys” the serotonin at that point.
This process is called reuptake. If too much reuptake occurs, low levels of serotonin result — which is associated with depression.
Drugs like Cymbalta inhibit, or put some brakes, on this reuptake process. The result is a higher level of serotonin, and in many cases, a complete vanishing of depression symptoms.
Cymbalta and other SNRIs, and SSRIs, don’t come without side effects. So before taking Cymbalta, do a risk-benefit assessment, and also keep in mind that if Cymbalta doesn’t work for your body chemistry, there are other similar drugs on the market.
And no matter what you decide, remember, a program of rigorous exercise and sound nutrition will go a long way to fight depression.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Phovoir

Kefir Is Great for Microscopic Colitis Relief!

Mmmm, a glass of chilled kefir just may relieve your microscopic colitis symptoms!
Give this probiotic a try; it will help re-balance the bacteria in your gut.
An imbalance may be causing or contributing to your microscopic colitis.
“Kefir or probiotic supplements can help to control the diarrhea in microscopic colitis,” says Lawrence Hoberman, MD, a board certified gastroenterologist and creator of EndoMune probiotic products.
“It is thought that there is a change in the healthy intestinal bacteria or microbiome which allows overgrowth of harmful bacteria, viruses or parasites.
“Taking kefir or probiotics that contain the healthy intestinal bacteria will rebalance the intestinal bacteria.
“This will modify the intestinal immune system and stop inflammation.”
Kefir Comes in Different Flavors

When I had a flare of microscopic colitis, kefir seemed to have a beneficial effect.
I won’t go the route of prescription or over-the-counter drugs because these only address the symptoms, if they even work at all.
In fact, Imodium may delay the inevitable by causing constipation.
Kefir works by actually treating microscopic colitis.
Essentially, kefir is yogurt in drinkable form, but it also contains live culture bacteria, or, the “good” bacteria, the beneficial bacteria that you need for optimum intestinal health.
Kefir is a probiotic; probiotics are good or “friendly” bacteria that are an integral part of a healthy balance of microorganisms in human intestines.
It’s believed by doctors that microscopic colitis can be caused by an overgrowth of bad bacteria; or, to put it another way, an imbalance in the ratio of good to bad bacteria in the intestinal tract.
There may be a genetic component to this, but that has not been proven.
Here are a few theories:
1) The body for some unknown reason “attacks” the good bacteria that grow in the colon, thereby offsetting the balance.
2) This can be triggered by NSAID’s and aspirin, antibiotics and eating certain foods that favor the growth of bad bacteria.
Because kefir is a probiotic, ingesting this drink helps restore a more optimal balance of good bacteria and bad in the gastrointestinal tract.
Years ago when my microscopic flare was in full force, I had gone off kefir several times, and every time, the symptoms returned.
My symptoms were a lot of diarrhea and large amounts of undigested food in my stools.
If you have microscopic colitis, go straight to the kefir, because it’s drinkable, which makes it more convenient than yogurt (which also comes in probiotic form).
You may also want to take probiotics in supplement form such as EndoMune if you don’t care for the taste of kefir or for times that you’ve run out of it.
 With 40+ years’ experience, Dr. Hoberman is an expert in probiotics. He has extensive first-hand experience treating a variety of digestive health issues and has seen the dramatic results probiotics have had on his patients. endomune.com/meet-dr-hoberman
With 40+ years’ experience, Dr. Hoberman is an expert in probiotics. He has extensive first-hand experience treating a variety of digestive health issues and has seen the dramatic results probiotics have had on his patients. endomune.com/meet-dr-hoberman
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/marina kuchenbecker

Natural Treatment for Microscopic Colitis: Kefir!

Let’s hear it for kefir as a natural treatment for microscopic colitis: This stuff works!
Microscopic colitis has no known cure, and treatments include natural and pharmaceutical.
However, treatment for microscopic colitis is hit or miss, and often nothing works to alleviate symptoms.
If you want to go the natural route with microscopic colitis treatment, I urge you to try kefir.
“Kefir is a fermented dairy product with high concentration of probiotics and special yeast which has been known for hundreds of years for its health benefits,” says Natasha Fuksina, MD, an internal medicine and obesity specialist who combines traditional, integrative and functional medicine to restore health and function.
“It contains multiple species of Lactobacillus, Lactococcus, Bifidobacterium and yeast.”
Perhaps you’ve already tried probiotics in pill form to naturally treat your microscopic colitis.
And they probably had no effect whatsoever. Don’t let this fool you!
I have microscopic colitis — have had a few major bouts — and they did not respond at all to probiotics in pill form.
However…every time I drank Kefir for more than a few days, the symptoms just about cleared up. This beverage is yogurt in drinkable form.
It’s thick like a milkshake and comes in different flavors.
However, I’ve been drinking only the plain.
Flavored varieties contain more sugars, and for all we know, this can interfere with the treatment process.
First try the plain kefir. Drink two cups (about 16 ounces) a day. No more.
No less, though I have not yet experimented with how effective less might be.
When on Kefir, I hardly had any diarrhea, and my stools looked closer to normal.
They were not as “dispersable” and contained noticeably less undigested food matter.
Thanks to this probiotic drink, my stool color was often normal and so was the caliber, shape and solidity.
It’s good to know that when I eat almonds, most aren’t passing right through me.
When I stopped drinking kefir, the symptoms of microscopic colitis returned: in my case, diarrhea nearly daily, at times twice a day, and lots of undigested food in my stools.
I’d go back on the probiotic drink, and these symptoms practically disappeared.
The reason I’d been on and off kefir is because, among a few other reasons, I wanted to prepare for a food sensitivity test, and wanted the microscopic colitis to be more in progress so that the stool sample could reflect it for the analysis.
Thus, I went off it for a week — and also because I had thought the microscopic colitis had spontaneously resolved.
What I didn’t realize was that the kefir had seemingly subdued it. Not long after quitting the beverage, the symptoms returned.
Within several days of resuming kefir, the symptoms again subsided. This cycle has happened several times now, and it can’t be coincidence.
“When consuming kefir on a regular basis, you introduce numerous colonies of healthy bacteria which can affect your microbiome in numerous ways,” says Dr. Fuksina.
“These newly introduced bacteria can fight harmful bacteria which develop during a colitis attack.
“They can help the good microbiota to proliferate and grow further.
“Furthermore, the bacteria contained in kefir and its byproduct, kefiran, can help modulate immune function and diminish inflammation.”
Remember, microscopic colitis is an inflammatory bowel disease.
“One daily kefir drink per day may be sufficient to help control mild cases of colitis, along with other nutritional strategies to keep the gut microbiome healthy and tame the inflammation.”
In conclusion, start drinking kefir today as part of your natural treatment for microscopic colitis, which, I might add, cannot be diagnosed with certainty unless you’ve had a colonoscopy — and tissue samples from your large colon are taken for analysis via microscope.
 Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
Dr. Fuksina is the founder of astraMDhealth, which includes telemedicine. Double board certified in internal and obesity medicine, she focuses on a personalized approach, including metabolism and genetic makeup, to customize treatments and preventive care.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Sea Wave

Denying Spouse Has Depression; When Partner Won’t Seek Help

How I convinced my father that my mother’s depression would not go away on its own.
Is one of your parents depressed, and the other parent in denial, and thus, a hindrance to treatment?
My mother was vehemently against taking an antidepressant, and wouldn’t state why, even though she was very amenable to taking prescription-strength narcotic painkillers, as well as Valium.
But for some mysterious reason, she refused to listen to why she should take an antidepressant.
Even though her clinical depression was draining my father, he, too, was very opposed to having his wife on an antidepressant.
I planned on staying with my parents for about three days, following my mother’s minor knee surgery, to help her recover. This was when I realized that she had developed clinical depression.
After six weeks of living with my parents to care for my mother who was crippled by depression, I convinced my father to speak to my mother’s doctor about prescribing an antidepressant.
The day I convinced him that an antidepressant was the only option left, was the culmination of six weeks of intense perseverance on my part.
Here are some objections (in bold) that the spouse, who’s in denial of a partner’s depression, might cook up, and after each objection, is what you, the daughter, son or other family member, can counter with.
I heard that antidepressants take two weeks to start kicking in.
“This depression will last a lot longer than two weeks without antidepressants.
“Before you know it, two weeks will have gone by, and she’ll still be disabled by depression, and then you’ll wish you had started her on an antidepressant two weeks ago.
“You don’t want to be kicking yourself for letting two weeks go by and she’s still suffering with depression.
“You don’t want to be thinking, ‘If she began antidepressants two weeks ago, where would we be now? Dang, I wish I got her on antidepressants two weeks ago.’
“There is no golden rule that it takes two weeks or four weeks for antidepressants to start working. That’s just a bell curve. For some people, the effect can be immediate, especially in severe depression.”
(In my mother’s case, the Cymbalta produced dramatic results the NEXT DAY).
She (or he) will never agree to see a psychiatrist.
“You don’t need to see a psychiatrist to get a prescription to an antidepressant. Any medical doctor can prescribe any drug. Her general physician can prescribe an antidepressant.”
She’ll never agree to go see even her general doctor for an antidepressant.
“Call the doctor’s office up, identify yourself, and ask if he could prescribe an antidepressant. He might do it over the phone without requiring a visit.”
(The phone call worked for my father, but this is no guarantee it will work for most people; we may have lucked out, because prior to this, my parents had been in his office and my father had inquired about an antidepressant, to which the doctor disagreed — details following).
Her doctor said she doesn’t need an antidepressant.
“Does her doctor LIVE with us to see what’s going on?”
My father accompanied my mother on a visit to her general physician for carpal tunnel syndrome, and at one point he asked about an antidepressant. The doctor said an antidepressant wasn’t necessary.
Ironically, my mother became hysterical after the doctor told her that he couldn’t line up an appointment with a hand surgeon sooner than one week away, and she cried her way out of his office.
After arriving home, my father told me that the doctor didn’t think she needed an antidepressant. When I objected, my father got angry. So repeat: “Does the doctor live here to see what’s going on?!”
Even if I get the antidepressants, she’ll refuse to take them.
“Not necessarily. Take things one step at a time. Cross that bridge when you get to it.”
Examine your unique circumstances. In my mother’s case, we could have easily given her Cymbalta without her knowing it was an antidepressant, calling it an “anxiety pill” instead (which Cymbalta is also prescribed for anyways), because my mother never goes online and thus would never Google Cymbalta.
If I tell her it’s an antidepressant, she’ll refuse to take it, and if I lie, she’ll look it up on the Internet anyways and find out.
“Tell her it’s an antidepressant and tell her you think it’s the right thing to do; when she sees you support antidepressant treatment, she’ll likely follow suit.”
This is exactly what happened with my mother; the moment my father relaxed his opposition to antidepressants, my mother instantly deferred to his judgment.
Crying spells are a symptom of depression, and my mother had plenty, but my father insisted: She keeps crying because of all the pain she’s in (carpal tunnel syndrome).
She must REALLY be feeling excruciating pain to be crying like that. The pain is what’s depressing her.
“Have you noticed that most of the time when she cries, she’s NOT reporting any physical pain?”
(My mother’s carpal tunnel syndrome pain triggered multitudes of sobbing episodes, but more sobbing episodes were during pain-free periods).
Point out to the spouse all the non-pain-related reasons that the depressed person has been weeping; reasons that should not make an emotionally well person break down.
Point out that when pain is severe enough, it’s impossible to cry: “A person will groan, moan, curse or holler, or even pass out, from truly excruciating pain. Who weeps upon stubbing a toe?”
“Think of the worst pain you’ve ever had; did you weep and weep? Maybe you screamed, but you didn’t sob.
Weeping is not a normal response to physical pain; it’s a response to EMOTIONAL pain, which can be brought on by moderate or even mild pain in a severely depressed individual.”
Point out that the crying sounds like she just learned her best friend died in a fire (which was exactly how my mother’s crying sounded).
She’s always been this way with pain. Point out how untrue this statement is, by citing examples. I cited examples of how my mother had responded in the past to physical pain (absolutely no crying or even teary eyes).
Never be afraid to use the word “depressed” repeatedly when referring to the patient.
Don’t give up. Keep harping on the fact that clinical depression will not disappear on its own; that nobody snaps out of this kind of depression; that you cannot talk a person out of FEELING the despair and darkness of major depression; and that, for Pete’s sake, since when is it normal to completely shut down, entire body and appetite and social connections and all, over carpal tunnel syndrome (or whatever relatively minor circumstance applies to your loved-one)?
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

IBS Relief from Bloating, Stomach Pain with Antibiotic Drug

Wouldn’t it be great if your IBS stomach cramping and pain and bloating could be relieved with a simple antibiotic drug?
IBS relief that lasts is here with an FDA approved drug, thanks to Cedars-Sinai Medical Center.
In this study, IBS patients reported continued relief of irritable bowel syndrome symptoms after going off the drug, called rifaximin.
This is a minimally absorbed antibiotic; it remains in the gut.
The trade name for the drug is Xifaxan.
“The study out of Cedar-Sinai was one of the studies that led to the approval of Xifaxan for IBS-D (diarrhea predominant IBS),” says Alan Gingold, DO, a board certified gastroenterologist with Central Jersey Ambulatory Surgical Center.
Dr. Gingold continues, “The study showed that a course of Xifaxan not only helped with the IBS symptoms of diarrhea but also helped with the abdominal pain and bloating that accompanies IBS.
“These symptom improvements seemed to be sustained beyond the time that the patient was on antibiotics and seemed to last for weeks to months beyond the course of antibiotics.
This also brought up the idea that there is an association between IBS and small intestinal bacterial overgrowth (SIBO) — and treatment of the SIBO improves the IBS.”
Consistency of stools also stayed improved in the study subjects.
The effect of Xifaxan supports the idea that gut bacteria trigger the symptom group known as irritable bowel syndrome, a chronic condition that affects 30 million U.S. people.
For some sufferers if IBS, treatment isn’t very effective. Treatment options include fiber supplements and changes in diet.
Xifaxan offers hope for these patients, especially since its benefits keep working weeks after the antibiotic is stopped.
Irritable bowel syndrome is typically diagnosed after all other possible causes of the symptoms have been excluded.
The symptoms of colon cancer are strikingly similar to those of IBS.
This is why you must have a colonoscopy if you’re experiencing any of the following symptoms:
• Unexplained Diarrhea
• Constipation
• Abdominal Cramping or Pain
• Abdominal Distension
• Bloating
• Excessive Gas
• Change In Stool Caliber
• Blood In The Stools
• Weight Loss
• Fatigue
• Diarrhea that Alternates with Constipation
 Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasha2109
Source: Cedars-Sinai Medical Center (2011, January 5). Antibiotic treatment effective in treating irritable bowel syndrome. ScienceDaily. Retrieved January 5, 2011, from http://www.sciencedaily.com /releases/2011/01/110105194836.htm

Can You Be Too Old to Get IBS (Irritable Bowel Syndrome)?

Are you thinking, “I can’t possibly have IBS because I’m too old!”? Then think again. You can be as old as the hills and still develop irritable bowel syndrome.
*****
An individual being too old for IBS?
“No! We need to first better understand IBS in order to see why different people develop this disease at different ages,” says Pejman Katiraei, DO, FAAP, an integrative physician whose many areas of specialty include adult and pediatric IBS.
Let’s examine the gut’s foundation. Some people are genetically predisposed to intestinal problems more than are other people.
This is why two people may eat the same bacteria-contaminated food, but only one gets sick.
“Was it the bacteria or the person?” says Dr. Katiraei. “To me, it was the person’s weak intestines that couldn’t handle the bacteria that was the problem, not the bacteria itself.
“By looking at things in this way and treating the problem underneath everything, we can help increase the resiliency of people and keep them healthy.
“There are ways to overcome genetic weaknesses. Having a gene does not mean you have to have the disease.”
Regarding IBS, there are individuals who have weaknesses in their intestines, whether it is a lack of digestive enzymes or a hyperactive immune response.
For some people, this may lead to subtle food reactions. This manifests in infants as colic or reflux.
“As these children grow up, they then develop ‘allergies’ with a chronic runny nose –- these children (and adults) are not having a reaction to the environment, but rather, they are reacting to the foods they are eating.”
With these kids are often recurring ear infections, which means recurring antibiotic ingestion. The human gut has “good” and “bad” bacteria.
Antibiotics kill the bad bacteria, but they also destroy the good, beneficial bacteria in the intestines. This weakens the intestines, perpetuating the vicious cycle.
“Next thing you know, the child ‘suddenly’ has IBS. It wasn’t ‘sudden!’ We just couldn’t recognize all the complaints that started in infancy.
“If that child was taken off dairy and/or gluten earlier in life, chances are they would have never developed IBS.”
Things play out differently with adults, continues Dr. Katiraei. Emotional stress kicks up the gut’s immune system.
In those with a hyperactive immune system, chronic stress results in an immune response that does not know how to shut itself off, as it would in a person who is blessed with a genetic predisposition to a resilient gut.
“As such, the immune system starts irritating the inside of the intestines, and this irritation ultimately shows up as IBS,” says Dr. Katiraei.
IBS does not have one cookie-cutter cause, which is why you cannot be too old to develop this condition.
An example would be a 50-something who’s always been healthy and takes a trip out of the country.
They suffer some temporary digestive upset from some bad food they ate in the other country and then forget about it.
Years later, says Dr. Katiraei, they “‘suddenly’ develop IBS after a seemingly minor flu or other illness. While this person may not have any genetic vulnerabilities, the parasite that they caught while on travel caused subtle but perpetual inflammation or irritation in their intestines.
“Then, any minor insult on top of the irritation causes the intestines to stop functioning well, which then results in an IBS picture.
“I have seen countless cases where once a person gets treated for a parasite, fungus, or odd bacteria, all of the sudden their IBS symptoms get better. IBS can show up at any age. It just depends what is causing the IBS to show up.”
Now that you know you can’t be too old to develop irritable bowel syndrome, realize that the older you get, the more likely that your IBS-like symptoms may actually be colon cancer!
In other words, don’t assume you have IBS and think it can’t be colon cancer because after all these years you’ve always been healthy.
Risk of colon cancer goes up with age, spiking after age 50.
If you have unexplained diarrhea, constipation, bloating, abdominal pain, weight loss or fatigue exceeding a few weeks, see a gastroenterologist to rule out colon cancer.
The diagnosis of IBS is made after a complete series of tests rule out other causes of your GI symptoms.

Dr. Katiraei created Wholistic Kids and Families for people interested in learning how to raise a healthy child (and future adult) in a world that’s becoming increasingly polluted with toxins (chemical and emotional).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sudden Headache While Lifting Weights: Causes and Solutions
A dangerous bleeding in the brain can be the cause of a sudden and severe headache that comes on during weightlifting.
Now let’s suppose you’re a longtime enthusiast of building muscle.
You’ve been pumping serious iron for years and have always felt fine.
Then one day in the gym as you strain for that last repetition in the squat rack – BOOM!
A sudden, really bad clap of a headache. Out of nowhere.
After you rack the barbell the headache is still there and lasts the rest of your time at the gym.
“Sudden onset of headache with intense exercise needs to be investigated,” explains Dr. Brian Loftus, a board certified neurologist in Bellaire, Texas, who specializes in migraine headaches and multiple sclerosis.
“The first job of the physician investigating is to rule out an intracranial bleed,” continues Dr. Loftus.
“If the patient is seen at the time of the headache – this can usually be done with a CT scan of the brain along with a lumbar puncture.
“If the patient is not seen near the time of the acute headache, then it is harder to rule out a bleed.”
If during a weightlifting set the athlete experiences a sudden bleeding in the brain, the cause would be a tear in a blood vessel.
But this cerebral blood vessel would have to have a pre-existing weakness in its inner wall.
This weakness causes the vessel to bulge or become dilated (aneurysm) – and all the while, maybe years, the athlete does not know this.
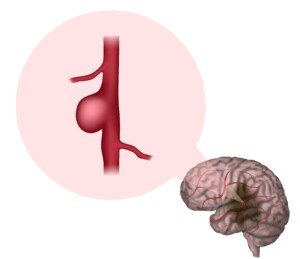
Brain aneurysm. Shutterstock/Veronika Zakharova
Until that moment while straining during a weightlifting set: the blood vessel tears. This is an aneurysm rupture.
Rising Blood Pressure when Lifting Weights
When you lift hard and heavy, blood pressure will significantly rise. This puts pressure on the inner walls of blood vessels.
That’s okay, too, as long as these inner walls are sturdy and tough.
But an aneurysmal wall may simply give way one day. A brain hemorrhage results.
It’s important that you realize that bodybuilding, powerlifting, etc., do not actually CAUSE an aneurysm.
But if you have a pre-existing aneurysm … intense straining with weight workouts is a risk factor for a tear.
As far as the overall possibilities of causes of a really bad headache in the middle of a weight workout, Dr. Loftus says that “It is relatively uncommon to find a bleed.”
A dilated cerebral blood vessel is a rare occurrence, especially in younger adults.
Risk factors are smoking and hypertension – which don’t go hand-in-hand with health conscious people who take their muscle building seriously.
Sudden Bad Headache While Strength Training
Now if you don’t smoke, have normal blood pressure and are a younger adult – and one day you get hit with head pain at the gym – you should still see a doctor.
If the pain goes away, it’s not a torn aneurysm. It’s likely an exertional headache.
These are harmless, though they can be painful enough to stop the workout.
They can last briefly to a few days and are often throbbing.
The throbbing nature does not mean it’s any more serious than if it were not throbbing.
Recommendations for “Weightlifter’s Headache”
Dr. Loftus endorses a medication called indomethacin for these exertional headaches.
A headache that comes on gradually, slow in onset, is not an exertional type.
The cause may be dehydration, especially while working out in a hot environment.
Stressed neck and trap-area muscles can also be a cause.
To help avoid any kind of headache while lifting weights, be well-hydrated prior to the routine, and keep hydrated throughout.
Stretch your neck and shoulder area before you begin working heavy.
Dr. Loftus has a private practice in Bellaire, TX, and focuses on headaches, multiple sclerosis and hyperhidrosis (excessive sweating). He is also board certified in headache medicine.
has a private practice in Bellaire, TX, and focuses on headaches, multiple sclerosis and hyperhidrosis (excessive sweating). He is also board certified in headache medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick.
Source: ihs-classification.org/en/02_klassifikation/02_teil1/04.03.00_other.html
Bad Pain in Back of Head from Squats: Causes Include Serious

Barbell Squat vs. Leg Press vs. Hack Squat Pros & Cons of All 3 Weightlifting Equipment

Barbell squats, leg press and the hack squat are favorite weightlifting routines among fitness enthusiasts and bodybuilders.
So as a former certified personal trainer, I decided to pit the barbell squat, leg press and hack squat against each other. Is one the best of the three?
Are they more or less equal?
Is one absolutely inferior to the others?
All three pieces of equipment – barbell squat, leg press and hack squat – can be a regular part of a leg routine, whether it’s strength training or bodybuilding.
But this does not mean that hack squats, barbell squats and leg press should always be in the same weight lifting routine.
I say always leave one on the backburner, to use when it’s time to re-shock your body into adaptation.
Choose two of the three for your weight lifting sessions. Also realize that barbell squat could mean free barbells or Smith machines.
Sometimes the free barbell squat is done with smaller lifting bars (the kind you can curl).
The hack squat this article refers to is the machine, not the free barbell version.
The leg press here is the floor equipment, which I consider more effective than the upright leg press, though the upright version has its virtues.
The best two out of the three are the leg press and barbell squat – though there are hardcore hack machine users who swear that the hack machine is the best.
Advantage of Leg Press
This apparatus pretty much leaves the lower back out of the picture; whereas in barbell squats, the lower back is stressed significantly.

Shutterstock/Free around
Because the legs are more isolated in the leg press, and your upper body is supported by the machine, you can work with much more weight than you could with barbell squats.
(People who can perform ultra-heavy barbell squats, can often do complete leg presses with up to seven, 45-pound plates on each side.)
There is far less risk for injury during leg presses, since your entire upper body is stabilized against the equipment’s back platform.
This enables you to do all sorts of interesting variations without worrying about slipping or injury: altering foot position and distance between legs, focusing on negative training, deep-knee training, etc.
Plus, if you can’t push the weights back up, you can always use your hands to push on your legs.
Disadvantage of Leg Press
Leg pressing really has no disadvantages. Just because leg pressing doesn’t work the entire body, like the squat, doesn’t mean it’s a flawed routine.

George Stepanek, CreativeCommons
The only “disadvantage” I can think of is that people with very stiff lower backs should avoid deep leg presses on declined leg press equipment until they gain some limberness in their lower back.
Advantage of Barbell Squat
Works many major muscle groups at once, including the core.
A strenuous set of 20 reps, in which the upward motion is more of a thrust, can drive heart rate up to 90 percent target heart rate — you can combine a short cardio interval with an intense resistance set. And 6-10-rep maxes have been known to build huge quads.

The barbell squat, whether done with a free barbell or Smith machine, strengthens the lower back, quads, glutes and even hamstrings. It improves body stability and balance.
Disadvantage of Barbell Squat
Requires tremendous attention to form. There is a relatively high risk of injury to the lower back and shoulders, especially if the barbell is free rather than the Smith machine. Some people never quite master good form.
A very deep knee bend can be stressful on knee joints for some people.
Because the lower back absorbs some of the weight, it’s hard for some individuals to reach a point where they can really challenge their leg power without their lower back giving out first.

Shutterstock/YanLev
Often, a 6-10-rep max is determined by the lower back maxing out long before the legs do.
If you have shoulder problems, barbell squats will be a hassle, since you must maintain a stretched, tensioned use of their shoulders to support the barbell.
In free barbell squats, it can be a drudgery to re-set a very heavy barbell back on its rack.
Advantage of the Hack Squat
Because these are so different from a leg press, they invite shock to the body and can accelerate results or bump you past a plateau. They target the quads more than the leg press.
Risk of low back strain is much less likely than in barbell squats, but it’s still present.

Shutterstock/mountaira
Disadvantage of the Hack Squat
These are just plain uncomfortable.
The position is unnatural, because you are tilted back while squatting. In real life, a squat is done vertically.
Also, most of these machines require you to slip your neck in between a narrow space, and shoulder pads fit on top of your shoulders; so your head and neck are very crammed in.
The problem is when your legs are so strong, you need a lot of weight, but then you can feel all that weight bearing down on your shoulders as you push up. Your shoulders may end up hurting more than your legs.
People with stiff lower backs may feel back discomfort at heavier weights.
On some hack machines, if you can’t get back up, you’re in deep trouble because your hands are not in a convenient position to lock in the platform.
Conclusions
If you absolutely abhor only one of these exercises, then it’s best to limit your involvement to several sets per month.
Otherwise, if you force yourself to perform the activity on a regular basis, you’ll likely output much less than 100 percent effort, when instead, you could be performing at 100 percent effort with a more desirable routine.
If you despise all three — barbell squat, hack squat and leg press — you’re on the wrong track.
You must make yourself look forward to at least two of them, so that every time you perform the routines, you can put passion into your efforts.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}