

Running on a Treadmill: Hands On vs. Hands Off

Find out just how big a difference there is between jogging on a treadmill while holding on vs. hands off.
If you’ve been holding onto the treadmill while jogging, you’ve hardly done anything to make yourself a better runner outside, on the court or in the field.
Just because there’s a place to put your hands on the treadmill doesn’t mean you should do this when running on it.
When you run or jog outside, on the street, in a park, an athletic field or on a basketball court, your upper body moves completely differently than how it’s positioned if you’re holding onto a treadmill.
When you hold onto a treadmill while jogging, your upper body is locked in place, moving minimally.
If you were to run outside or anywhere other than on a machine, your upper body would be fully engaged.
This is the way you should run: the upper body moving in synch with the lower body, in unison, arms swinging.
This natural motion is completely tossed when you hold onto a treadmill—even if you’re in poor physical condition, overweight, older, what-have-you.
Holding the Front Bar while Jogging Makes You Lean Forward
Some runners who hold onto a treadmill lean INTO the machine when their hands are on the front bar.
However, holding onto the side bar doesn’t make things right, either.
Even if you’re a slow jogger, you simply should not hold on. Your arms are supposed to swing gently at your sides. Even toddlers, when “running,” know this basic rule of the human body.
By holding onto the bar in front, you’ll remove workload from your core.
Yes, the core works when you run or jog naturally without clinging onto anything for support.
If you’ve seen fit-looking people holding onto a treadmill while doing their make-believe running, don’t think for a second that this externally supported movement contributes to their nice physique.
A person can get a good body by strength training alone, coupled with a smart diet.
And again, holding onto the side of the machine isn’t any better. The body’s natural movement patterns still get disrupted.
“Holding on may giver joggers a sense of ‘more intensity,’ but it actually results in a less effective workout,” says John Whyte, MD, board certified internist in Washington, DC, and author of “Is This Normal? The Essential Guide to Middle Age and Beyond.”
If you’re up to jogging on a treadmill but feel out of shape, you will do yourself a giant disservice by holding on.
Instead, start out slowly with baby steps. Go 3.5 mph or even slower, zero incline.

Shutterstock/MikeBiTa
If your feet or some other area begins hurting or aching, then walk for a while.
But do not hold onto the treadmill when running.
This is a terrible habit. Even if you get dizzy, do not hold on.
Just go slower, hands free, arms swinging naturally, and give your body a chance to acclimate and adjust.

Dr. Whyte is the chief medical officer of webmd.com. Prior, he was the chief medical expert for almost a decade at Discovery Channel.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Depositphotos.com

Birth Control Pills Cause Blood Clots in High Risk Women

How long after taking birth control pills might a blood clot form in high risk women like smokers?
Blood clots are possible complications of using birth control pills, especially for women at higher risk for blood clots; namely women who smoke, and women over age 35.
However, is there an answer to this question: How soon after taking birth control pills on a regular basis, can a blood clot develop in women at high risk?
“A blood clot can form anytime while on birth control in any patient,” says Dr. Corinne Bazella, OB/GYN with University Hospitals Case Medical Center.
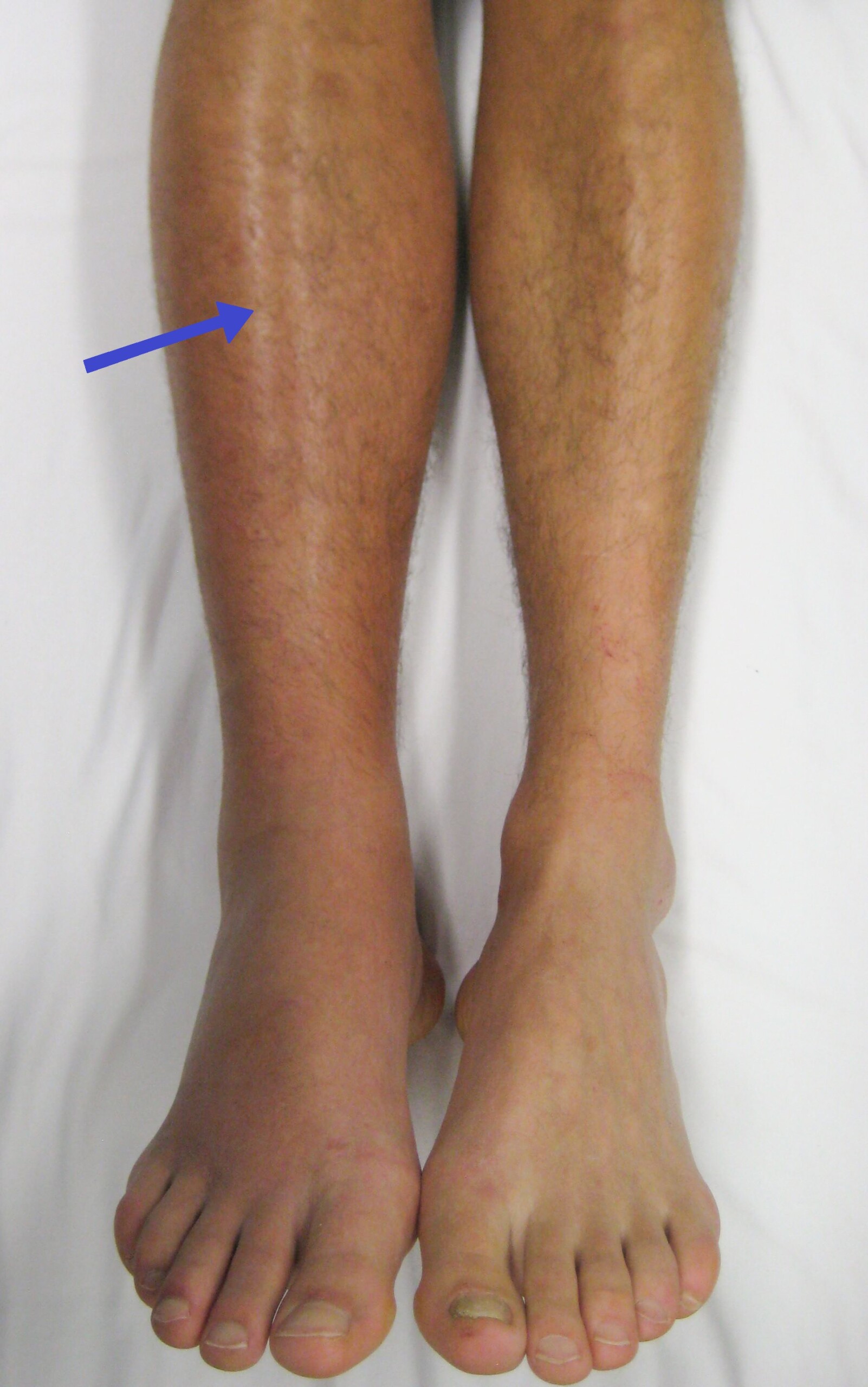
However, it happens more often in the first years of use. Blood clots form in the deep veins of the legs, and can travel to the lungs through the circulation, causing a life threatening condition called a pulmonary embolism.”
This kind of blood clot also goes by the name deep vein thrombosis, or DVT, and a woman on birth control increases the baseline risk of blood clots with birth control if she has any one of numerous risk factors.
Dr. Bazella lists the following additional risk factors for blood clots in women on birth control, but also for people in general:
- Inherited clotting disorders
- surgery, particularly joint replacement and abdominal
- prolonged immobility (especially in cramped quarters such as on airplanes)
- inertia from excessive desk work or bed rest
- trauma
- obesity, especially morbid
- smoking. If you’re a woman over age 35 who smokes, this puts you at considerable risk for blood clots while taking birth control pills that contain estrogen; avoid estrogen-containing birth control pills.
Ironically, a woman is much more likely to develop a blood clot while pregnant, than while on birth control pills.
Dr. Bazella explains, “In healthy nonsmoking women who are on combination low dose birth control pills, the risk of getting a blood clot is 12-20 women in 100,000.
“This risk greatly increases with pregnancy and is as high as 48-60 women in 100,000.
“Therefore, the risk of birth control pills causing a blood clot is less than the risk of getting a blood clot while pregnant, which is what you are trying to prevent!”
 Dr. Bazella’s expertise includes abnormal uterine bleeding, adolescent gynecology, contraception and menopausal care.
Dr. Bazella’s expertise includes abnormal uterine bleeding, adolescent gynecology, contraception and menopausal care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sore Throat from Exercise: Causes & Solutions

An ear, nose and throat doctor explains why exercise such as running can cause a sore throat and how to solve this problem.
Stacey Silvers, MD, first points out that a sore throat from exercising has two main causes: nasal obstruction and acid reflux.
“Poor flow of air through the nose makes it harder to oxygenate especially during a workout,” says Dr. Silvers, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
“We are inclined to open our mouths to breathe better. This, however, can make the throat dry, and for some people the throat can get sore, as the dry air can be irritating.
“The mouth is meant to eat through and talk through. We are obligated nose breathers and our nose is our air filter and air moisturizer.
“The causes of nasal obstruction are congestion and a deviated septum.
“Most of us have an element of both and some more extreme than others.”
What can be done about a sore throat caused by exercise?
“In most cases conservative medical management like saline nasal washes and nasal steroid sprays can improve nasal breathing,” says Dr. Silvers.
“If not, then some are candidates for a simple surgical option to open the nasal airway.”
Many people have acid reflux and are not aware of it.
Silent reflux can cause chronic sore throats, hoarseness and clearing of the throat.
Working out soon before you digest your food can allow acid into the back of the throat as you jump around, and cause pain in the throat.
“Many of us make thick protective mucous to coat the throat and protect from the acid, but some of us don’t have enough, and throat soreness is a result.
“Try waiting three hours after eating for your workout and cut down on highly acidic foods.
“If this is not enough you can try an OTC reflux pill one hour prior to exercise.”
If you continue to experience a sore throat that seems to be caused by exercising, despite implementing these measures, than see an ear, nose and throat physician.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

When I Swallow There Are Clicking Noises: Help!

An ear, nose and throat doctor explains the causes of clicking sounds when you swallow and what can be done about this.
“Many people experience clicking in the ear when they swallow or chew,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
“The two main causes of this are the Eustachian tube and the temporal mandibular joint (TMJ).
“The Eustachian tube allows the middle ear to ‘breathe’ and function at the same atmospheric pressure that is in our environment.
“This tube ventilates the middle ear space and opens into the back of the nose.
“The act of breathing through the nose will allow air into the middle ear space through the Eustachian tube.
“This Eustachian tube opens and closes as needed to allow the correct pressure in the ears.
“The act of swallowing and chewing will help open this tube, as the palatal muscles are attached to the Eustachian tube.
“This is why chewing and swallowing are natural for us when we are landing on an airplane and the ears feel pain or pressure and we want them to pop.”
So what can cause the clicking noises when we swallow?
“If the mucous is thick that lines the Eustachian tube, associated with allergy or dehydration, then the tube can be sticky, not allowing good ventilation, and an appreciation of a sound when the tube opens and closes,” explains Dr. Silvers.
Solution for clicking noises when swallowing?
“Decongestants and proper hydration are usually the best treatment options for this.

Shutterstock/Phovoir
“Some people have a patulous Eustachian tube and the tube simply functions poorly.
“Clicking can also be the bones rubbing in the TMJ joint. Some people have TMJ pain while others just experience the noises as the joint can rub with jaw movements.
“This is similar to a clicking in the knee when walking. You may want to visit a TMJ specialist and consider jaw strengthening exercises.”
Pay attention to how you bite into very hard food.
A bout of clicking sounds can be triggered from repeatedly biting into hard blocks of chocolate, for instance, straining the TM joint.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Holding on Treadmill Side Rails while Running: Bad Idea

Putting your hands on the side rails of a treadmill while running or jogging will sabotage your efforts and waste your time.
If you hold onto the side rails of the treadmill while doing your running, you’ll want to seriously rethink this bad habit.
When I was a personal trainer people would tell me they need to hold on “for balance” or to “keep from falling off.”
One man, around 60, told me he did it to keep steady. The irony was that he’d set the speed at 6 mph!
This is pretty fast for someone who feels unsteady!
He’d been going to the gym for years, holding onto the treadmill’s side rails and “running” 6 mph – and during that entire time, his body remained the same chubby form.
If this sounds like you—locked in the same state, same body weight—despite months or years of running on a treadmill—and you’ve been holding onto the side rails (or the front bar, or the console), then here’s what you should do:
LET GO. If you think you’ll fly off, this means that the speed you’ve been using is way too fast.
“Holding the rails while running on the treadmill actually affects the natural running posture and alignment,” says D’Wan Carpenter, DO, a board certified physical medicine and rehabilitation physician with SIMEDHealth in FLA.
“It decreases efficiency of the body due to the lax posture allowing the core abdominal and back muscles to relax.
“This change in the natural alignment can also cause increased stress on other areas, and particularly places much of the body weight on the upper extremities, which are not designed to be able to effectively support the whole body.”
How to Solve the Unsteadiness Problem
The chubby man was afraid of losing his footing. I told him, “Set the speed at 4 mph and tell me if you feel unsteady.”
He began jogging, without holding on, at 4 mph, and was able to keep his balance just fine.
He also felt that he was getting a better aerobic workout than he had been getting at 6 mph and holding onto the rails.
Look at the woman in the photo above. Does this in any way simulate outdoor jogging?
Even a light handhold on the rails will compromise effectiveness. The type of hold doesn’t matter — be it palms only; wrapping the fingers around the rail; pressing only the fingers to the rail; bent arms; straight arms — this will create a fake jogging experience that will hold you back from progress.
When a person runs or jogs naturally, arms swinging, their core (the soft structures of the low back and abdominal region) works to coordinate the movement between the lower and upper body.
You may not feel this core engagement, but it’s there. That’s why competitive sprinters and even longer-distance specialists (400m, 800m, even 1,500m) have great abs!
Nobody rocks a six-pack like a sprinter! Think that’s from thousands of crunches? Think again. It’s from running! Note the abs of soccer players or any athlete who does a lot of running.
When you hold onto the side rails (or anywhere else) of a treadmill while running…you cancel out abdominal and low back engagement, plus short-change leg involvement.

What in the heck kind of jogging form is THIS? Don’t say it’s better than a sofa workout. If you have to compare this deranged form to sitting on a sofa in order to validate it, then you just made a comparison to an extremely low standard!
The abs and low back get a free ride when you hold on. If you’ve been jogging 5, 6 or 7 mph on a treadmill and holding on…and doing no outside running…and then one day you go outside to do some running…the fatigue will begin biting at you very quickly because your body won’t be used to running without holding onto anything for support.
What makes this habit even worse is when someone presses UP on the side rails while running. This literally subtracts body weight off the tread.
I’ve witnessed this to the extreme: an “air jog.” What are people thinking when they do this?
Their arms are locked straight, shoulders scrunched up, as they keep their feet partially lifted off the tread as they air jog.
“Holding the rails also decreases the amount of weight bearing and reduces the number of calories burned during the exercise,” says Dr. Carpenter.
The calorie readout is generated by the selected speed and incline, regardless of what the user is doing.
Break the Bad Habit of Holding onto the Treadmill’s Side Rails when Running
Set the machine to a slower speed and let go.
See if you truly fly off or topple backwards.
If you’re apprehensive, set the speed to 3 mph and trot it.
Gradually increase the speed as you adjust.
If you normally “run” at 6 mph and say, a 10 percent incline…while holding on…you’ll have to drastically reduce these settings in order to let go.

Shutterstock/Den4is
Don’t assume you’ll sacrifice workload by letting go at 2 mph and 10 percent incline or 6 mph and zero incline.
Trust me: A 2 mph trot at 10 percent incline will get your heart going, and you’ll feel your calves working like you’ve never felt before (holding on removes significant workload from the legs).
Experiment with different settings to find a sweet spot range…without holding on.
If dizziness is the issue, again, use a very slow speed at first and swing your arms.
Give your body a chance to overcome the dizziness.
If balance is the issue, again, go slow at first and give your body a chance to acquire better balance.
It will never learn to balance if you hold on.
A person who can deftly run down the street after a loose dog, chase their children in a park or run like the wind in a parking lot after a blowing $50 bill, did not pick up these skills by holding onto a treadmill.
 Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Systolic Blood Pressure (Top Number) in Elderly: 150 vs. 140

Does it really make a difference if the systolic blood pressure in the elderly is around 150 vs. a little bit under 140?
The guidelines that systolic blood pressure should be below 140 are based on research that has, historically, targeted non-elderly people.
A report appears in Drugs & Aging, in which Leah Goeres, lead study author, points out that the goal of keeping the systolic blood pressure under 140 has been a longstanding protocol.
“Yet at the same time, there’s been some reservations among some doctors about how important this guideline is…in that, would 149 vs. 139 really make a difference in an elderly person?
“Keeping systolic blood pressure in older adults below 150 is important,” says Goeres in the paper. She says this is a “mild level of control.”
Then she adds that for the person over age 65, “that level is also good enough.”
After extensive analysis, Goeres maintains that more intensive blood pressure management, to keep it under 140, is not necessary for the older adult.
A potential side effect of drugs that lower blood pressure is orthostatic hypotension: Blood pressure quickly drops when someone rises from a chair, and this can cause passing out.
This problem is much more prevalent in people 80-plus.
The report explains that as men and women get older, the evidence becomes thinner that strict control of the systolic should continue to be very important.
Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths and Tricks: A Physician’s Advice,” concurs with the study’s findings.
“As a practical matter, in someone over 70 years of age, I consider a systolic pressure of 150 acceptable.
“Although it is a bit more desirable to go even lower than this in this group, this is difficult to achieve in the elderly without the use of multiple drugs, which increase the likelihood of objectionable side effects.
“So it’s usually best to strike a happy compromise with a less aggressive approach.”

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Alexander Raths
Source: sciencedaily.com/releases/2014/11/141103142322.htm

Falling from a Standing Position to the Floor in the Elderly

A fall in an elderly person from standing to the ground is deadlier far more often than you may think.
“Slip-and-fall” accidents may be the fodder of reams of personal injury lawsuits, but for the elderly, they are serious business, and fatal significantly more often when compared to non-elderly people, says a study.
When an elderly person takes a fall from a standing position and hits the floor or ground, this can kill them, and if this worries you, don’t let anyone convince you your imagination is overactive.
My father thought my imagination was overactive when I kept expressing concerns about my mother (elderly) taking a fall due to her frequent blackouts while standing (severe orthostatic hypotension).
Well, one day it finally happened (because I wasn’t present to prevent it), and six weeks later, she paid the price in the form of a brain bleed that had to be surgically drained.
A report in The Journal of Trauma: Injury, Infection, and Critical Care stresses the seriousness of short falls in the elderly.
It seems like a no-brainer to say that elderly people are less likely to survive a short fall than are younger individuals.
But the elderly are three times more likely, says the study (over 57,000 patients), to die from a short fall than are people under age 70.
The report points out that short falls should not be underestimated in the elderly, and that about 30% of people over 65 suffer from a fall every year.
What makes the potential for death or permanent disability greater is if the person loses consciousness while standing, and then falls, obviously unable to help break the fall due to lack of awareness. This puts them at very high risk for head injury.
But short falls are still potentially very dangerous for fully conscious victims.
My aunt took a short fall, broke her hip, then succumbed to postsurgical pneumonia.
The study found that about 4.5 percent of elderly individuals died after a short (ground-level) fall, whereas the death figure for those under age 70 was 1.5 percent.
Of survivors, the elderly stayed in the hospital longer, and just 22 percent were able to function independently after discharge. The figure for people under 70 was 41 percent.
Nevertheless, almost 75 percent of elderly people are not severely injured from short falls.
Unfortunately, some elderly people think they’re in this 75 percent group and thus don’t take all the safety precautions they should.
Fall Prevention Tips in Your Home
“Fall-proof your home — remove rugs and obstacles at ground level,” says D’Wan Carpenter, MD, a board certified physical medicine and rehabilitation physician.
“Utilize assistive devices (walker, cane, crutches) and get instruction on proper use from a physical therapist.
“Have vision, hearing and balance assessments at least yearly.
“Get active. As people age they tend to decrease their activity and become sedentary which also increases risk for osteoporosis [brittle bones].”
Dr. Carpenter is one of the nation’s top board-certified physical medicine and rehabilitation physicians, a national speaker, medical legal expert and independent medical examiner. She is founder and Chief Medical Officer of DJC Physical Medicine Consultants. Follow Dr. D’Wan on Twitter.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/glenda
Source: sciencedaily.com/releases/2010/11/101101130135.htm

If You’re a Slow Walker Will this Shorten Your Lifespan?

Slow walking in daily life may increase mortality risk in older people.
Years ago I worked in a department with many people over age 55. I confess: I had no tolerance for slow walkers, as they headed out of the department for lunch break, me stuck behind them in the narrow hall.
I was never ahead of them because my workstation was far from the exit, while theirs was much closer.
Getting stuck behind these slow walkers cost me time on my lunch break; when you have a 35 minute lunch break, every single minute counts.
Faster walking speed correlates to longer lifespan, says a report in the Journal of the American Medical Association.
Though the JAMA study focuses on older adults, it stands to reason that if you want to be a brisk walker in older age, you should begin walking fast when you’re younger.
I’m flabbergasted at how so few younger adults have a perk in their step. I would tell even my younger personal-training clients to make a habit of walking at a quick pace in daily life, even if it was just a short distance from their parked car to the entrance of a store.
Walking Speed and Survival
Stephanie Studenski, MD, led the study of 34,485 adults over age 65.
The analyses, which covered many years, revealed that walking speed was associated with variations in the likelihood of survival at all ages in men and women, but was particularly correlative over age 75.
“Predicted years of remaining life for each sex and age increased as gait speed increased, with a gait speed of about 0.8 meters [2.6 feet]/second at the median [midpoint] life expectancy at most ages for both sexes,” says the report.
Another finding was that when survival was predicted based upon gender, age and walking speed, this was just as accurate as predicting mortality based upon gender, age, self-reported function, chronic conditions, blood pressure, smoking and body mass index.
Why does walking speed predict mortality?
The paper points out that walking requires energy and control of movement, imposing demands on various bodily systems.
A person who walks slowly may have damaged organs. (But I’m betting that slow older walkers were also slow when they were young. After all, do slow young walkers turn into fast older walkers?)
As a fitness expert, I propose an additional explanation: If you don’t use it you’ll lose it.
Nevertheless, at a minimum, making a habit of walking briskly in daily life will certainly make it easier for you to move fast when you have to.
You won’t get fatigued or feel exhausted after doing a lot of required fast walking if your body is already used to this.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Actinic Keratosis Appearance vs. Squamous Cell Carcinoma

Actinic keratoses and squamous cell carcinoma can look similar; in fact, an actinic keratosis can turn into a squamous cell carcinoma.
Some doctors even believe they are one and the same, just at different points along the continuum.
Squamous cell carcinoma is the second-most common skin cancer. About 3,500 people in the U.S. die from it every year.
This skin malignancy grows slowly, but the deadliness lies in the delayed diagnosis.
The delay means that five percent of squamous cell carcinoma spreads, and this is what makes it lethal. As it grows locally, the destruction can become quite gruesome.
How common is squamous cell carcinoma?
Every year in the U.S. there are 250,000 new cases. Though this disease is strongly tied to sunlight exposure and usually grows in heavily exposed areas to the sun such as the face, scalp and limbs, it can actually grow in dark areas such as under the tongue.
Skilled Mimicker of Normal Aging Skin
Squamous cell carcinoma often initially masquerades as what many people might pass off as benign aging of the skin.
People may see that slowly developing dark pink, scaly patch of skin as a harmless consequence of getting older, or even harmless sun damage or the non-cancerous but abnormal actinic keratosis.
The individual may end up completely ignoring the stealthy growth, becoming desensitized to it, especially if he or she has already been diagnosed with similar-looking benign growths. Skin cancer never enters their minds.
The diagnosis of squamous cell carcinoma is on the rise in people under 45.
What Squamous Cell Carcinoma Looks Like
- Patchy area of skin, reddish or pink in color.
- Often scaly and/or crusty. The crust may be some shade of brown or brownish yellow.
- May also take the form of unsightly nodules or very raised bumps, sometimes with a horn-like structure sticking out of them.
- If growth is allowed to progress enough, the area can become quite “gross” in appearance.
Actinic keratosis (below), which is very common, results from sun damage, and if left untreated, 5-10 percent of these morph into squamous cell carcinoma.

Shutterstock/Dermatology11
I asked Jason Lupton, MD, how a doctor can tell the difference between actinic keratosis (which many people have but don’t realize it) and early squamous cell carcinoma.
Dr. Lupton is a board certified dermatologist practicing in the San Diego, CA area.
Dr. Lupton: Sometimes it is hard to distinguish between AK and early SCC. This is sometimes determined by response to treatment — if a lesion responds to basic treatment — liquid nitrogen or topical therapies — then a further pursuit is unnecessary.
If it does not, then the lesion is biopsied to determine if it has changed over into a squamous cell carcinoma.
Typically SCC’s feel more pronounced, a little bumpier, rougher and bleed more easily and are just more “hearty” lesions — although again, this is not exact.
A squamous cell carcinoma is also more likely to be tender or feel — to the fingertips — as though it has some substance beneath it.
Can squamous cell carcinoma develop from a mole?
I have never heard of an SCC developing from a mole. It derives from the squamous epithelium. They are different entities.
Since squamous cell carcinoma is tied to sun exposure, how is it that it can develop inside the mouth or anus?
SCC is related to sunlight exposure, but in those other areas it is associated with preceding HPV infections. So sunlight is not everything with this type.
If you suspect you have only an actinic keratosis, you should see a dermatologist just to be sure.
To prevent this from morphing into squamous cell carcinoma, your doctor will spray it with liquid nitrogen (cryotherapy) which should kill the atypical cells.
If there’s no response, a prescription cream can be applied.
 Dr. Lupton specializes in skin cancer prevention and treatment plus minimally invasive cosmetic procedures including mole removal, skin rejuvenation, wrinkle reduction and acne treatment.
Dr. Lupton specializes in skin cancer prevention and treatment plus minimally invasive cosmetic procedures including mole removal, skin rejuvenation, wrinkle reduction and acne treatment.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

DVT Treatment: Blood Thinner vs. Removal with a Catheter

Which is better for DVT treatment: a blood thinner drug or catheter-based removal?
A Temple University School of Medicine study involving 90,000 patients has an interesting conclusion.
The mortality rate between the two DVT treatments is the same. However, the catheter procedure brings more risk of bleeding.
This, however, is not related to the efficacy of the catheter treatment as far as removing the blood clot.
What is the catheter-based treatment for deep vein thrombosis?
This minimally invasive procedure involves catheter insertion through veins to deliver a clot-busting drug right at the site of the DVT.
This procedure costs more than anticoagulant therapy (blood thinner) and requires more days in the hospital.
Within 30 days of diagnosis, about six percent of patients with a DVT die.
In these cases, the blood clot breaks loose and travels to the lung (where it’s now known as a pulmonary embolism), cutting off oxygen supply.
Despite 90,000 cases being involved in this research, it was considered too small for any rock-solid conclusions to be drawn regarding the safety of the catheter-based therapy vs. anticoagulants alone for the DVT treatment.
Blood Thinning Drugs
The study might have you wondering about the use of blood thinning drugs for treating a DVT that’s already present.
“Blood thinners (anticoagulants) prevent formation of a new clot; they do not dissolve the clot,” points out Dr. Paramjit “Romi” Chopra, MD, founder of the Midwest Institute for Minimally Invasive Therapies (MIMIT), an interventional radiology and endovascular therapy practice.
“Catheter directed thrombolysis (removal of clot) is required in cases where the clot burden is extensive and the body’s natural mechanisms cannot dissolve it.
“We want to avoid chronic DVT and the post-phlebitic syndrome.”
Catheter-directed thrombolysis (thrombolysis = breaking up a blood clot) leads to a big reduction in the chances of developing this post-thrombotic or phebitic syndrome, an often debilitating condition of the legs.
PTS, a painful condition, is more likely to occur in patients for whom the clot occurs above knee level, particularly in the hip and groin area.
The American College of Chest Surgeons favors drugs alone, while the American Heart Association favors the catheter procedure — at least for people at low risk for bleeding.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}