

Bad Cough in Elderly: When to Go to the ER

A bad cough in the elderly can mean pneumonia, a top killer of the elderly, so head to the emergency room promptly.
If an elderly family member (over age 65) has a cough that seems to be getting worse, take them to the emergency room, because this can mean pneumonia.
Pneumonia is the fifth leading cause of death in the elderly (over age 65).
“If there is fever, shortness of breath, and/or mental status changes, one should definitely visit the doctor’s office,” says Richard Honaker, MD, Chief Medical Advisor at Your Doctors Online, an online doctor chate site.
“If none of these are present, it is recommended to see a doctor if the cough lasts more than a week, is rapidly worsening, impacts sleep, is severe or is causing distress,” continues Dr. Honaker, who has 30+ years’ experience as a primary care physician.
My mother, whom I consider “young elderly,” developed a nagging cough that involved phlegm (a “productive” cough).
I didn’t think much of it since she felt fine otherwise, and has had coughs in the past.
“Because illnesses in older adults can be more serious and life threatening, I would suggest that they call their doctor who can then evaluate them and determine the appropriate next steps,” says Amber Robins, MD, a board certified family medicine physician in NY.
My mother called the Kaiser Permanente hotline to receive some advice from a nurse.
The nurse said that sometimes, it takes about three weeks for a cough (non-pneumonia) in the elderly to work its way out of the system.
That’s all the nurse said; just let it run its course. It seemed to run its course and apparently was out of my mother’s system.
A few weeks later I was visiting and noticed my mother was coughing quite a bit—the same type of cough, but very frequently and for lengthy episodes. She was hacking up phlegm.
I wondered if the previous bout had never really gone away, and instead whatever had caused it was still in her system, this time all fired up with a vengeance.
My father informed me that my mother had been coughing like this for the past three or four days.
Mistake
My father should have been more tuned into this problem and gotten my mother to the emergency room.
“Coughing in older adults can be due to several medical reasons that include both heart and lung disease,” says Dr. Robins.
Pneumonia, however, should always be considered even if the older individual does not have a chronic lung disease or a known heart problem. The earlier that pneumonia is treated, the higher the chance for recovery.
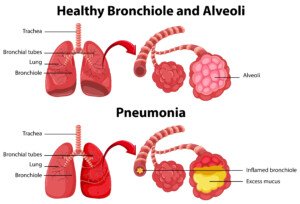
Freepik.com, brgfx
Instead, my father had believed that it was a mere resurgence of the cough of several weeks ago that the nurse hadn’t seemed too concerned about.
In fact, the nurse never even mentioned that it might be pneumonia!
Why didn’t the nurse say, “I can’t diagnose over the phone, but when an elderly person has a persistent or worsening cough, they should go to the ER to rule out pneumonia or a bronchial infection” ?
I couldn’t help but think about pneumonia, as the cough had a sinister sound to it. TRUST YOUR GUT.
I also had no reason to believe my elderly mother was immune to this infectious disease.
I said, “We have to get you to the ER. If this is pneumonia, it can be easily treated in the early stages.
“But if we don’t go to the emergency room, and this is pneumonia, it will progress beyond the point of no return.”
Well, that clinched it, and I took her to the ER, where the chest X ray confirmed “a little pneumonia.”
It was “a little” because I had gotten her to the ER early in the disease. Treatment was an antibiotic.
 Dr. Honaker has been recognized by D Magazine as one of the Best Doctors in Dallas several times and a Texas Super Doctor by Texas Weekly. He’s also a recipient of the Physician Recognition Award from the American Medical Association multiple times.
Dr. Honaker has been recognized by D Magazine as one of the Best Doctors in Dallas several times and a Texas Super Doctor by Texas Weekly. He’s also a recipient of the Physician Recognition Award from the American Medical Association multiple times.
 Dr. Robins has been active in various research studies that include gynecologic cancers, adolescent mothers and minorities in medicine.
Dr. Robins has been active in various research studies that include gynecologic cancers, adolescent mothers and minorities in medicine.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Ruslan Huzau
Sources:
seniorhealth.about.com/od/deathanddying/tp/cause_death.htm
mayoclinic.com/health/pneumonia/DS00135/DSECTION=symptoms

Pulmonary Embolism Tied to Excessive Sitting in Women

A pulmonary embolism is a blood clot in the lungs, and can be fatal within a minute, and for women who sit a lot on a daily basis, their risk is two to three times higher than in more active women.
This 2011 conclusion appears on the British Medical Journal website. An inactive lifestyle ups a woman’s risk of pulmonary embolism, plain and simple.
The conclusion was reached following an 18-year study of almost 70,000 female nurses who provided detailed information concerning their lifestyle.
In women who spent over 41 hours a week sitting, excluding at the workplace, the risk of pulmonary embolism turned out to be more than two times greater when compared to women who sat less than 10 hours a week, excluding at work.
Variables such as body mass index, age and smoking were adjusted for.
Not surprisingly, the investigation also revealed that a sedentary lifestyle correlated with high blood pressure and heart disease, and these conditions could quite possibly be driving forces behind pulmonary embolism.
There are a number of ways to reduce sitting time outside the workplace.
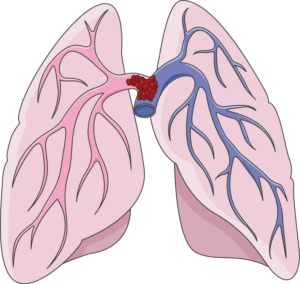
A “saddle” type pulmonary embolism, plugging up the area where the pulmonary artery splits off into each lung. This can cause death in minutes. Laboratoires Servier, CC BY-SA/creativecommons.org/Wikimedia Commons
If you’re concerned about pulmonary embolism, consider the following strategies for cutting back on the amount of time you spend sitting.
– Treadmill desk. A cheap model can serve as a desk for your computer at home, so that you can very slowly walk (sub-1 mph will do) while perusing the Internet.
– Set a timer for 45 minutes every time you sit before the computer. When it goes off, do something on your feet for several minutes.
– Stand while watching TV. This isn’t as dreadful as it sounds. You’ll get used to it. You need not stand still. You can march in place or tap your feet side to side, or pace frontward and backward for several steps.
– Pace while on the phone.
– Stand while going through the mail or eating a snack or even a bowl of cereal.
You should also be aware of how much time you sit at the gym, and I don’t mean during seated strength training exercises.
I mean in between sets.
Keep on your feet your entire workout, unless it’s time to lie down for a bench press or sit for an overhead dumbbell press or cable row.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik/8photo
Source: sciencedaily.com/releases/2011/07/110705071745.htm

Premarin vs. Estradiol and Blood Clot (DVT) Risk

Find out which poses a higher risk of a DVT blood clot: estradiol pills or Premarin pills.
To help manage menopausal symptoms, women can be prescribed estrogen-type pills, but these carry with them the increased risk of a deep vein thrombosis.
This is a type of blood clot that can dislodge and get into the lungs, fatally blocking air supply.
A new report in the JAMA Internal Medicine explains that in a study, women who took estradiol had fewer negative vascular events (such as a blood clot) when compared to those who took Premarin.
Premarin vs. Estradiol: DVT Study
The women in the study who did not develop a blood clot were also compared, in terms of their clotting factors.
The women on the Premarin, in this particular group, had increased clotting factors in their blood, than did women on the estradiol.
Plus, the Premarin users had a small increase in the risk of suffering a heart attack.
However, a difference in the risk of stroke was not observed.
Easing Menopausal Symptoms
So if you’re a woman who’s considering taking a pill to ease menopausal symptoms, you now have some information that should be helpful if you’re concerned about an increased risk of a blood clot, says the study’s first author, Nicholas L. Smith, PhD.
Symptoms of menopause include hot flashes, night sweats, vaginal dryness/burning/irritation, constipation and migraine headaches, says Mayoclinic.com.
The site also says that mood changes, sleep disturbances, thinning hair, dry skin, slowed metabolism and weight gain are also symptoms.
Many women prefer to manage menopausal symptoms with nutrition, supplementation and exercise, rather than take estradiol or Premarin.
But women who do take these hormone pills should know what the symptoms of a DVT are: swelling in one leg; redness and warmth in one leg; sudden cramping or pain that cannot be explained by recent exercise.

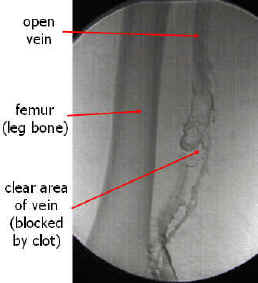
The leg on the right is affected by a DVT. Heilman, MD, CreativeCommons
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio
Sources:
sciencedaily.com/releases/2013/09/130930162226.htm
mayoclinic.com/health/menopause/DS00119/DSECTION=symptoms

Trouble Breathing, Chest Pain After Joint Replacement Surgery

Trouble breathing with chest pain after joint replacement surgery never has a benign cause, says Barbara Bergin, MD, an orthopedic surgeon.
NEVER assume that chest pain with difficulty breathing following joint replacement surgery is a sign of anxiety.
What can chest pain and feeling like you can’t get enough air actually mean?
“This would be a bad sign,” says Dr. Bergin, board certified orthopedic surgeon at and co-founder of Texas Orthopedics, Sports & Rehabilitation Associates.
“I can’t think of a benign process which would cause chest pain and trouble breathing after a total joint replacement, unless you coincidentally sustained an injury to your chest or ribs.
“Otherwise, you’re either experiencing a heart attack, or more likely…a pulmonary embolism, which is the result of a blood clot which has dislodged from the leg and entered the lungs.”
Father Had a Knee Revision Operation
I visited my father in his room three hours after his knee joint revision surgery.
On both feet were sequential compression devices that periodically inflate to squeeze against the patient’s feet to generate circulation in the legs to prevent blood clots.
He was also on the blood thinner Warfarin and was wearing knee high compression stockings.
Shortness of Breath and Chest Pain While Still in the Hospital
The hospital stay for a knee or hip replacement surgery is normally several days.
The patient himself, upon experiencing chest pain or diffiulty with breathing, may be able to press the nurse’s call button if alone.
The diagnosis of a pulmonary embolism, however, can only be made with a CT scan. There may be a few other tests as well.
Pulmonary Embolism
Only after this confirmation would the patient be givn a clot-busting drug via an I.V. — per doctor authorization.
Never would the patient receive such a drug without FIRST a diagnosis of a pulmonary embolus.
Naturally, I wondered what would happen if my father suddenly developed chest pain and shortness of breath, and on the way to the CT scanner, the pulmonary embolism got bigger and completely blocked his ability to breathe!
“A large blood clot to the lungs can kill you in short shrift,” says Dr. Bergin.
Why a Blood Clot Forms
“After surgery on the lower extremities, the blood coagulation process is in a heightened state,” says Dr. Bergin.
“This happens throughout the whole blood supply, in response to having a cut anywhere in the body.
“But in the leg, the circulation of venous blood gets sluggish because of the surgery and swelling.
“The movement of blood through the veins is assisted by movement of muscles.
“This helps pump venous blood out of the extremities, because veins have no ability to pump blood, like arteries do.
“What happens after surgery? We’re lying around in bed, not moving our leg, because it hurts [knee or hip replacement].
“So heightened coagulation + surgical swelling + less movement of the leg = increased potential to have a blood clot in the leg.
“This process usually takes a few days, but occasionally, it happens sooner. Some patients are more susceptible to developing blood clots, so it can happen within 24 hours.”
Trouble Breathing, Chest Pain Soon After Discharge
The patient continues to recover from joint replacement surgery at home. They then develop these two symptoms.
“This is an emergency, and under no circumstance should it be ignored,” says Dr. Bergin. “Call your surgeon, or better yet…call 9-1-1.”
Deadly Saddle
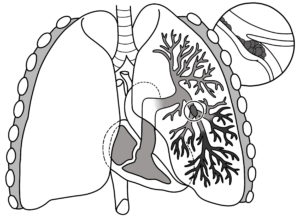
The type of pulmonary embolus that can kill in a minute is called “saddle,” because it blocks blood flow to both lungs at the same time — sealing off the entrance to any inhaled oxygen.
However, the saddle P.E. is not likely to strike a healthy person, even if they’re over 80.
It’s more likely with someone who has a pre-existing clotting disorder or very poor health.
The type of pulmonary embolus that usually develops in joint replacement patients are smaller clots that occupy only one lobe of the lungs (a pair of lungs has five lobes total).
A patient could have trouble breathing because a clot is in one lobe, but still be able to breathe with the four other lobes and have plenty of time for a CT scan and diagnosis.
Can shortness of breath + chest pain after a joint replacement have a less serious cause?
Dr. Bergin explains, “Occasionally chest pain and shortness of breath can be due to stomach acidity.
“But don’t assume that,” EVEN IF the patient has recently been diagnosed with a bad case of acid reflux.
“Chest pain and shortness of breath after surgery on the lower extremities means heart attack or pulmonary embolism until proven otherwise. You’re off to the ER in short order” if this occurs after the patient returns home.
As for my father, I was always on high alert, periodically asking him if he felt short of breath or had chest pain. He had no complications and fully recovered.

Dr. Bergin is a general orthopedist, surgically and conservatively treating all manner of bone and joint conditions. She enjoys educating patients so they can emerge stronger than they were before their orthopedic injury or surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ESB Professional
Sources:
mayoclinic.org/diseases-conditions/pulmonary-embolism/basics/symptoms/con-20022849
mayoclinic.com/health/pulmonary-embolism/DS00429/DSECTION=risk-factors

Knee Replacement DVT: Patients at Highest Risk?

Certain kinds of patients have the highest risk of a DVT following joint replacement surgery.
A DVT is a deep vein thrombosis which could break off and travel to the lungs and be life threatening.
When it comes to knee replacement surgery, few patients just do not have a choice, and along with this extremely common procedure is the risk of DVT: deep vein thrombosis.
DVT has gotten a lot of attention lately within the context of extended air travel, but the king of DVT production is surgery, especially joint replacement.
A deep vein thrombosis is a blood clot. Part or all of it may break away and migrate into the lungs: a pulmonary embolus.
Tiny pulmonary emboli are not life-threatening, but massive or “saddle” pulmonary emboli can drop you in seconds — permanently.
This is why DVT prevention is critical.
Anyone can develop a pulmonary embolus if the perfect storm is in place, such as extended air travel while keeping the legs in the same cramped position; lack of hydration; being on birth control pills; excessive bed rest from a foot injury; and so many other circumstances.
Joint replacement patients are given DVT prevention treatment, namely blood thinners.
But certain joint replacement patients still have a relatively high risk of deep vein thrombosis.
A report in the Journal of Bone and Joint Surgery (2011) states that blood clot formation, including the pulmonary embolism, is a serious complication from knee replacement surgery.
The paper also says: “Prophylactic measures, such as the use of blood thinners around the time of surgery, are used to reduce the occurrence of clots, but their effectiveness in routine clinical practice following surgery is more uncertain.”
How the Study Was Done
- The study tracked over 37,000 knee replacement patients between 1997 and 2007.
- For 90 days after surgery is when pulmonary embolism risk is highest.
- There were 441 patients (1.2 percent) who had to be hospitalized for blood clots during this time window. The following risk factors were associated with clot formation:
– Over age 80
– History of previous clot
– History of cardiovascular disease
– Increased comorbidities (additional medical conditions like diabetes)
The study noted that knee replacement surgery is generally a safe procedure, but that people need to be very DVT-aware.
During the surgical consultation, patients should discuss blood clots and not leave the consultation without knowing precisely what the prevention measures will be.
Some surgeons will prescribe blood thinners for only the hospitalization duration.
“Despite the use of blood thinners, patients undergoing knee arthroplasty continue to remain susceptible to clot formation for several weeks following surgery,” says the paper.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasirin pamai
Source: sciencedaily.com/releases/2011/07/110727121658.htm
Retrievable (Temporary) IVC Filters vs. Permanent: Pros & Cons
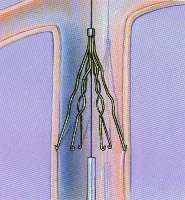
Wondering about the pros and cons of retrievable IVC filters vs. permanent ones?
Since you’re here you probably know what an IVC filter’s job is: prevent pulmonary embolism.
The largest study on following people with retrievable IVC filters supports the guidelines generated by the SIR: Society of Interventional Radiology.
An IVC filter can be placed temporarily or permanently.
IVC stands for inferior vena cava (a large vein involved in circulation).
A blood clot in a deep vein is called a deep vein thrombosis (DVT). If the clot breaks loose and travels to the lung, it becomes a pulmonary embolus, which can choke off a person’s oxygen supply in seconds.
Most people with DVT are treated with a blood thinner drug, which usually prevents pulmonary embolus.
An IVC filter will block a migrating DVT from getting into the lungs. Some people are not suitable candidates for blood thinners, such as trauma patients.
There’s also people who, despite being treated with blood thinners, develop DVT anyways.
In 2007, 167,000 IVC filters were placed. In 2012, at least a quarter of a million were placed.
Most of these filters were meant to be permanent. A type called “retrievable” can be later removed by a doctor.
However, some retrievable IVC filters can fracture or even migrate to other portions of the bloodstream.
The FDA has recommended that doctors who implant these devices routinely consider the risk/benefit ratio for every patient.
Removal should be considered for patients no longer at risk for PE.
Some Big Considerations
“In 2019, if a filter is deemed necessary, it probably should be a retrievable one, but plans need to be made for removal at the time of placement,” says Steve Elias, MD, FACS, a vein specialist with Englewood Health in NJ.
“The biggest problem with retrievable filters is that they are not retrieved,” continues Dr. Elias. “They work well. If one is 100% sure it never needs removal, then a permanent filter should be placed.”
A retrievable filter may need to be taken out within four to six weeks of placement. Waiting too long for removal would give the filter a chance to become too firmly attached to the inferior vena cava to be removable.
One of the reasons a retrievable filter may end up in the patient’s body too long is that the patient loses touch with their doctor during the crucial follow-up period.
Hence, selection of which patients should receive a retrievable IVC is very important.
Patients with retrievable IVCs or who are being considered for one should have very close communication with their doctor.
Those with the filters should talk to their interventional radiologist, plus other physicians, about any concerns.
 Dr. Elias is a leading name in venous disease, minimally invasive vein disease therapy and clinical vein and wound research. Dr. Elias lectures about all aspects of venous disease nationally and internationally.
Dr. Elias is a leading name in venous disease, minimally invasive vein disease therapy and clinical vein and wound research. Dr. Elias lectures about all aspects of venous disease nationally and internationally.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: sciencedaily.com/releases/2011/11/111128121545.htm

How Often Does Someone in the U.S. Die from a DVT ?

The rate at which a deep vein thrombosis kills an American will floor you.
Every year in the United States, a significant number of people die from VTE: venous thrombus embolism.
“DVT kills more people than accidents, cancer and AIDS combined,” says Steve Elias, MD, FACS, a vein specialist with Englewood Health in NJ.
“It is common all over the world — but perhaps not recognized as often in developing countries.”
How often does an American die from DVT?
Every five minutes, reports the Vascular Disease Foundation.
This translates to 100,000 to 180,000 Americans every year succumbing to deep vein thrombosis.
Though most VTE isn’t fatal, there’s no way to tell, in any given patient with a DVT, whether or not the clot will break off and travel to the lungs, how big the breakage will be and/or exactly where the broken fragment will lodge.
Keep in mind that many lives are saved because the symptoms of a deep vein thrombosis are difficult to ignore, prompting people to seek medical attention, leading to diagnosis and treatment.
Some estimates are higher, such as 300,000 Americans a year (Journal of Vascular and Interventional Radiology, Oct. 30, 2009).
The Vascular Disease Foundation says that just about anyone can develop a deep vein thrombosis under the right circumstances, and the more risk factors present, the more likely you’ll develop the condition.
The VDF names the following risk factors: smoking, obesity, sitting for more than six hours when traveling, prolonged bed rest, family history, cancer and cancer treatment, increasing age, recent major surgery (particularly orthopedic), and hospitalization for illness.
DVT symptoms may consist of pain, tenderness or aching in one or both legs; change in skin color (usually red or purple); skin hot to the touch; and swelling. Be especially suspicious if these symptoms occur in one leg.

Scientific Animations, Creative Commons/BY-SA/Attribution-ShareAlike 4.0 International
Dr. Elias is a leading name in venous disease, minimally invasive vein disease therapy and clinical vein and wound research. Dr. Elias lectures about all aspects of venous disease nationally and internationally.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Ocskay Bence
Sources:
sciencedaily.com/releases/2011/03/110305105233.htm
sciencedaily.com/releases/2009/10/091027132430.htm

Can a DVT Go Away on Its Own?

A deep vein thrombosis (DVT) can be deadly, but does this mean it can’t go away on its own?
If you suspect a DVT, get to the emergency room, because a deep vein thrombosis can travel to the lungs and cut off your air supply, killing you.
My mother was diagnosed with a “big DVT” in her jugular vein soon after coronary bypass surgery, but, believe it or not, it went away on its own.
Just when the DVT formed is not known; it may have formed during surgery or in ICU recovery.
It fattened her arm and I insisted on an ultrasound. However, nothing was done for this blood clot because the infusion of a clot-busting drug, said the doctor, would have put her at risk for lethal internal bleeding.
She was already on the blood thinner Coumadin as a regular post-bypass therapy, and thus, administration of a clot-busting drug was contraindicated.
So I asked the doctor, “What about this DVT in her neck? Can’t anything be done to break it up?”
He said that there was a “slim” chance that it would dislodge (travel to lungs).
I was told that her body would “reabsorb” the DVT, that it would “resolve on its own.”
How true is this?
“DVT, when it resolves, usually does “resolve’ on its own,” says Steve Elias, MD, FACS, a vein specialist with Englewood Health in NJ.
“Even when patients are using blood thinners for DVT treatment, the blood thinners’ role is to prevent further DVT from developing,” continues Dr. Elias.
“Blood thinners do not dissolve DVT. The patient’s own body’s enzymes do.
“So yes, in theory, a patient not on blood thinners can resolve their DVT.”
Sit and Wait
So over the next several days after her surgery, I knew that this big DVT was just sitting in my mother’s neck.
I knew that there was nothing to stop a piece of it, or the whole thing, from becoming renegade and getting into her lungs and becoming a pulmonary embolism.
I watched her arm like a hawk over the next several days to see if it was getting even bigger.
However, I noticed that the alarming swelling was gradually going down. Ultimately, the swelling disappeared.
At some point along the way a second ultrasound showed that the DVT had gone away.
Nevertheless, if you suspect a DVT, don’t think it will always “reabsorb” or “resolve on its own.”
Even if you’re young or an athlete. DVT means ER.
At the time of my mother’s deep vein thrombosis, I didn’t know about special filters that can be inserted in the patient’s vein to trap blood clots that have migrated from their origin and are heading towards the lungs.
However, filter insertion is usually for patients who cannot take Coumadin or other anticoagulant drugs, or when these drugs are not effective.
Dr. Elias is a leading name in venous disease, minimally invasive vein disease therapy and clinical vein and wound research. Dr. Elias lectures about all aspects of venous disease nationally and internationally.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus/CreativeCommons

DVT Prevention with a Treadmill Desk
A treadmill desk will go a very long way at helping prevent DVT: deep vein thrombosis.
Perhaps you’ve heard that prolonged sitting during air travel or road travel is a risk factor for developing a deep vein thrombosis (DVT).
Likewise, sitting for long periods in general can put a person at risk for a DVT, and this was first reported in the January 1954 New England Journal of Medicine.
And a report titled “eThrombosis” appears in the Feb. 2003 European Respiratory Journal, which describes venous thromboembolism that’s associated with immobility.
Unfortunately, the commercial invention of the treadmill desk didn’t occur until years later.
More and more office and home workers are using treadmill desks, the only way to eliminate all their excessive sitting.
The risk of DVT from excessive sitting is no secret, as more and more studies pile up pointing this out, such as the 2010 report in the Journal of the Royal Society of Medicine titled “Prolonged work and computer-related seated immobility and risk of venous thromboembolism.”
Venous thromboembolism is the term that incorporates both DVT and PE — pulmonary embolism — which can result when the blood clot partially or in whole dislodges and travels to the lungs, causing a potentially fatal outcome.
Long stretches of sitting does slow the blood flow in the legs; it doesn’t matter if you’re on an airplane, watching TV or at a computer.

Shutterstock/fizkes
A report in a 2007 Journal of Thrombosis and Haemostasis says that after 90 minutes of sitting (without intermittent relief exercise), blood flow to the vein behind the knee drops by 40 percent.
Treadmill Desk Solution to DVT from Prolonged Sitting
You needn’t walk fast on a treadmill desk to make it work against DVT development. Even a one-half-a-mile per hour walk will keep the blood flowing in your legs.
The Centers for Disease Control recommends that desk workers raise and lower their heels while keeping their toes on the floor, and repeating this but with the heels on the floor, and then tightening and releasing the leg muscles.
As a former personal trainer, I recommend simply exiting the chair and doing high knee marches, going up and down on the toes, leaning the hands on the desk and extending the legs, or walking about the room.
However, this requires keeping track of time, and for a busy desk worker, 90 minutes can fly by while they sit immobile without them realizing it.
A treadmill desk will solve this problem, keeping you in constant motion. I myself have a treadmill desk, and once you get absorbed in your work, you can easily forget that you’re walking.
Don’t take a chance; consider investing in a treadmill desk to help prevent DVT.
You need not spend ALL of your computer time walking at the desk.
You can move your laptop back and forth between a sit-down and a treadmill desk.
Or, a more convenient option is to get two computers: one that’s always at the treadmill desk and one that’s always at your sit-down station.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Source: patientblog.clotconnect.org/2012/10/22/behind-the-headlines-does-eating-lunch-at-your-desk-increase-blood-clot-risk/#more-1757

DVT Detection with Urine More Accurate than D-Dimer

A urine test may soon replace the D-dimer to screen for DVT (deep vein thrombosis) blood clots.
Imagine being in the ER with a suspected DVT (deep vein thrombosis), and instead of getting your blood drawn for the D-dimer test, you’re asked to give a urine sample because the nurse says, “We can see if you might have a blood clot by analyzing your urine.”
This scenario may soon be standard in ERs, thanks to a study led by Timothy Fernandes, MD.
The study report was published in 2014, but detecting a deep vein thrombosis with the patient’s urine is still not a standard procedure in emergency rooms.
But imagine the possibilities:
Detection of a DVT through urine would make it simple and easy to do in a regular medical clinic.
My mother has had her D-dimer level evaluated at least three times when she presented to the ER with symptoms that a DVT can cause.
Each time, the D-dimer was positive, and because of that, a CT scan of her chest was ordered to see if there was blood clot in her lungs (pulmonary embolism).
The CT scans were negative all those times. A positive D-dimer doesn’t always mean a blood clot. However, this tests helps guide physicians in what to do next.
“Physicians, especially in the emergency room, are often faced with patients with symptoms and risk factors concerning for DVT/PE,” says Dr. Paramjit (Romi) Chopra, MD, founder of the Midwest Institute for Minimally Invasive Therapies (MIMIT), an interventional radiology and endovascular therapy practice.
“Like most screening exams, D-dimer is a blood test with a high sensitivity and low specificity for diagnosing PE.
“However, some studies have shown that fibrinopeptide levels in the urine may have higher diagnostic accuracy than D-dimer.
“Ultimately, the key to diagnosing DVT/PE is a thorough history and physical exam by an experienced physician.”
What is fibrinopeptide?
FPB is a compound that’s released when a blood clot forms, and gets excreted through urine.
Dr. Fernandez says in the report that the urine test is more accurate than the D-dimer.
That’s because the D-dimer protein fragment becomes present in the blood after the DVT begins to break down.
Whereas the FPB is present in the blood before the DVT begins degrading, while the thrombus is still active.
The urine test, though, is still not refined enough to become a replacement for the D-dimer test.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}