
Can a 24 Hour Holter Monitor Miss Atrial Fibrillation?
Since atrial fibrillation isn’t guaranteed to occur in any given 24-hour period, isn’t it logical to conclude that a Holder monitor could miss it?
What exactly is atrial fibrillation?
Atrial fibrillation (AFib) is a heart rhythm disorder characterized by rapid and irregular electrical activity in the atria, the heart’s upper chambers.
This irregularity leads to an erratic heartbeat, which can cause symptoms like palpitations, fatigue and shortness of breath.
AFib increases the risk of stroke and heart failure if untreated.
If you were to view the number on a heart rate screen of a person with this heart arrhythmia, you would not see a steady number.
A normal heartbeat would show a steady number, give or take a few, such as a consistent range of 78 to 81.
If someone is in the midst of atrial fibrillation, you’d be seeing the numbers jumping all over the place quite quickly.
One moment the range might be high 70’s. Next moment it’s jumping around between 140 and 170.
Then suddenly it’s between 100 and 120. Then suddenly it’s 85, then 150. You get the picture.
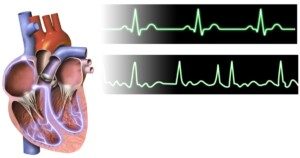
A-fib. BruceBlaus
If a doctor or you yourself suspect atrial fibrillation, and the next step is to wear a Holter monitor, you may then think that this won’t necessarily be an effective way of tracking the heart rhythm disorder — since the atrial fibrillation may be quiet during the time you have on the Holter device.
“Atrial fibrillation can occur at varying frequency and is often not associated with symptoms,” says Norman E. Lepor, MD, cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
“If it occurs less often than every 24 hours it can be missed on a Holter monitor,” he adds.
“Longer-term monitoring devices that can be monitoring for weeks to years can be used in those cases.”
So if the Holter device shows no abnormalities…this in no way means you don’t have A-fib.
Your doctor will tell you that you need to wear an event monitor that tracks heart rhythm for a longer period of time.
This device records your heart’s electrical activity continuously or at specific intervals to help diagnose irregularities or abnormal rhythms that may not be picked up by a Holter monitor.
Untreated atrial fibrillation is a major risk factor for an ischemic stroke.

Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

The Truth About GAS Causing Heart Palpitations

A cardiologist, not an online thread layperson, answers the question, “Can gas cause heart palpitations?”
Is there a true connection between farting and a flip-flopping heart?
“There is no clear cause and effect relationship between gas and palpitations. As common events, they can occur together,” says Norman E. Lepor, MD, cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
So then, palpitations of the heart cannot possibly ever be caused by gas?
Dr. Lepor responds, “Only if one feels very embarrassed by the release of gas in public.”
The beating of the heart is driven by electrical signals. If you fart, there is no way that this will disrupt those electrical commands. Not directly, anyways.
Passing gas involves the digestive tract. Heart palpitations involve the cardiovascular system.
Though some bodily systems work closely together, such as the musculoskeletal and the nervous system, this is not the case with the digestive and the cardiovascular system.
So if you find that your heart skips a beat or jumps somewhat right after you pass gas … then consider the possibility that it’s embarrassment.
And try not to let one out when you’re around other people, especially inside a car or an elevator.
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Master1305

PVCs After Exercise: Forerunner of Heart Attack?

Have you been having PVCs right after you stop exercising, as in, you’ve been running on a treadmill or doing the burpees or pushups, and within seconds of ceasing the activity…you feel the premature ventricular contractions?
Does this mean you’re in trouble, as in, a future heart attack is awaiting?
“Post-exercise PVCs can be considered a risk factor for cardiac events if they are associated with underlying cardiac pathology,” says Norman E. Lepor, MD,cardiologist and internal medicine specialist Norman E. Lepor, MD, who’s with Cedars Sinai in Beverly Hills, CA.
There’s a few things to consider here before you start panicking. Dr. Lepor mentions “cardiac pathology.”
If you just sprinted 14 mph for 30 seconds on the treadmill…chances are, you do not have cardiac pathology.
Nobody can just run like this. It requires training to get to this ability, even though it’s not exactly collegiate track team skill.
But a person with a pathologically compromised heart will not be able to sustain the training that’s required to reach this level.
Try it sometime: A young adult just starting an exercise program will be tossed off a treadmill or forced to step off if they attempt to run it, WITHOUT holding on, at 14 mph.
Another issue to consider, if you’ve been having PVCs post-exercise, is the anxiety factor.
You just rapidly squatted deep for 20 repetitions while holding a 40 pound medicine ball. You now feel the PVCs as you take a seat to catch your breath.
Chances are not high that there’s heart pathology involved, simply because this level of exercise—though not Olympic caliber—requires a trained body.
Many people off the street can’t even pick up a 40 pound ball, much less squat 20 times in a row with it.
Do you feel anxiety after finishing a set or ceasing an aerobic-based burst?
The anxiety may be from worrying about your exercise performance.
It may be from concern that an injury still hurts—did the set just make the injury worse?
And maybe you’re worried about PVCs in general and heart attacks, and after completing your intense exercise set, you started thinking about PVCs…and voila…you felt a few!
The adrenaline is going like mad, spurred by the exercise, and then spurred even more once you come to a rest and begin worrying about PVCs.
The conditions, then, are ripe for PVCs, since these can be triggered by adrenaline from anxiety over having a heart attack.
If you notice that PVCs regularly come right after exercise in the absence of anxiety, this increases the odds that there’s cardiac pathology.
Dr. Lepor says, “People with PVCs associated with activity should undergo a routine cardiac exam including a stress test and echocardiogram.”

Heart attack symptoms
If you fear a heart attack, don’t put off making the doctor appointment.
Having performed over 4,000 coronary angiograms and angioplasties, Dr. Lepor has focused on prevention and treatment of coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: MikeSaran

What Bleeding in Between Periods & Missed Periods Might Mean
Bleeding or spotting in between periods CAN mean cancer but also many other benign causes, and missed menstruation has a ton of causes.
Have you ever spotted in between periods? Seen blood stains on your underwear or on the tissue paper after you wiped yourself?
What’s the first thing that came to your mind?
Or, if this has not happened to you, what do you THINK would be the first thought that occurred to you? “Could I have cancer?”
Well, the truth is, bleeding in between doesn’t always mean cancer. On the other hand, it’s a very common symptom of uterine (endometrial) cancer.
It can be a sign of ovarian cancer, but only rarely.
Another cause, believe it or not, can be sitting on a hard bicycle seat and pedaling furiously — with no cycling exercise history, or after a long absence from cycling.
The jarring and pressure against a hard seat can cause mild spotting, but this does not come from the genital area; it’s likely from microscopic tears in the anal area.
This actually happened to me after pedaling furiously on a stationary bike—so hard, in fact, that when I was done, the bike had moved across the floor.
Another cause is doing rigorous jumping drills — again, with no jumping history, or after a long absence from jumping routines.
This has happened to me. But the spotting in these cases is either immediately after the exercise, or a little later on, and does not persist; it’s usually a one-time occurrence shortly after the activity.
If you haven’t done these activities and are bleeding (or spotting) in between periods, take this cue seriously, especially if you are postmenopausal.
It can mean cancer, though it can also have many other, less serious causes (which is actually usually the case).
Postmenopausal vaginal bleeding is a symptom of cancer in about 30 percent of cases.
About 90 percent of women with uterine cancer experience vaginal spotting or bleeding in between periods, or after menopause, according to the American Cancer Society.
Vaginal bleeding is often the first clue that something is wrong.
Other symptoms may not show until the disease is advanced.
Other symptoms of uterine cancer: prolonged periods; a pink, watery or white vaginal discharge (note: a milky-white discharge is also normal; this is known as “between-period discharge”).
It’s best to frequently monitor yourself so that you become familiar with what is normal and routine for your body, and what suddenly becomes different.
This could include pain during intercourse; a pelvic mass; pelvic pain; and unexplained weight loss (these usually occur in later disease stages).
Known Risk Factors for Uterine Cancer
• Diabetes
• Advanced age
• Longer menstrual span (i.e., time span from menstrual onset in adolescence to menopause)
• Never having been pregnant
• Obesity
• Higher lifetime-exposure to estrogen
• Pelvic radiation therapy
• Family history
• Breast/ovarian/colorectal cancer personal history.
Bleeding in Between Periods: Summary
The patient’s age factors into most probably causes, says Justin Chura, MD, a gynecological oncologist in Philadelphia, PA.
“For example, in a 20-year-old woman on birth control pills, bleeding between periods is very common, and the risk of cancer is extremely low.
“On the other hand, for a woman in her early 50s who still has menstrual periods and is now experiencing bleeding in between periods, further evaluation is needed including an ultrasound and possibly a biopsy.”
By the way, eating beets or juiced beets can cause urine to have a reddish tinge (from the beets’ red pigment), and this might pass for “bleeding in between periods.”
Missed period but not pregnant or menopausal?
Relax, it’s not a sign of cancer. Other causes of a missed period include:
– Severe dieting/substantial weight loss in short period of time
– Excessive, rigorous exercise, particularly related to endurance training
– Unusual amounts of stress
– Fast weight gain, or obesity
– Bulimia (vomiting food to lose weight)
– Birth control pills
– Depo-Provera injections
– Hormone imbalance
– Polycystic ovarian disease (hormone imbalance interferes with normal ovulation)
– Breast feeding
– Travel
– Illegal drug use
– No known cause – missed periods (in absence of pregnancy) are not that uncommon, and may actually mean nothing is up at all.
Nevertheless, it would be wise to see a gynecologist if you have missed two periods in a row, or two periods in 12 months.
 Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/siam.pukkato
Can Your Bad Cramps Be from Cervical Cancer?

Many disorders can cause bad cramps in the lower abdomen or pelvic area, but what are the odds that your recent-onset cramping is being caused by cervical cancer?
Yes, cervical cancer can cause bad cramping, but where does this disease rank as far as likelihood that it’s causing your discomfort as opposed to a benign cause?
Cervical cancer can cause pelvic or lower abdominal cramping.
“Cervical cancer can cause cramping in the pelvis,” says Justin Chura, MD, a gynecological oncologist in Philadelphia, PA.
“This can occur as the tumor expands on the cervix and pushes on the bladder and the bowel.”
Advanced Cervical Cancer
“Advanced cervical cancer can cause bleeding and increase the risk of infection, which can, in turn, cause cramping,” says Mylaine Riobe, MD, founder of Riobe Institute of Integrative Medicine. Dr. Riobe, who’s board certified in ob/gyn and integrative medicine, is the author of “The Answer to Cancer.”
Cramping, however, is a common symptom and it is not specific to cervical cancer.
In fact, a sensation of cramping in the abdominal or pelvic region is one of the most common symptoms that doctors see patients about.
Causes are far-ranging and include strained muscles and irritable bowel syndrome.
“In other words, there are many more causes of cramping that are not cancer related,” says Dr. Chura. “This can include cramping from fibroids, endometriosis, infections and painful menstrual cycles.”
Inflammatory bowel disease is another possible cause, though the pelvic cramping will likely be accompanied by aches elsewhere in the body due to the “enteropathic arthropathy” of inflammatory bowel disease.
Have a Pap smear if you’re worried about cervical cancer. This disease is SO easy to detect in its earliest stages.
The Pap smear can also detect precancerous changes in the cervix.
Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.

Dr. Riobe has helped thousands of patients overcome difficult illnesses by addressing root causes, not just masking symptoms. The Riobe Method focuses on the prevention of disease, not the prevention of death from disease. She has 20+ years’ experience using integrative techniques to treat diverse patients.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/siam.pukkato
Can Chronic Cervicitis Lead to Cancer?

Cervicitis is inflammation of the cervix, but can this turn into cancer?
This is a question that many women would like to know, so I posed it to Justin Chura, MD, a gynecological oncologist in Philadelphia, PA.
“Chronic cervicitis does not lead to cervical cancer,” says Dr. Chura. “Cervicitis means inflammation. Inflammation can have multiple causes. This can include infection.
“The cause of cervical cancer is the human papilloma virus. Most of the time, chronic cervicitis is asymptomatic.
“Meaning, findings are seen on a Pap test, but the patient has no symptoms. When this is the case there is no recommended intervention.”
Perhaps the fear that cervicitis can lead to cancer or raise the risk of it originates from the fact that it can be discovered with a Pap smear — some patients wrongly connect dots and draw erroneous conclusions.
The risk of cervical cancer goes UP when a woman has multiple sex partners!
A sexually active woman should have a Pap smear annually, though this is also usually recommended for all women.
Frequency of the screening Pap smear should be discussed with one’s OBGYN.
Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Does Cervical Dysplasia Always Turn into Cancer?

“Just because a woman is diagnosed with cervical dysplasia does not mean that she will develop cervical cancer,” says Justin Chura, MD, a gynecological oncologist in Philadelphia, PA.
A Pap smear will detect cervical dysplasia, which means atypical cell growth that’s non-malignant.
Dr. Chura explains, “For women with mild cervical dysplasia, no treatment is recommended, as this process resolves on its own most of the time.
“In addition, mild cervical dysplasia does not lead to cervical cancer. Severe cervical dysplasia, however, can lead to cervical cancer if not treated.
“Fortunately, treatments such as a cone biopsy are very effective in preventing this process from turning into cervical cancer.
“For some women with severe dysplasia, hysterectomy may also be an appropriate treatment option. The progression from severe dysplasia to cancer takes several years to occur.”
Luck of the Draw: Who Will and Won’t Develop Cervical Cancer
Dr. Chura explains, “The problem is that we do not know for which patient it will turn into cancer and for which patient it will not.
“One risk factor that a woman can control in potentially decreasing the risk of dysplasia progressing the cancer is exposure to tobacco.
“In other words, smoking should be avoided in women within all women, but especially in women with cervical dysplasia or cervical cancer.” Quit smoking!
Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

What’s that Discharge after Colposcopy and Cervical Biopsy?

Here’s reassuring information about your discharge after a colposcopy and cervical biopsy.
Just how common is the discharge?
“Experiencing discharge after colposcopy and cervical biopsy is common,” says Justin Chura, MD, a gynecological oncologist in Philadelphia, PA.
Causes of the Discharge
“Sometimes the discharge can be due to medications applied to the cervix to stop any bleeding after the biopsy,” says Dr. Chura.
“A common medication will often cause a discharge that looks like coffee grounds when it mixes with blood.
“Discharge can also be part of the healing process from the biopsies.
“As long as the discharge does not have a significant odor and there are no associated fevers or other significant pain, this usually stops within two weeks after biopsy.”
What is a colposcopy?
The purpose of a colposcopy, which takes five to 10 minutes, is to closely examine the cervix, vagina and vulva for any signs of disease.
The instrument that’s used is a colposcope, which is a lighted, magnifying device.
Why would a doctor would recommend a colposcopy?
One reason is an abnormal Pap smear result. Another reason is unexplained vaginal bleeding.
During a colposcopy, tissue is removed that can be sent to the lab for a biopsy.
A colposcopy can show the following:
- Precancerous changes in cervical tissue
- Precancerous changes in vaginal tissue
- Precancerous changes vulvar tissue
Complications of the procedure that are worrisome do not include the commonly observed discharge.
Call your physician if you experience any of the following:
- Bleeding heavier than what you typically experience during menstruation
- Chills or fever
- Severe abdominal pain
Are you terrified of your upcoming colposcopy?
To ease your anxiety, think of a colposcopy for what it actually is: a closer way for a doctor to examine your cervix, vagina and vulva, and a more effective way to collect tissue.
A recommendation for the procedure itself DOES NOT MEAN YOU HAVE CANCER.
Dr. Chura provides standard cancer care and robotic surgery for cancers of the cervix, ovary, uterus/endometrium and vulva. He is affiliated with multiple hospitals including Jefferson Einstein Philadelphia Hospital-Jefferson Health and City of Hope Cancer Center Atlanta, and has been in practice for 20+ years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

Two Ways Melanoma Can Become Deadly

If melanoma is caught early enough, it’s highly curable, but many people let it slip by, and this is how this deadly skin cancer can get past even health-conscious people.
Two ways that this can happen stand out to Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
“One way is that a change noted in a mole has already gone too far by the time you seek attention,” begins Dr. Prystowsky.
“For instance, when a melanoma is already bleeding at the time of diagnosis, it has ulcerated and the risk is high that the melanoma has already metastasized.
“Even determination of the actual thickness of the melanoma [in the case of a bleeding one], an important factor in assessing the risk of the melanoma, is compromised because the top of it has been destroyed.”
Appearance
“The second way is that some melanomas do not look like the usual pictures of melanoma and they can grow quickly,” continues Dr. Prystowsky.

Melanoma on a cheek
“This nodular type of melanoma may have no brown or black color and may look like a pink to reddish bump on the skin.
“Usually the only reason for testing it is that it is a new bump or it may resemble a basal cell carcinoma; the biopsy result for doctor and patient is typically a surprise.
“Nodular melanoma can be particularly deadly because it is capable of metastasizing from the beginning of its existence.
“An early diagnosis and treatment does not guarantee a cure. Approximately 15% of all melanomas are in this category and it is very bad luck for the patient.”
Spread
“Once melanoma has metastasized, regardless of the original type of melanoma, it has spread to lymph nodes or other organs.
“This is very serious because it may cause death.
“There are several new treatment advances which can now put metastatic melanoma into remission, but they do not work on all patients.”
Prevention and Screening
Dr. Prystowsky stresses the importance of avoiding excessive sun exposure and avoiding tanning beds; using a sunscreen with an SPF of at least 30 and getting regular clinical skin exams by a dermatologist.
She recommends the ABCDEs:
Dr. Prystowsky explains that “A stands for asymmetry, as in a lopsided appearance to the mole.
“B stands for border irregularity of the mole, as in the appearance of the coast of Maine on a map.
“C stands for colors that are not uniform in the mole or a color change.
“D stands for the diameter of the mole. If the mole is over 6 mm in diameter, the risk is greater that the mole is abnormal.
“E stands for evolving because a mole that is changing such as itching, bleeding or showing other new symptoms suggests a possibility of melanoma.
“Because about 50% of melanomas arise in a pre-existing mole, seeing these changes in a mole should prompt a visit to the dermatologist.”


In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/wavebreakmedia
Melanoma: How Not to Let This Deadly Skin Cancer Get Past You

There’s a disturbing case of a young woman who let melanoma skin cancer get past her, and as a result, she died. But it didn’t have to be this way.
Melanoma kills about 10,000 Americans every year. This skin cancer kills by spreading to organs.
But melanoma has a near-100 percent cure rate if caught early. All a person needs to do is check his/her skin for suspicious moles.
Sounds simple enough, but many people will see a suspicious mole and make excuses not to see a doctor. I one day read about a woman with melanoma, and the poor service by her doctors was alarming.
This young woman with melanoma died, and it’s impossible to rule out that this cancer death can be traced back to inept doctors.
If you have a mole removal, there are things you absolutely must know:
- The doctor should be a dermatologist.
- The doctor should remove not just the mole, but a margin of skin around the mole and beneath it.
- The doctor should send all of this tissue to a pathology lab to see if the cells are melanoma or other skin cancer.
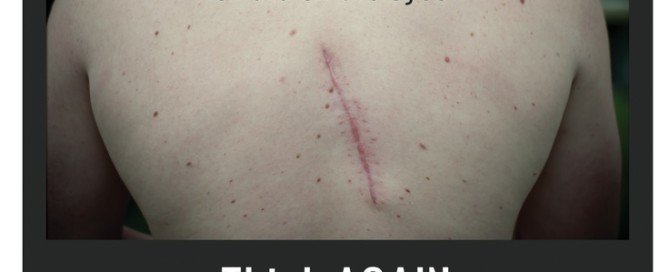
In the case of the melanoma death, the patient wanted mole removal for cosmetic reasons. She was 14 and the mole was on her back/shoulder area.
About six years later the scar from the mole removal began itching and bleeding.
A doctor diagnosed an infection and prescribed antibiotics. He didn’t even scrape a tissue sample for biopsy.
If I recall the magazine article correctly, I think it was this doctor who found a swollen lymph node in the woman’s neck and thus, she saw another doctor for that.
In this next exam, the doctor was suspicious about the mole removal scar and had a sample tested for cancer.
• It came back positive for melanoma.
• The melanoma eventually spread and killed the young woman.
Steps to Take for a Favorable Outcome
- The patient needs to be informed ahead of time by doing some “homework.” Don’t walk into a doctor’s office completely in the dark without a clue. Medical errors are a leading cause of death in the U.S. (cdc.gov/HAI/surveillance/).
A favorable outcome is far more likely if a patient or patient’s parent always adheres to this rule:
If something is removed from the body, insist that the doctor send it to a lab for a biopsy, REGARDLESS of what the doctor thinks it is.
Do not let a doctor’s assurance of, “Oh, it’s nothing to worry about,” con you into passing up a biopsy. Over a million people in America every year are diagnosed with skin cancer.
In the case of the young women with melanoma, though this was six years before the area started showing symptoms, it’s possible that a biopsy would have revealed atypical or abnormal cells: a red flag for future cancer.
The doctor should have taken it upon himself to send the mole and skin tissue to a lab, whether or not the patient requested a biopsy.
It was later learned that the doctor had thrown out the tissue instead!
- Laypeople need to realize that they should be proactive with the health of their skin and body. Even if a mole removal is done for cosmetic purposes, insist on a biopsy regardless of what the doctor says.
Another problem is that many people are afraid to question a doctor or make sure a doctor does A, B and C.
When I had a patch of skin scraped for biopsy, I jokingly said to the doctor when I saw her pick up the little container that had the tissue, “Oh, make sure my full name is on there!” (The result was benign.)
WE ARE THE CUSTOMER. We are paying the doctor for a service. We have as much right to question a doctor and make sure he does A, B and C, as we do the people who are building a house for us, or laying in our new carpet, or putting in our new furnace, or fixing our car’s engine!
Take a good look at the different melanomas below.
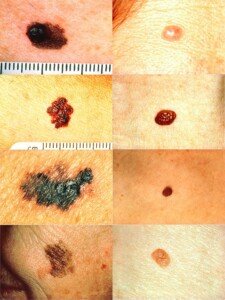
The person who wouldn’t hesitate to oversee what a mechanic is doing to his car might be the very same person who’s afraid to ask a doctor lots of questions!
- Six years later when the mole removal area began itching and bleeding, this should have been a red flag for melanoma. When you have this basic knowledge, it will profoundly affect the outcome. When you don’t have this knowledge, precious time is wasted (during which melanoma grows) before the correct diagnosis is finally made.
If a mole is changing, suspicious, or the mole removal scar is doing strange things, FIRST THINK MELANOMA. Do not think anything else.

Shutterstock/Andrey_Popov
When you first think melanoma, you then can’t help but act accordingly, in that you will demand a biopsy rather than settle for a benign diagnosis.
Yes, we’d all like to hear it’s just an infection. But unless you have that biopsy, you cannot rest assured it’s not melanoma.
I can’t believe a doctor could look at an itching, bleeding scar and exclude melanoma without a lab test.
Though nobody likes to automatically default to an “It’s melanoma” mindset, this is what MUST be done.
The next step is see a dermatologist ASAP and insist on a biopsy to rule out melanoma.
No. 1 course of action when a mole removal scar, or mole, itches and bleeds: SEE IF A DERMATOLOGIST CAN RULE OUT MELANOMA — and not with a visual inspection, but with a BIOPSY.
Always assume the worst, and then work backwards from that worst-case scenario. This is the difference between life and death.
“With melanoma there is no guaranteed way to make sure it does not get past you,” says Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
Nevertheless, it really pays to become very acquainted with the warning signs of this disease.
Melanoma can be deadly two ways: Dr. Prystowsky explains.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}