

5 Reasons a Woman with Broad Shoulders Should Feel Great

Women who have broad shoulders should prize their dimensions, not despise them!
Why is it that if a woman has a trait that’s “more,” she so often detests it?
I wonder if women who hate having broad shoulders, or who hate being very tall, etc., were raised to believe that it’s wrong for women to take charge in situations, voice opinions and show some feistiness and fire when push comes to shove.
I’m a woman with broad shoulders and I love them!
Though I’m not super tall, my height of 5-8 in combination with my broad shoulders creates in me a presence that can hardly be described as demure and classically feminine.
#1. They can be intimidating to a man.
WAIT — before you go, “What? That’s the problem!” let me say this: A man is less likely to mug a woman whose shoulders are as broad as his.
A rapist might think twice before “interviewing” a potential victim when he spots the broad shoulders.
To a man, this stunning trait in a woman might indicate the ability to throw a knockout punch — whether she can or can’t. It’s all about what seems to be.
#2. They can help you find Mr. Right.
Yes, that’s correct: Broad shoulders in a woman can help her quickly determine which men are put off by a trait that, quite frankly, should be seen as exceptionally attractive.

Shutterstock/eanstudio
Though many men find this trait to be sexy and appealing, it’s also true that some men do not like broad shoulders in the opposite gender.
If a man blows you off because of this trait, then this isn’t the right man for you, and you found out before you wasted six months of your life dating him (if you had “normal” shoulders).
#3. When the body gets old, it shrinks.
Look at the shoulders of elderly women. They’re atrophied, often shapeless.

Is this where your shoulders are headed? Shutterstock/wavebreakmedia
Now, if a woman does some serious strength training before she reaches senior age, she can dramatically delay and partially prevent much of the shriveling up of her upper body with old age.

Sharon Smith of Denver, CO, is 71 years young! Are her shoulders awesome or WHAT!
A woman with broad shoulders won’t look as shrunken, vulnerable and frail when she’s elderly. Clothes will fit much better on her old body; the shoulders will be like hangers.
#4. I have to believe that this trait means that she is that much more efficient at certain sports.
I’ll admit I’ve never read any research studies on this topic, so I’m basing my assessment on common sense.
Imagine a woman with a small upper body swinging a golf club to make a 250-yard drive; throwing a softball to the first baseman from center field; attempting to whip out a Frisbee to her dog to chase after; or lifting heavy weights.
Now, imagine a woman with broad shoulders doing these same things. Seems to me that broad shoulders would produce more torque; torque is a physics term that applies to rotary force.
#5. This next reason might seem silly…
A woman’s broad shoulders better hold up a purse strap. I’ve seen those with tiny shoulders constantly pushing up a falling purse strap!
I’ve seen them keeping their shoulder in a hunched-up position to prevent the strap from slipping.
So such are my five reasons a woman can feel great about having broad shoulders!
Sharon Smith has been in the fitness industry for 25+ years and specializes in the over-40 client.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/YAKOBCHUK VIACHESLAV

Six Myths About Dog Muzzles

Muzzling a dog has received a really bad rap, and many people even believe that putting a muzzle on a dog is cruel or inhumane.
This perception was perhaps ignited by images of greyhounds being caged and muzzled with wire contraptions.
Myth #1: The muzzle interferes with the dog’s breathing.
My parents thought this because after they removed their German shepherd’s denim muzzle while in the car, he began panting. However, look at the design of a muzzle.
The animal’s nostrils are exposed. My parents thought that breathing was compromised because the design prevented barking, i.e., opening his mouth.
Eventually my mother asked a vet if these devices cut off breathing, and the vet assured her that they do no such thing.
Myth #2: Muzzles stress a dog out.
This same vet then added, “Muzzles relax dogs and make them feel secure.”
And I have witnessed this many times with their dog; he seems most relaxed when it’s on him, and he even falls asleep with it on.
Of course, at a buzzing vet clinic, the gadget doesn’t do much to calm the dog, but that’s because at the clinic, there is sensory overload; the animal could see, hear and smell all the dogs there, plus the cats, in the waiting room.
Myth # 3: Muzzles prevent a dog from drinking.
This depends on the design of the contraption.
A mesh design, also known as a basket design, will allow drinking, if the water is high enough in a bowl.
The dog simply proceeds to drink, and pushes down into the bowl, and the water level rises through the muzzle and the animal can lap up the water.
The other common design, in which the gadget is a solid material such as denim, will not permit drinking.
Myth # 4: A muzzle doesn’t guarantee protection from getting bitten.
Again, this depends on the design. The mesh or basket type will, indeed, prevent biting.
Myth # 5: A muzzle hurts.
They do not; make sure they are not strapped on too tightly, that’s all.
Myth # 6: A dog will associate a muzzle with punishment.
You will determine this, not the muzzle.
If right after you put the device on your dog, you yell at him, strike him, lock him in a room, or subject the animal to some other aversive condition, then yes, he will associate the device with punishment.
I put one on my parents’ dog before giving him medical injections — 30 minutes before, so that he wouldn’t associate the device with needles.
A treat at the bottom of the muzzle will make the dog associate this device with getting a treat — and that’s always a happy time for a dog!
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

NDEs Are Real: 3 More Commonalities to Near-Death Experiences

Here are 3 outstanding points that support the idea that NDEs are very real.
But first, here are the well-established common features of an NDE that point to the idea that they are very real:
Being outside one’s body and observing conversations, actions and physical appearances of people they’ve never met—that are later verified.
Returning from the NDE with knowledge that the individual could not have possibly known unless they had learned it from the deceased loved-one they encountered during the NDE.
Other common features point to the reality as well. For example, why would everyone, from any walk of life, any religion, any age, encounter some form of a blinding or brilliant light that never hurts their eyes?
- Why do so many have a life review?
- Why are the experiences so overpowering that the NDE’er’s outlook on life and attitudes towards people are profoundly altered?
And that barrier or border; nearly every NDE has this feature: some kind of threshold that the person knows that going through it will mean a point of no return.
There are three additional features that are common to all NDEs that heavily point to their reality.
Skeptics, or people who insist that near-death experiences are hallucinations or dreams manufactured by dying brain cells or brain cells starved of oxygen, really need to ask themselves the following questions:
#1. Why is it that in these alleged hallucinations or dreams…the person never actually crosses that threshold and gets into Heaven?

Freepik.com, creativeart
Nobody ever comes back to say, “I got into Heaven! There was this bridge, and I knew that if I crossed it, there’d be no going back.
“I wanted so much to cross it, and my deceased loved-ones beckoned for me, so I did—I crossed the barrier—and I was officially christened an angel!”
No sir, NDE’ers never report crossing over. They say, 100 percent of the time, that they either decided to return to their body, or, they were forced back into their body.
Funny how none have ever reported that they wanted to go back to their body, but were forced to go through that barrier or gate!
If NDEs are only a dream or hallucination, then anything should go. So why don’t NDE’ers ever actually cross over, then “wake up” from the dream to report this?
#2. Part of many NDEs is the OBE: out of body experience.
Now don’t you find it quite interesting that whenever someone reports the “hallucination” of being outside their body…that they never also “hallucinate” or “dream” that their body is doing anything more than just lying there unmoving with its eyes are closed?

Why don’t NDE’ers ever report, “I was floating above my body. I then saw my eyes open and my body sit up, and then my body walked across the room and called Dominoes to order a pizza. The pizza came seconds later and I watched my body eating it.”
Dreams during sleep, and hallucinations from brain chemistry gone awry, typically LACK logic.
So why don’t NDE’ers report that they witnessed their body get up and speak to the NDE’er?
Or order that pizza? Why doesn’t the NDE’er ever have conversations with his or her “body”? Or jump off the operating table and tell the doctors, “Hey, I’m cured!”
No sir. The body always just lies there, not moving. It never suddenly grabs the resuscitation paddles and says, “Hey Doc, enough already.” Aren’t dreams and hallucinations supposed to be rather wild?
Yet the “dream” or “hallucination” of hovering over one’s own body are quite bland: The body never does anything but lie there.
#3. If these are dreams or hallucinations…why don’t NDE’ers ever experience their fantasies?

©Lorra Garrick
For example, many people fantasize being intimate with their favorite movie star — or gorging on the best chocolate cake in the world. The one at the top of this article would be one heavenly experience!
You’d think that in these exceptionally vivid dreams or hallucinations, the dying brain cells would conjure up a very stunning replica of, say, Marilyn Monroe, Elvis Presley, Sharon Stone or Harrison Ford — there for the taking by the NDE’er — who then proceeds to spend what seems like hours with this facsimile of their favorite entertainer.
So those are the three questions that skeptics of NDEs need to ask themselves.
The overnight dreams and drug-induced or mental-illness-induced hallucinations of people do NOT contain common threads like NDEs do.
Really, if you were to ask 1,000 people what they dreamt last night, you’d get hundreds of very different stories.
Ask 1,000 NDE’ers to explain their “dream,” and you’ll get the same thing over and over and over (though the details will differ, e.g., how they approach the light, shape of the light, type of barrier, presence or absence of music, etc.).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Gts

If NDEs Are Real, Why Aren’t They All the Same?

Why do NDEs differ so much, despite the common themes?
Some commonalities among near-death experiences are that of overwhelming joy and peace; reunions with deceased loved-ones; a threshold that the NDE’er knows that once crossed, there will be no return; the absence of time; brilliant lights; and a feeling that one’s consciousness is intertwined with everyone else’s.
However, all of the details that can be filled in differ wildly from one NDE to the next.
There is no universal setting. Messages and interactions differ tremendously.
The appearance of spirits or angels differs. Why would angels or spirits look so different from one NDE to the next?
Why does God or Christ look different to different people?
And that light—that blinding light—sometimes it’s a sphere. Sometimes it’s a pillar-like shape.
One man described it as strands or strings. Sometimes it’s an orb. Sometimes the light has no shape or form; it’s just there.
Another differing aspect of the NDE is the “barrier” or threshold that the person instinctively knows that if they cross it—they won’t be able to return to their physical body.
In some NDEs it’s a bridge over some water. In one NDE that I read about on nderf.org, the barrier was a set of glass doors.
In another, the barrier was a ball of light. Sometimes it’s a walkway of sorts. Does the after-life have a lot of different barriers?
“No two near-death experiences are the same,” says Jeffrey Long, MD, author of the New York Times Best Seller, “Evidence of the Afterlife: The Science of Near-Death Experiences.” Dr. Long is a radiation oncologist in Houma, Louisiana.
Sometimes the NDE’er will spend time inside buildings or libraries and be “walking” on marble. Sometimes the NDE will involve water.
Or it may be fields of grass and flowers. Sometimes there’s music. Other features that are not common to all include panoramic vision, a life review and colors that the NDE’er cannot describe other than to say that no such colors exist in the physical world.
Interestingly, you’d think that at least some NDEs would include gorging on the most delicious foods the person has ever eaten without getting full—either the best versions of their favorite foods in the physical world, or, new tastes and gustatory experiences they’ve never had before.
After all, eating is one of life’s most intense pleasures. Oddly, eating isn’t much of a part of the NDE phenomenon.
Another NDE might have clouds. Some involve outer space, planets and galaxies. Despite the common threads, NDEs really are so different from one individual to the next.
Dr. Long continues, “My best guess as to why this is happening is that NDEs are an intersection with the infinite and eternal.
“It is quite possible that NDEs may be co-created to help the near-death experiencer learn what they need to learn to help them in their meaning earthly life.”
 As a leading NDE researcher and a medical doctor, Dr. Long has appeared on national media including NBC Today, ABC with Peter Jennings, the Dr. Oz Show, the History Channel, the Learning Channel and National Geographic.
As a leading NDE researcher and a medical doctor, Dr. Long has appeared on national media including NBC Today, ABC with Peter Jennings, the Dr. Oz Show, the History Channel, the Learning Channel and National Geographic.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Where Does the Soul Go During Cryonic Suspension?

If your soul goes to the afterlife at the start of your cryonic suspension, what happens if you’re thawed out and cured of your disease?
Let’s play around with this a little. Let’s just suppose that one day, cryonic suspension of humans is possible. In cryonic suspension, a person with an incurable terminal illness would be frozen.
When the cure is discovered, the patient would then be thawed out and given the cure, and resume life — even if this thawing occurred 200 years after the freezing began.
In cryonic suspension, the body, technically, is dead (no heartbeat).
So according to this, the patient has an NDE, if you believe that everyone who experiences cardiac arrest has an NDE.
However, a cryogenically preserved body doesn’t decay or decompose, so in that sense — true death doesn’t occur. The tissues are preserved.
So where is this person’s consciousness (astral self, spirit, soul) meanwhile? Does it hover in the “vestibule” between life here on Earth and life in Heaven?
You can’t freeze a soul. You can’t freeze your astral double or spirit…so it has to go somewhere during the suspension. But where?
Maybe you’re thinking, “There’s no point in speculating because we will never achieve this kind of technology in the first place.”
But you don’t know that. Go back to the Renaissance and tell the most brilliant minds of that time that one day, there will be heart transplants.
Tell them that one day doctors will take an unborn baby halfway out of the womb, surgically repair a defect, then put the baby back in to finish up its growth.
Tell them we’ll be able to clone dogs and cats. Tell them one day man will walk on the moon.
What seems impossible even in this day and age may actually one day be a reality, so don’t be quick to dismiss the possibility of cryogenic science — the ability to freeze people and then thaw them out and revive them.
You can’t compare this to what happens to a piece of steak that’s been in your freezer for 20 years.
That steak was not treated chemically or subjected to any kind of medical applications.
However, this all still begs the question:
Where does the soul go during cryonic suspension?
Would the patient have any kind of NDE? Does the patient actually cross over into the afterlife and exist as any deceased person would, in spirit form, doing things that spirits do?
And if so, then suppose 200 years later a cure for their disease is found. Does a spirit guide — or even God — inform that person, “They’ve found a cure for your disease; you have to go back”?
I posed this question to Jeffrey Long, MD, author of the New York Times Best Seller, “Evidence of the Afterlife: The Science of Near-Death Experiences.” Dr. Long is a radiation oncologist in Houma, Louisiana.
Dr. Long explains, “This is speculative, but my guess would be that their spirit would remain in existence even if their physical consciousness is dormant.
“NDEs point to a collective consciousness. The collective consciousness seems related to spirit or ‘soul.’ I think that this would operate the same way as people who are physically unconscious for a short period of time.”
For obvious reasons, there have never been any scientific studies regarding what would happen to the soul of a person who’s in cryogenic suspension.
But this topic is utterly fascinating and can drive an all-nighter of discussions.
As a leading NDE researcher and a medical doctor, Dr. Long has appeared on national media including NBC Today, ABC with Peter Jennings, the Dr. Oz Show, the History Channel, the Learning Channel and National Geographic.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

NDE’ers Being Told, “It’s Not Your Time” During CPR

During an NDE, are people told “It’s not your time” only when it seems that the doctors or EMTs won’t give up on the CPR?
A common theme in near-death experiences is that the individual is told, “It’s not your time; you must go back,” by either a deceased loved-one, spirits, angels or even God. It’s usually a deceased loved-one who makes this announcement.
Suppose Arista goes into cardiac arrest due to anaphylactic shock from the contrast dye that was injected into her for her MRA scan.
A crash cart is nearby and medical staff immediately begin resuscitation attempts. Arista has been down (clinically dead, heart stopped) for over 30 seconds.
She encounters her deceased grandmother in a brilliantly colored valley of incredible peace and joy. “It is not your time; you must go back.”
Somehow, Granny knows that the doctors are working furiously on getting Arista’s heart restarted and are willing to keep up their efforts for as long as it takes.
Arista decides to “go back,” and suddenly, the doctor sees a heartbeat. It’s as though the deceased loved-one knew this would happen. But what if Arista had decided, “No, I want to cross over”?
And she steps across the bridge. Would the doctors then suddenly say, “I give up, let’s call time of death”? (After all, this would match up with what happens to Arista during the NDE when she crosses the bridge.
Of course, it may also turn out that the doctors keep trying resuscitation for 40 minutes and then give up.)
Do you see what I’m getting at here?
Somehow, the deceased grannies, grandpas, parents, spouses, uncles and aunts know the difference between a woman whose heart stopped inside a hospital and one whose heart stopped at the hands of a violent boyfriend who strangled her in the woods.
Well, you know he’s not going to attempt CPR, so when that woman meets up with her deceased grandma—there won’t be any “It’s not your time; you must go back.”
My question is: Suppose in Arista’s case, she decides to go back…and just as she’s being flung backwards through the tunnel, towards her body…the doctor suddenly gives up hope and says, “Enough already; she’s gone; let’s call time of death”?
Will Arista suddenly find herself being yanked back through the tunnel towards Nana?
“That is a good question about the interplay of the choice of NDERs to return and the choice of those attempting to resuscitate them to either continue resuscitation or stop it,” says Jeffrey Long, MD, author of the New York Times bestseller, “Evidence of the Afterlife: The Science of Near-Death Experiences.” Dr. Long is a radiation oncologist in Houma, Louisiana.
Or, to put my question another way, suppose the doctors won’t give up the resuscitation attempts, and Arista, having decided to “go back,” is flying backwards through the tunnel, watching her grandmother’s form become smaller and smaller in the increasing distance.
Then suddenly…a gunman bursts into the room and shoots the doctors dead. Will Arista be yanked back to her grandmother?
Or will this yanking never occur because Nana already knew that the gunman would burst in and shoot everyone dead, and thus would have told Arista, “Welcome! Come with me to eternity!”?
Dr. Long continues, “My answer must be speculative, but my best guess is that the wise spiritual beings on the other side have the good sense of whether resuscitation will be continued or not.
“We have many NDERs were told, “It’s not your time,” were not being actively resuscitated by a medical team, or anyone else.
“Many NDERs who are aware that ‘It’s not your time’ have no other people around them.”
Wow. Does the spirit world know the future?
Why is there even a need for the spirit world to say, “It’s not your time?” if the future is already determined? Or isn’t it?
So it looks as though often, a person whose life-threatening situation is fuzzy (such as drowning in the presence of other people who can give CPR) gets to choose to “go back,” while someone whose life-threatening situation is more defined, such as having a massive heart attack when nobody is around — doesn’t get to choose — though there are cases like this in which the person came back from an NDE.
But let’s go a step further: The person is crushed beneath a car. We know that in that case, there will be no “It’s not your time.”
A compelling question is why are NDE’ers being told, “It’s not your time; you must go back,” if ultimately, God controls destiny? If the NDE’er controls it, then why does Gramps appear to tell him, “It’s not your time”?
What kind of NDEs did people who went into cardiac arrest 200 years ago have?
I’m talking people who had conditions that could have been remedied by CPR, but because CPR wasn’t around back then…these people certainly had a much different NDE—more like an ADE: actual death experience.
So it seems as though, to some extent, the choice to “go back” or not hinges on the presence of people who know CPR.
As a leading NDE researcher and a medical doctor, Dr. Long has appeared on national media including NBC Today, ABC with Peter Jennings, the Dr. Oz Show, the History Channel, the Learning Channel and National Geographic.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

NDE’ers Told They’d Come Back in a Vegetative State?

Ever wonder what kind of near-death experience that a person in a persistent vegetative state had?
Thousands of people have reported NDEs during the time their heart was stopped and brain not receiving blood flow and oxygen.
Often, these individuals are faced with choosing between crossing some threshold (beyond which they won’t be able to “return” to their body), or “going back” to their body.
In other cases, they want to cross over, but are “forced” back into their body. Many are shown, while having the NDE, snippets of what their future holds. This may include an arduous medical recovery.
Obviously, none of these NDE’ers came back as vegetables. However…just what kind of NDE does someone who ends up in a permanent vegetative state have?
Let’s assume that cardiac arrest (regardless of cause) results in what we know as the near-death experience.
This means we can assume that Terri Schiavo and Nancy Cruzan both had the same NDE (as far as common themes) as did any one of the NDE’ers who have shared their story on nderf.org — a site created by NDE researcher Jeffrey Long, MD, author of the New York Times bestseller, “Evidence of the Afterlife: The Science of Near-Death Experiences.”
Dr. Long is a radiation oncologist in Houma, Louisiana.
Schiavo and Cruzan lived for years in a persistent vegetative state before dying. Quinlan lived for nine years in an irreversible coma before dying, though some reports say persistent vegetative state.
One has to wonder: Were these three individuals, along with the hundreds of thousands of other people who live as vegetables or in irreversible comas, told during their NDE that they’d be returning to their bodies as a vegetable?
Were they told, “It’s not your time; you must go back, but you will be in a permanent vegetative state”? Or were they only told, “It’s not your time; you must go back”?
And then they felt themselves going “back,” having no idea what was in store?
Or perhaps some of them tried to cross over after being told of their fate, but were “forced” back through the tunnel.
Maybe some had no idea what fate awaited them back in their bodies, but tried to cross over anyways.
Were NDE’ers who came back as vegetables okay with the news from spirits, angels or deceased loved-ones that they’d be coming back as a vegetable? Here’s what Dr. Long says:
“When someone is told, ‘You can cross over or you can go back; the choice is yours.’ we cannot assume that they were informed that they would be in a vegetative state.
Many NDE’ers who are given a choice to cross over or return are shown a future vision of their earthly life if they choose to return.
“They may be shown how difficult the recovery is from their life-threatening event. They may also be shown how difficult the future life will be.
“It is possible that some people having an NDE knew they would return in a vegetative state and chose to do so.
“Since this group of people cannot communicate well (or at all), it may be difficult to know this for sure. We can only understand NDE from people who return and are able to adequately communicate the experience.
“We simply don’t know about the experience of those in a vegetative state, although my best guess is that they have NDEs similar to all others, and I suspect many are aware that they would return in a vegetative state, but understand that there are important reasons for them to do so. This is speculative.”
One More Thing to Consider About NDE’ers Who Return As Vegetables

Shutterstock/CandyBox Images
A common thread among NDEs is the absence of time perception. Time stops. Time is endless. Time doesn’t exist.
Suppose a person is told, “If you go back, you will be a vegetable.” But that person has also learned, via near-death experience, that in the grand scheme of things, living out the rest of their life in a vegetative state will serve a significant purpose.
Knowing this, and also knowing that one day they will indeed cross over the “barrier” to the eternal paradise, this individual welcomes returning as a vegetable.
Now here’s something very riveting to consider: From a family member’s point of view, this individual’s vegetative state (or permanent coma) is harrowing. But from the patient’s point of view…it may seem like only moments passed.
Suppose they go “back” to their body and live another 20 years in a vegetative state. Then they die for good. That’s 20 years.
But from THEIR point of view, since they had NO awareness during that 20 years…it will seem like only seconds passed—and before they know it—they are once again seeing the brilliant light and deceased loved-ones welcoming them to cross over for eternity. Thus, the decision to return as a vegetable would be quite easy.
But this begs a question: What about vegetative people who, years later, briefly come out of this state and have awareness?
There are a few cases in which a person who was in a PVS for years mysteriously popped out of it enough to speak with family members, then slipped back into it and never aroused again or aroused only a few more times, then died.
Well, from their point of view, time passage between their first NDE and actual death 25 years later, with one or two episodes of, say, five weeks of consciousness in between, would seem like only the time passage of those five weeks of consciousness.
But then what about those individuals who come back from an NDE as vegetables—but after years like this—exhibit signs that all along, they’ve been aware?
Functional MRI brain scans have shown “lit up” areas of the thinking part of the brain in several such patients, suggesting that these patients can hear and have full consciousness—but no way to communicate—not even by squeezing their eyes shut.
And if that’s confounding, what about people who, after cardiac arrest (and presumably an NDE), come back to live for years in a minimally conscious state?
As a leading NDE researcher and a medical doctor, Dr. Long has appeared on national media including NBC Today, ABC with Peter Jennings, the Dr. Oz Show, the History Channel, the Learning Channel and National Geographic.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sources: en.wikipedia.org/wiki/Cruzan_v._Director,_Missouri_Department_of_Health en.wikipedia.org/wiki/Terri_Schiavo_case nature.com/news/neuroscience-the-mind-reader-1.10816
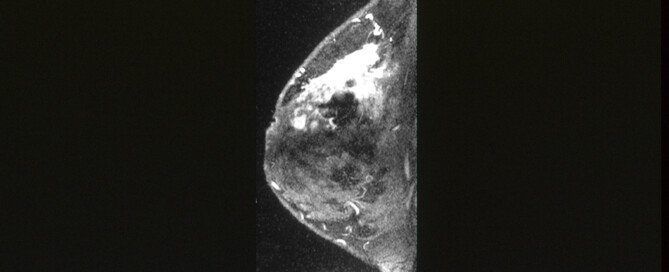
Natural Cancer Cure: Woman Who Cured Breast Cancer with Vegan Diet
Ever wonder if a natural cancer cure might exist? Such as in the form of diet?
Breast cancer survivor Ruth Heidrich believes so.
She was diagnosed with metastatic breast cancer 35+ years ago at the age of 47.
Heidrich had refused chemotherapy and radiation, despite bone scans showing that the breast cancer had spread to both femur (thigh) bones and pelvis. An X-ray revealed the cancer was also in one of her lungs.
This interview is strictly meant to accurately present what Heidrich told me; hence, this post falls under the category of interview, not medical advice.)
Ruth Heidrich discovered a lump in her breast during a breast self-exam. Cancer was confirmed after a physician performed an excisional biopsy (surgery).
Prognosis?
It was so serious that I got second, third and fourth opinions. No doctor could tell me if I had three months, three years, or what. The oncologists all recommended chemo, radiation and tamoxifen.
Before diagnosis, what were your eating habits?
I thought that, since I had studied nutrition during college, I was eating the healthiest diet possible, although it was actually sad: the Standard American Diet.
I had virtually cut out red meat, increasing my fish and chicken intake to compensate for the animal protein which I mistakenly thought was needed, and drank a lot of powdered skim milk, again, mistakenly thinking this would make my bones strong.
Actually, as scientific studies show, animal products are not any healthier at all, and in fact were most probably the cause of my breast cancer!
Why did you shun chemotherapy?
Two weeks after my cancer diagnosis, I spotted an announcement in the newspaper, which was for a clinical research study to investigate the validity of the low-fat vegan diet versus standard chemo/radiation to reverse cancer.
I literally ran to the phone and found myself speaking to the study’s head researcher, John McDougall, MD.
When I got to his office, he showed me the bleak results of conventional medical treatment, and I then decided to enroll.
This study involved what?
I had to agree to switch my diet to low-fat vegan, that is, 100% plant foods. This meant no animal foods at all and no added oils.
I went home and began this diet within two weeks from the biopsy with its horrible diagnosis.)
Did you inform the doctor who diagnosed you what your plans were?
Yes, and he just shook his head in disgust, saying that “Diet has nothing to do with breast cancer.” I knew better because I had seen the scientific studies demonstrating otherwise.
After you started this diet, how much time went by before you returned to the diagnosing doctor to check if the cancer still was there?
It was a matter of just weeks. The initial bone scan with the “hot spots” was two weeks following diagnosis.
A month later, those “hot spots” had significantly receded, and within three months, they were completely gone.
The chest X-rays, however, to this day still show the encapsulated tumor that’s in my left lung; it hasn’t grown in 25 years.
How was the cancer in your breast determined to be gone?
After that first biopsy revealed no clear margins (they hadn’t gotten all the cancer), I had more surgery. (the excisional biopsy was an attempt to get the whole thing out.
A modified radical mastectomy was determined to be needed because the cancer had also spread throughout the breast as well as the bones and lung. realize, it’s not cancer in breast tissue that kills you — it’s cancer cells that metastasize to vital organs, usually the bones, LIVER, lungs, and brain. All of the follow-up tests continue to show no recurrence of the cancer.
When the bone cancer disappeared, how did the physicians react?
They had no explanation for how this happened and told me that my new diet couldn’t have any effect on the spread of the cancer, that I was taking a risk in continuing to refuse chemo and radiation.
Using a layperson’s perspective, explain why the cancer doctors did NOT get excited about your situation and did not tell their colleagues.
All MDs go through fairly standard training and are usually taught that diet does not cause cancer, and therefore, certainly can’t cure or reverse it, that only chemo, radiation, or hormone manipulation can treat it.
Of course, the pharmaceutical companies stand by, always ready to supply the chemo and hormone blockers. A physician who “dares” try anything different, such as dietary manipulation only, violates a code or “community standard of practice.”
Therefore, even if an MD believes it could work, he or she takes a big risk in going against conventional medical protocols.
Another factor to consider, and I’m sure that Dr. McDougall will agree with, is that MDs and drug companies will not make any profit treating cancer this way. Actually, I think our health care industry would dissolve if people went vegan!
Do you stand to get any financial gain by fabricating any of this?
I don’t have anything to gain financially — fact is, I’ve invested a great deal of energy, time, and gas, visiting cancer patients, giving talks, getting on the radio, and writing books — all to little or no avail.
Ever considered submitting your medical documentation to various medical or cancer organizations?
If even physicians like John McDougall, Michael Klaper, Neal Barnard, Michael Greger, Terry Shintani, and more., and even one of the most widely respected nutrition scientists in the world, T. Colin Campbell, PhD, can’t convince them, I myself really don’t stand much of a chance.
I’ve also approached the Susan G. Komen Foundation and American Cancer Society, and got nowhere because they rely on the mainstream medical approach.
**********
A point to consider: Technically, a vegan is someone who avoids all animal-derived foods, but doing such doesn’t always mean a healthy diet, if this “vegan” consumes a lot of sugar, processed refined food, additives, preservatives and artificial sweeteners.
Heidrich has to her credit more than 900 trophies from multitudes of athletic competitions, including Ironman Triathlons, Half Ironmans, and dozens of marathons and ultra-marathons.
She has won eight gold medals from state and national level Senior Olympics, and is the author of three books.
“Ms. Heidrich’s story illustrates the importance of nutrition when fighting cancer,” says Jonathan Stegall, MD, an integrative oncologist and medical director for The Center for Advanced Medicine, an adult cancer treatment center in Alpharetta, GA.
“We have a significant amount of research showing that nutrition is important for patients with cancer as well as for those who want to prevent cancer.
“There are other stories of patients who have beaten cancer relying mostly or exclusively on nutrition.
“However, it is important to note that these patients are very rare. So while I acknowledge that it’s possible to cure cancer with diet alone, it isn’t very likely.
“Consider someone who wants to accumulate wealth. One way to do that is to buy a lottery ticket.
“Some people have gotten rich by winning the lottery, so it’s possible – but it isn’t likely.
“In fact, it’s a poor choice for accumulating wealth, since there are many other approaches which have proven to be more effective.
“Similarly, solely relying on nutrition to beat cancer is a poor choice, since we have many other treatments which have been shown to be more effective.
“I share Ms. Heidrich’s passion for nutrition, and believe that it is a very important aspect of cancer treatment.
“For example, I put all of my patients on a plant-based eating plan, and provide recipes as well as advice on fasting.
“But I also want to caution people that as important as nutrition is, it should never be the focus of their cancer treatment plan.
“This is where integrative oncology really shines, where we strategically combine conventional treatments such as surgery, chemotherapy and radiation with evidence-based natural therapies such as nutrition, supplementation, stress reduction therapies, lymphatic therapy, mistletoe, etc.”
Ruth E. Heidrich
RuthHeidrich.com
Author of “CHEF,” “A Race for Life,” and “Senior Fitness”
 Jonathan Stegall, MD, provides a long-awaited remedy for our cancer problem. Having a successful integrative oncology practice in Atlanta, GA, he’s seen firsthand what works and what doesn’t with cancer treatment. Dr. Stegall is the creator of the Cancer Secrets Podcast and author of “Cancer Secrets,” available on Amazon.
Jonathan Stegall, MD, provides a long-awaited remedy for our cancer problem. Having a successful integrative oncology practice in Atlanta, GA, he’s seen firsthand what works and what doesn’t with cancer treatment. Dr. Stegall is the creator of the Cancer Secrets Podcast and author of “Cancer Secrets,” available on Amazon.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: cancer.gov
Look Tall with Shoe Lifts: Review of Inserts

There are many shoe lifts out there, but which truly work best for making you taller?
Many people want to be tall or taller. It’s no secret that many men, and women, wish to be taller; especially men.
Women easily achieve this with high heeled women’s shoes, but men don’t have this option for appearing tall with men’s shoes — unless they insert shoe lifts. Though some men’s shoes come with built-in shoe lifts.
Shoe lifts will create the illusion you are taller without it showing, as in high heels. Some shoe lifts slip right in the shoe, while others have an adhesive.
A lot of men and women do wish to be taller; even some tall people would like a little more height. Being tall has been proven to be a great asset in the business world, and an extra inch can make a difference.
I ordered three pairs and got a fourth pair free: one quarter inch, one inch, one and a quarter inch, and then the free one at one and a half inch.
I recently purchased shoe lifts online (Canfield Plastics), even though I am considered tall, at 5-8. I’d rather appear to be a natural 5-9 if I can accomplish this with shoe lifts inside my sneakers.
Some shoe lift companies offer deals where you save by buying three shoe lifts at a time, and the shoe lift heights range from one-quarter inch to two inches or slightly more than two inches.
The quarter inch was for my four-inch heel pump shoes, but these are generic shoe lifts and thus they do not fit into the women’s shoe pump design.
The inch and a half shoe lifts were for my dress boots, but with the shoe lift inside the boot, I am unable to zip the boot up.
An inch and a half may not seem like a lot, but this is too high for a regular shoe or sneaker; your heel will be practically sticking out of the shoe and every time you walk, you’ll struggle to keep the shoe on. It will also be obvious you have a shoe lift.
I can zip my boots up with the inch and a quarter lift.
And the inch lift go inside my sneakers. The inch and a quarter leave my heel more noticeable than it should be, and it feels like the sneaker will slip off with each step.
They are comfortable; not hard as wood, but not soft enough to lose height from your body weight. So if you wish to be taller, buy shoe lifts. They aren’t cheap, either, but investigate the various package deals.
If you’re wondering why a 5-8 woman would want shoe lifts, I’ve always wanted to be taller.
In fact, why does ANY woman wear high heels? Certainly not for comfort. It’s for fashion and looks, and being taller is a part of that for many women.
Many stylish women’s shoes just happen to have a 3 or 4 inch heel, but some high heeled women’s shoes are also very plain looking, so when women buy these, one has to believe that often, it’s because the woman wants to look taller.
But the increased height looks artificial because the heels are visible. A shoe lift solves this problem, though the lift height is limited.
A woman, even at 5-8, who wants to appear taller and thus uses shoe lifts, is operating under the same mindset as a woman who colors her hair, wears artificial long nails, spends 20 minutes applying eyeliner and mascara to each eye, paints her lips an artificial color, puts extensions in her hair, etc.
It’s all about fashion accessories, and shoe lifts can be part of this.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Why Thin Heart Attack Survivors Have Higher Mortality Risk

A report says that lean people have an increased risk of death five years after a heart attack, but there’s a flaw in this report.
So if you’re plus size, don’t rejoice just yet.
Plus size or not, you may be stunned to learn about the findings that were presented at the ESC Congress 2013 by French researchers, that lean heart attack survivors (along with very obese and those with disproportionately big bellies) are at increased risk of mortality five years out.
The term “lean” is misleadingly used in the French study. Perhaps “skinny-fat” should have been used instead.
Heart Attack Mortality Risk in Skinny-Fat Survivors vs. Lean Survivors
The paper states that both lean subjects and very obese ones had an increased risk of death after five years.
In addition, high waist girth, severe obesity and also underweight were associated with the biggest risk of death in those who’d had a heart attack.
These results are based on BMI (body mass index) calculations as well as waist circumference.
The paper had actually used the term “underweight,” not just “lean.”
To fitness professionals, the term “lean” is NOT the same as “underweight,” “slender,” “thin” or “skinny.”
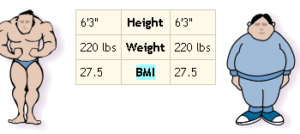
In fact, a man who stands 5-9 and weighs 220 pounds could actually be very lean!
And a woman who wears a size 6 can actually have excess visceral fat (fat around the vital organs including the heart)!
The Problem with BMI
BMI is a value that results from a calculation involving one’s height and weight. Period.
BMI does not reveal body composition. It’s quite fair for me to wonder, then, if those “lean” heart attack survivors with that increased mortality risk had the so-called skinny-fat bodies.
A skinny-fat person appears “lean,” slender, lanky or thin in terms of size, but their body composition tells a different story.

Shutterstock/Sorn340 Images
If a personal trainer were to take a caliper skin-fold reading of a skinny-fat person to determine body fat percentage, the result would likely be a number in the “acceptable” range.
But according to the American Council on Exercise, the “acceptable” range for women is 25 to 31 percent, and for men it’s 18-24 percent.
If a person who appears slim, lanky or underweight has a body fat percentage in these ranges (gender considering), they will appear soft or flabby, despite being able to wear a size 6 or 8 dress or a slim-fit suit.
What body fat percentage would indicate “lean,” in the true sense of the word, according to ACE?
For women, 14-20 percent, and for men, 6-13 percent. Though a person who’s literally starved (such as from anorexia nervosa) will have an exceedingly low body fat percentage, they’ll also have an exceedingly low amount of muscle.
A lean person who works out and eats healthy, however, will have plentiful muscle mass while having low body fat. They are healthy-fit lean, not skinny-fat.
This is why BMI is worthless to athletes, especially physique specialists and bodybuilders. Their BMIs are often in the “overweight” range, yet their body fat percentages are very low.
I’d love to know what the body fat percentages and muscle volume levels were of those “lean” heart attack survivors in Professor Simon’s study.
Another striking point to consider is just how “lean” or “underweight” those smaller study subjects were, AND if maybe they had underlying medical conditions (which could shorten lifespan) that somehow caused the underweight.
I do not believe these heart attack survivors’ body compositions were comparable to those of athletes and physique specialists, even though dress-size-wise or suit-size wise, they can be interchangeable with athletes and physique enthusiasts.
If BMI is so misleading, why is it used in heart attack research?
Because it’s super easy! Often, research involves investigating and tracking up to hundreds of thousands of people.
Imagine the hairy logistics involved in getting a skin-fold reading on every one of them!
On the other hand, to get the BMI, all the researchers need do is get the patient’s height and weight from medical records. How easy is that?
When medical researchers use the word “lean,” consider the possibility that what they’re referring to is dress or suit size rather than body composition.
Having higher levels of body fat, even if the person has a slender frame, increases risk of health ailments including cardiac-related.
Hopefully, you now know why thinner heart attack survivors were found to have an increased risk of five-year mortality.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}