

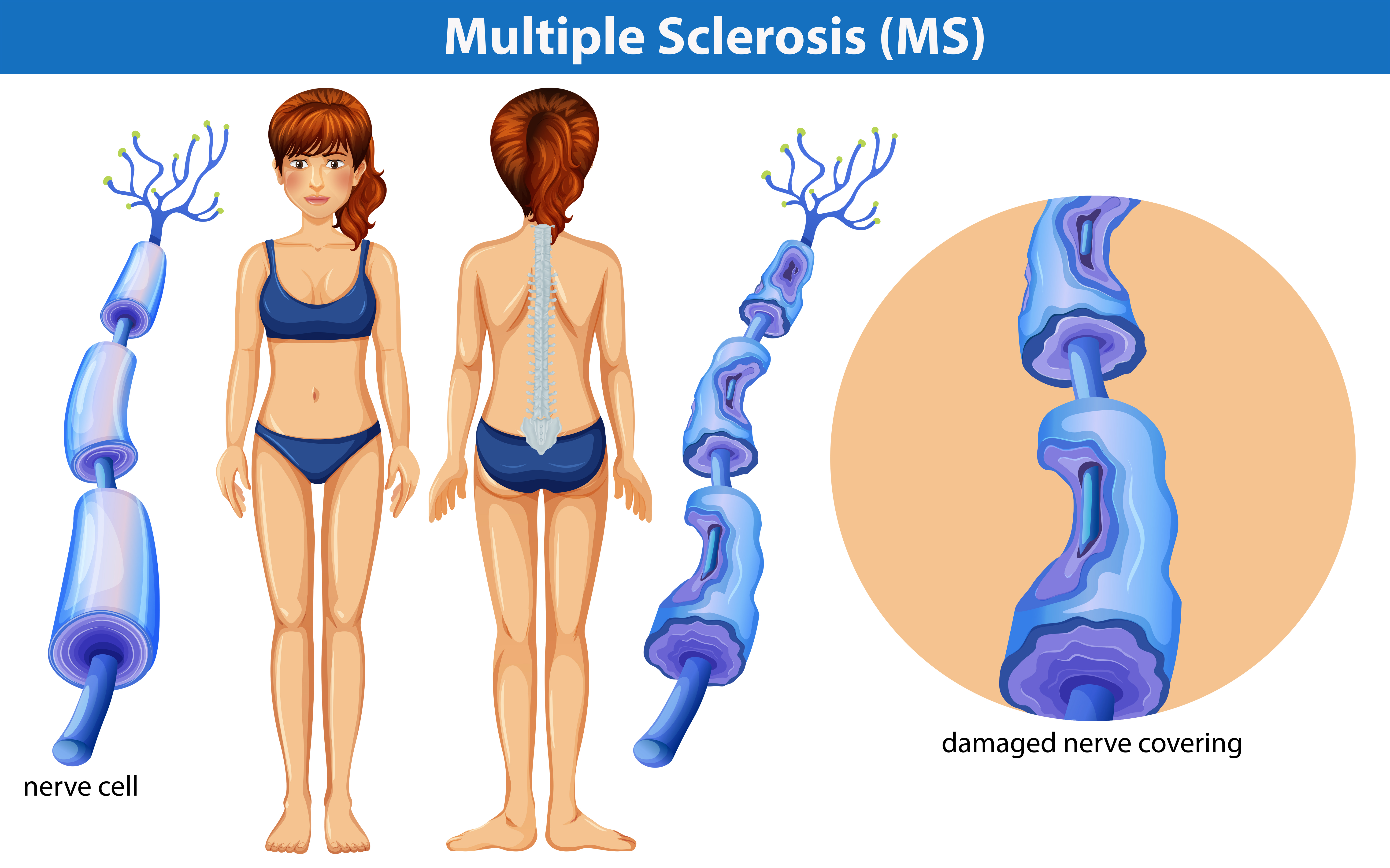
Can Twitching Muscles Be an Early Sign of MS?

Many people wonder if twitching muscles might be an early symptom of multiple sclerosis.
Multiple sclerosis is an autoimmune disease that can render a person bedridden and comes with an assortment of possible symptoms.
“Twitching per se is not a common MS symptom and is not considered an early sign of MS,” says Karen M. Blitz-Shabbir, DO, a neuro-rehabilitation and multiple sclerosis specialist based in Islip, NY.
“Some symptoms that warrant investigation or consult with a neurologist include weakness, tingling, numbness, tremors.”
When I say “twitching,” I’m referring to fasciculations, or the kind of twitching that occurs in perhaps millions of eyelids every day.
These same kind of fasciculations also commonly occur in the legs, particularly after heavy exercise or activities like a long hike or hard time spent on cardio equipment.
People usually become aware of their twitching muscles when they are at rest, such as at a computer or when watching TV.
Somehow, some way, they come up with the idea that multiple sclerosis often, or just sometimes, starts out with these kinds of muscle twitches.
If you’re still worried that your muscle twitching signals an early symptom of MS, then here are the limb/muscle-related symptoms of this neurological disease (no particular order):
Weakness or numbness in at least one limb. Typically this happens on one side of the body at a time.
(Weakness and numbness are not to be confused with twitching muscles, and keep in mind that many, many conditions can cause numbness and especially weakness.)
Tremors. A tremor is not the same as a fasciculation-type muscle twitch. A tremor is a kind of shaking or trembling.
Tingling or pain in portions of the body, and/or fatigue that can’t be explained away by exercise, stress or side effects of a medication.
 Dr. Blitz-Shabbir is also the medical director of rehabilitation with Holy Name Medical Center MS Center.
Dr. Blitz-Shabbir is also the medical director of rehabilitation with Holy Name Medical Center MS Center.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: vecteezy.com
Source: mayoclinic.org/diseases-conditions/multiple-sclerosis/basics/symptoms/con-20026689

“My Giant Life”: Super Tall Women Nothing to Feel Sorry For

We all have struggles, and many people wish their biggest problems were finding jeans that are long enough and trying to squeeze into an airplane seat.
Meanwhile, I’ve always wished I were six feet, and envy women who are even taller than this (though my preferred height isn’t exactly “giant” caliber, yet at the same time—a little bit of me envies the women of “My Giant Life.” I don’t feel sorry for these super Amazons, especially since two play my sport, volleyball).
TLC’s “My Giant Life” focuses on four women ranging from 6-6 to 6-9, though one of the “women” is actually a 16-year-old girl who, at 6-6, may still grow another several inches.
“My Giant Life” is sure to be a hit show. What’s always stunned me is how women who are only (yes, “only”) 5-9 can feel self-conscious about their height.
I don’t get this. I was at the gym today. Even though I’m 5-8, I was dwarfed by one man after another in the free weight area. I don’t mean by muscle size, but by height.
So if a woman is 5-9, even close to six feet…she wouldn’t exactly stand out—at least not from where I come from.
And by the way, if someone asks if you play basketball because you’re so tall, don’t be a schmuck and ask them if they play miniature golf.
This is as old as the hills, and if it ever was a clever come-back, it certainly lost that zing decades ago. Be a good sport and give an honest answer.
If someone comments, “Gee, you’re so tall,” don’t be snarky by saying something like, “Oh, thank you for pointing that out; I had no idea!” After all, even very tall women are capable (as is the rest of the population) of pointing out the very obvious.
If you’re blessed with generous height, have you never pointed out the obvious before? Perhaps you commented to a stranger in the supermarket line with her preschooler, “Wow, your daughter has such curly hair!”
Chances are, you’ve said the following to at least a dozen women: “Oh, you’re so thin!”
Maybe you’ve said to someone in the park or on the sidewalk in your neighborhood, “Gee, your dog is huge!”
These are all examples of pointing out the obvious. Here’s another one that you may be guilty of: “Wow, your eyes are so blue!”
Yes, it could get very annoying, but that’s no reason for being a schmuckaroo. After watching “My Giant Life,” you’ll have a new perspective on your height.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Muscle Twitching: Is It ALS, Anxiety or BFS? Best Information!

Do twitching muscles have you terrified of ALS?
Then you need tons of reassurance, and I have it for you: a collection of the best muscle twitching articles that cover everything imaginable to help you through your ALS panic, fear, anxiety and sleepless nights.
This superb collection of muscle twitching articles was written by me, based on my own experience with a brief bout of muscle twitching fear that was brought on after I googled the wrong words and ended up reading some scary information on an ALS site.
The articles INCLUDE STATEMENTS FROM DOCTORS WHOM I INTERVIEWED.
Because I’m a writer by profession, I decided to write all about muscle twitching, benign fasciculation syndrome (BFS) and the accompanying ALS anxiety and panic.
Muscle twitching is technically known as benign fasciculation syndrome (BFS) if the twitching is accompanied by other symptoms such as tingling, cramping and soreness.
Twitching muscles, in isolation, are known as fasciculations. These fasciculations are not to be confused with restless leg syndrome, even though some types of muscle twitching can be described as “creepy crawlies” under the skin.
Everyone experiences muscle twitching, by the way. The difference between the people who are consumed with fear they have deadly ALS, and everyone else, is that, by sheer freak chance, on a bad day, the people in the first group googled “twitching muscles” or something similar, and found themselves glued to an ALS site.
The ensuing fear of having ALS can happen to just about anybody.
You CAN overcome it!
Read every one of my well-organized articles to help with your recovery. You will be so very reassured.
And if you have relapses, each will be less disastrous than the last, until eventually, relapses last only for 10 minutes, until finally, you’ll no longer have them!
I’ve reached a point where I just LOVE the feel of muscle twitching in my right hamstring, because one of the muscles has a slow-healing, running-related injury.
The “fascs” literally give it relief and feel like a mini-massage.
Any time you need reassurance that you don’t have ALS, refer to the information below for the specific assurance you seek.
You can once and for all conquer your fear of a disease that’s very rare.
Anxiety over having the beginning signs of ALS can be overwhelming, especially if you’re not sure how to visually identify atrophy of the muscles.
Another source of anxiety is that of twitching occurring in the same spot over and over and over.
This often involves an eyelid, but it can also involve a lip or an area near the lip, somewhere on the quadriceps (front of the thigh), the hamstring area (back of the thigh), and a thumb or calve.
A particular area that has many men and women scared out of their wits is their tongue.
Have you gone down a rabbit hole of fixation over your tongue, examining it througout the day?
Do you stop at every mirror you ever pass to inspect your tongue?
Do you try to hold it as still as possible but still see it twitching?
Does chewing food seem a bit difficult lately? How about forming words?
Are you constantly worrying that you have the bulbar form of ALS? Here is some reassuring information that you can really use!
The Thigh Dent
Here is yet another specific area of fear that some people have.
Somehow, someway, an individual has become overly focused on what appears to be a dent or indent in one of their upper legs.
It could be on the front or the side, and what’s alarming is that something similar is not on the other leg.
This is one of the most frightening symptoms for anyone who’s in the throes of ALS anxiety.
Knowledge of the facts is an unbelievable weapon against this type of anxiety.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Chest Pain, Swallowing Hurts: Heart Attack or Esophagus Spasm?

Chest pain with painful swallowing can mean a number of things including heart attack in progress, heart attack in the near future and benign esophageal spasms.
About 200,000 people in the U.S. every year suffer from some kind of non-cardiac chest pain that may be accompanied by other symptoms like discomfort swallowing.
Dr. Ron Schey, a gastroenterologist at Temple University Hospital, recommends a specific treatment for chest pain that results from an issue with the esophagus rather than the heart: dronabinol.
Dronabinol is a drug that historically has been used for nausea and vomiting that result from chemotherapy.
Dr. Schey had a small group of people with non-cardiac chest pain (which can mimic a heart attack and cause severe anxiety) take five mg of dronabinol two times a day for four weeks, while other patients took a placebo.
Those on the dronabinol did better with tolerating their chest pain, and it was less intense and less frequent. Plus, there were no notable side effects.
Because this study was small, it’s not possible to compare how this drug works for non-cardiac chest pain vs. the current therapies.
Dr. Schey explains in his study report that dronabinol likely works by activating cannabinoid receptors in one’s esophagus, thereby reducing sensitivity. A larger-scale study is planned.
If you’ve been experiencing chest pain, even if there is some kind of difficulty or discomfort with swallowing, you should get a thorough evaluation at the ER to rule out a heart attack (a blood test will do this).
However…the blood test (which checks for leakage from damaged cardiac muscle of an enzyme called troponin) does NOT detect the presence or absence of clogged arteries!
“Troponin is a protein in the heart involved with contraction and relaxation of the heart muscle,” says Jack Wolfson, DO, FACC, a practicing cardiologist in Arizona, author of The Paleo Cardiologist: The Natural Way to Heart Health.
He continues: “If troponin is elevated, it is a sign of heart muscle damage. This is obviously not a good thing.
“But millions of people are walking around with extensive blockages, yet troponin is normal if checked.
“Again, elevated troponin is a sign that you may be having a heart attack.”
“Thus, if this blood test comes out negative, you should then follow up with your cardiologist.
“If all is fine, then the next step might be with a gastroenterologist to see if there’s an issue with your esophagus (which could be a spasm or acid reflux, among other issues) that’s causing the chest symptom.”
 Wolfson Integrative Cardiology specializes in functional medicine and provides treatment plans for out-of-town patients.
Wolfson Integrative Cardiology specializes in functional medicine and provides treatment plans for out-of-town patients.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/ShotPrime Studio
Source: sciencedaily.com/releases/2014/10/141021135018.htm

How Many Whole Eggs Are Safe to Eat Per Day?
A cardiologist explains how many whole eggs you can confidently eat in a single day.
Is it unhealthy to eat five whole eggs a day? Bodybuilders swear by eating lots of whole eggs, but what about cardiologists? Can too many whole eggs a day raise your bad cholesterol numbers?
“Eggs are one of nature’s perfect foods,” says Jack Wolfson, DO, FACC, a practicing cardiologist in Arizona, author of The Paleo Cardiologist: The Natural Way to Heart Health.
“It is like a multivitamin, containing everything a chicken needs to come to life,” continues Dr. Wolfson. “Hundreds of studies have proven eggs to be safe. In fact, eggs raise the beneficial HDL cholesterol.” HDL stands for high density lipoproteins.
Dr. Wolfson continues, “Eggs were vilified for many years because they contain cholesterol. But humans need cholesterol and it is beneficial to consume it. Times are changing, but many hospitals and doctors do not allow eggs for cardiac patients.”
This is so true. After my mother had her heart bypass surgery, I noticed that she was barred from ordering real eggs off the hospital menu.
The dietary staff knew which orders were being called in from the cardiac unit. Cardiac patients were permitted only the “Egg Beaters” type eggs—which actually is a synthetic goop that (in my opinion) hardly tastes like the real thing.
Hospitals, says Dr. Wolfson, instead serve pancakes with sugar-free syrup. “This is the source of the problem, and this lack of understanding keeps people coming back for more stents and surgeries.”
Pancakes are loaded with refined carbohydrates. These promote inflammation throughout the body and in the coronary arteries.
The body responds to this inflammation by building plaque in the arteries. The onslaught of sugars erode the inner wall of the coronary arteries. In simple terms, think of the repair process as the body shellacking these erosions—the shellac being plaque buildup!
“I recommend rotating foods, so every 3-4 days I will have 3-4 eggs as an omelet, scramble, egg salad and even raw. I always add plenty of herbs and spices when cooking to counteract any damage from cooking the eggs.
“Boiling eggs would not have a much oxidative damage from the heating process. And don’t forget, all of the nutrition is in the yolk.
“Those who order egg-whites only are depriving their body of precious nutrients and may actually be causing harm from doing something so unnatural.”
So back to the original question: How many whole eggs can you eat every day, then, since the cholesterol in them isn’t what actually harms the heart?
Dr. Wolfson explains, “A dozen eggs per week is not a problem according to most published studies. Therefore, 3-4 eggs per day however you like to prepare them is not a problem.
To avoid developing a sensitivity or allergy, I recommend eating eggs only 3-4 days per week at most.”
So there you have it: Enjoy your king-sized omelets (but spare the white flour and add in more vegetables like onions, peppers, mushrooms and spinach. Add in chopped walnuts for a unique addition of flavor and boost of nutrition.)
Wolfson Integrative Cardiology specializes in functional medicine and provides treatment plans for out-of-town patients.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Heart Palpitations During, After Eating: 6 Causes

“Many patients note heart palpitations after meals,” says Chester M. Hedgepeth, III, MD, PhD, Executive Chief of Cardiology at Care New England.
“The most common reason for this is dietary caffeine intake during mealtime which is found in many drinks, including coffee, tea, soda, and energy drinks and chocolate.
“Alcohol consumption during mealtime, especially if in moderate of high levels, can be associated with heart palpitations.”
Dr. Hedgepeth further explains, “Some patients may also have sensitivity to a particular food, or food additive like monosodium glutamate (MSG).
“Heartburn caused by eating spicy or rich foods can lead to heart palpitations.
“If you have heart palpitations after eating, it may not be directly related to the food but to the mealtime experience.
“Palpitations can be triggered by the simple act of swallowing, or if your mealtimes are a source of anxiety or stress.”
That last point is very compelling. For many people, mealtimes are a time of stress.
If you’ve been experiencing heart palpitations while you eat or “from” eating…take note of the conversation and emotions that take place during the meal.
Do arguments usually ensue?
Do the discussions revolve around stressful topics such as budgeting and saving money, negative experiences at the workplace or the in-laws’ upcoming visit?
Of course, if you have heart palpitations while eating alone, you may still want to assess your thought processes during this time.
When you eat by yourself, is this also the time that you worry about all sorts of things?
Can heart palpitations after eating mean anything bad?
“Usually, the palpitations after mealtime are not associated with any pathology and resolve on their own,” says Dr. Hedgepeth.
“Rarely, these palpitations can be associated with a cardiac arrhythmia.
“Progressive palpitations which are increasing in duration or which are associated with chest pain, shortness of breath or fainting should be evaluated by a physician.”
Preventing Palpitations “from” Eating
“The key to preventing the symptoms is to try identifying what the trigger is for them to occur,” says Dr. Hedgepeth.
“Certainly, reducing caffeine and alcohol intake will help prevent mealtime associated palpitations.
“Also, eliminating foods for which the patient may have a sensitivity or which contain additives (e.g., MSG) may help.”
MSG (monosodium glutamate, common in processed and restaurant foods) is a sodium salt, and consuming it in large amounts will contribute to increased sodium intake.
High sodium levels can affect blood pressure and heart rate, potentially leading to palpitations in sensitive individuals.
 Dr. Hedgepeth also serves as a physician in the cardiovascular division and arrhythmia service at Brigham and Women’s Hospital, plus is an instructor of medicine at Harvard Medical School.
Dr. Hedgepeth also serves as a physician in the cardiovascular division and arrhythmia service at Brigham and Women’s Hospital, plus is an instructor of medicine at Harvard Medical School.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Monster e

Acid Reflux: Chest Tightness vs. Angina, Heart Attack

Acid reflux or GERD can cause chest tightness, but how does this compare to that caused by a heart attack or angina?
“GERD is a disease where the esophagus is exposed to abnormal amounts of acid which is not designed to tolerate,” explains Jay Desai, MD.
Dr. Desai specializes in colon cancer screening, upper endoscopy and consultative gastroenterology with New York Gastroenterology Associates.
“The most common symptom is a burning sensation in the chest, which can also manifest as a tightening sensation.”
This sensation of tightness in the chest would, understandably, be quite frightening to anyone who knows that “tightness in the chest” is typically listed as a symptom of heart trouble, particularly that of a heart attack.
Dr. Desai continues, “It is important to note that this is just a symptom; the chest does not actually physically tighten.
“GERD symptoms can be confused with a cardiovascular event. Patients who are at risk for cardiovascular disease, i.e., people over age 50, tobacco smokers and those with family history of heart disease, should be evaluated for heart disease if they have these symptoms.
“If cardiovascular disease is ruled out, a trial of antacid medication should be initiated to see if it improves symptoms.”

A wedge pillow for acid reflux
GERD can also occur overnight or even shortly after going to bed.
What works for many people is that of elevating the upper body with a wedge pillow (one style is shown above), to help keep the stomach acids from creeping up the esophagus.
There are different styles of wedge pillows, and you may have to experiment with several before finding the one that’s the most comfortable for your sleeping habits.
You may also want to consider sleeping in a recliner chair.
Mattresses have not been proven to be the best sleeping surface for every single individual, and their horizontal shape is the last thing that someone with overnight acid reflux needs.

Board certified in internal medicine and gastroenterology, Dr. Desai provides a wide range of GI services including for bacterial overgrowth, constipation, acid reflux and GERD, IBS, incontinence and small bowel disease. Twitter handle: @NYGADocs
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/8photo

Why Kids Shouldn’t Invite Everyone in Class to Birthday Party
Here is why children have a right to invite only select classmates to their birthday party and should not be forced to invite the whole class.
*********
- Planning for your child’s birthday party?
- Have you told them they should invite their entire class?
- Dang! Would YOU invite all your COWORKERS to YOUR birthday party?
Should children invite every classmate to their birthday party?
“No, no, no! This is the same misguided advice that says that every kid should get a trophy in a competition,” says Dr. John Mayer, a practicing clinical psychologist specializing in teens/families/children/young adults, and author of “Family Fit: Find Your Balance in Life.”
Dr. Mayer continues, “It does not teach children/teens the REAL WORLD and does not teach appropriate relationship building.
“That’s why we have so many people walking around with no social skills. Forcing a child to invite everyone — you are modeling inappropriate social skills and hindering the child’s social development.”
And what should parents do if their kid’s classmate invites just about everyone to a birthday party except their child?
I once read a letter to “Dear Amy” concerning parents perplexed by this common problem with kids’ birthday parties. The parents were distressed over how to handle this.
In a perfect world, everyone in the whole class is invited to every kid’s birthday party.
But it doesn’t work that way, and parents should educate their “rejected” kids why. It’s part of learning about life.
“It is a good, normal and beneficial experience to be rejected and it prepares you for losses and transitions later in life,” says Dr. Mayer.
Anyone — parents or childfree adults — can relate to this birthday-invite phenomenon, because the exact same thing happens to adults in the workplace.
Just about every person who works in an office has experienced “rejection” when a coworker invited practically the entire office to a birthday party, barbeque, baby shower or some other event.
If parents believe kids should invite their entire class to a birthday party, in the name of not letting any child feel left out, does this mean that the parents, themselves, would invite every single one of their coworkers to their own birthday party, housewarming party, dinner party, college kid’s graduation party, summer barbecue, Christmas party, etc. ?
How many parents include every coworker on their own party list?
It’s not an issue of limited seating. There may be only eight coworkers. Yet two or three will not be invited to your birthday party or other event.
Adults indeed have a right to invite whomever they please. Why shouldn’t this same right extend to kids?
Children are capable of liking some classmates, while disliking others. They have just as much right to this as their parents do with office coworkers.
If you disagree, then what’s the cut-off age to where kids are finally old enough to invite only a select group to a birthday party? 12? 14? 16?
Are children supposed to magically like everyone their age?
- Maybe Emily can’t stand Billy because Billy often talks about unpleasant things.
- Perhaps McCayla is always bragging about herself.
- Maybe Kelsi hardly talks.
- Perhaps Tommy never bathes.
- Maybe your little angel is actually a bully at school.

Freepik.com
Don’t harangue your child for not inviting everyone to their birthday party any more than you’d appreciate being given the third-degree over why you excluded some coworkers from your summer barbecue.
Children need to learn that they will sometimes be excluded from birthday parties and that not everyone owes them an invite.
If they don’t learn this, how will they handle not being invited to a coworker’s baby shower or dinner party years later? How will they deal with any kind of rejection in life?
How parents react when their kids are excluded from a party is extremely important — kids learn values and coping methods from parents.
Explain to your child that some personalities go together as well as peanut butter and jelly, while others don’t quite match up.
Don’t make a big deal out of the “rejection,” and your child won’t, either.
 Dr. Mayer is a practicing clinical psychologist who treats adolescents, children, families, violent and acting-out patients, substance abusers and disorders of young adults.
Dr. Mayer is a practicing clinical psychologist who treats adolescents, children, families, violent and acting-out patients, substance abusers and disorders of young adults.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Why You Should NEVER Make Your Kids Give Hugs!

“Is it okay to make my child hug people against his or her will?” NO, NO and NO!
This article is about making (requiring, forcing) your child to “give a hug” to either someone they just met, or someone they’ve previously been in the presence of a few times or even more than occasionally (i.e., uncle or aunt, childhood friend of yours, “nice lady” at the candy shop).
Why do parents make kids hug people against their will?
Because some parents believe that if they DON’T say, “Give Aunt Alice a hug,” or, “Give that nice lady a hug for fixing your doll,” that people will think they’re failing to teach their kids manners.
Another reason is that parents think forcing hugs teaches their child to be affectionate.
But affection cannot be taught like math and vocabulary can be taught.
“Trying to force your child to hug someone is not only counterproductive, it can lead to dangerous consequences,” says Carole Lieberman, MD, a forensic psychiatrist and author of Bad Girls: Why Men Love Them & How Good Girls Can Learn Their Secrets.
“Children are not puppies who innately greet people with kisses,” continues Dr. Lieberman.
“They need to be given a lot of affection from their parents in order to spontaneously want to give affection back to anyone.
“And, if they are affectionate in general, except to someone they don’t spontaneously want to hug, it’s a red flag that parents should note.
“Maybe they don’t want to hug Aunt Alice because she smells of cigarette smoke.
“Or maybe they don’t want to hug Uncle Jim because he’s been touching them inappropriately.”
Dr. Lieberman mentions that if parents have been giving a lot of affection to a child, but he or she is still not affectionate, this could signal a neurodevelopmental condition such as autism.
But nevertheless, Dr. Lieberman continues: “In no case should you try to force your child to hug anyone, even though it may be embarrassing for you at times.”
Your child’s well-being always ranks higher than the alleged feelings of Aunt Alice, Uncle Freddy or that “nice lady.”
For what it’s worth, I have never, in my entire life, felt disdain towards any parent simply because they did not order their child to give me a hug!
Dr. Lieberman adds, “Forced hugs won’t teach your child to be compassionate or loving. Only your behavior towards them and towards the rest of the world will teach this.”
When parents make kids give hugs, whose best interests are the parents considering? Their OWN! People want to make a good impression, and, in their minds, what better way to do that than to order kids to give a hug?
So what’s wrong with making children give hugs?
It fails to take the child’s feelings into consideration. When’s the last time you felt like hugging someone you hardly knew or at least felt uncomfortable with? Think about that.
It’s natural for an adult to want to hug the stranger who just fixed their flat tire in the pouring rain.
But outside of major and minor heroics, many adults don’t care to hug people they barely or even casually know. Why should children? And if the adult is a relative, this should not matter.
Funny how the mother who’s thankful that the stranger fixed the doll and is ordering her introverted daughter to hug the stranger, won’t hug the stranger HERSELF.
Giving kids control over whom they hug or who touches them, teaches them that they have dominion over their bodies, and that nobody has the right to touch them “funny.”
Kids who feel they have the final say-so with whom their body comes in physical contact are far more likely to immediately report sexual abuse after the first time, rather than stay silent for years and years while the predator violates them over and over.
Dr. Lieberman explains, “Forcing your children to yield their body to someone they don’t want to be in contact with, teaches them to do this in other situations, which makes them vulnerable to being a victim of sexual abuse.
“It makes kids believe that they have to please others who want to touch their body. This makes it less likely that they’ll recognize how wrong sexual abuse is, and be less likely to refuse these advances and to report it right away.”
Parents also need to consider how the recipient of their child’s hug feels.
That “nice lady” who fixed your daughter’s doll doesn’t necessarily like to be hugged by little kids (or anybody, for that matter) unless she’s very close to them.
But is hugging a child such a bad thing for the adult?
To some, yes. Everyone has a threshold. What’s yours?
- Maybe you thrive on hugs, but somewhere else in your life, you lack courage. The adult who doesn’t want to receive a hug from your child may be skilled at doing things that leave you trembling. Think about that.
- Maybe they’re fearless at speaking before groups—something that petrifies you. Maybe they’re not the least bit nervous about asking a neighbor to turn down the booming music, but that’s something you’d never have the nerve to do. The point? Respect other adults’ boundaries.
Little girls, more often than boys, are ordered by parents to hug adults.
And women, more than men, are solicited as the recipients!
Dr. Lieberman points out that “there is an unfortunate expectation that girls are supposed to be more affectionate and compassionate people pleasers.
“But, forcing kids to hug someone indiscriminately teaches them that giving their love isn’t something special that should be reserved for special – whether this love is the warm friendly kind, familial, romantic or sexual.”
If you’re still not convinced of any of this, then what’s the cut-off age after which you will not order little Dakota to give her Aunt Alice a hug? When she’s nine? Ten? Or 12 and a half? Or 15?
If hugging is so important, why is there that cut-off age, and gender preference of female for both child and recipient?
Will you force your 15-year-old son to give a 30-year-old neighbor, Steve, a hug after the man fixes his skateboard?
 Dr. Lieberman analyzes the psychological impact of world events, as a guest and/or host on all major media outlets. Her appearances include “Larry King Live,” “The Today Show,” “Good Morning America,” “Entertainment Tonight,” CNN and Fox News.
Dr. Lieberman analyzes the psychological impact of world events, as a guest and/or host on all major media outlets. Her appearances include “Larry King Live,” “The Today Show,” “Good Morning America,” “Entertainment Tonight,” CNN and Fox News.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/altanaka

Philips HF 3520 Wakeup Light: Confusing, Poor Instructions

Be forewarned that the Philips HF 3520 Wake-up Light comes with very poor instructions, making its operation confusing.
I’m no dumb bunny. I have a four-year college degree, and my father has two, and neither of us were able to figure out how to set the “pm” and “am” times on my new Philips HF 3520 Wake-up Light.
We not only consulted with the very poorly written instruction booklet, but also tinkered around with the device without referring to the instructions.
My father has been working with machinery and DIY projects as a hobby for decades, having at one point built a porch on one of my childhood homes, and even HE couldn’t figure out the pm/am function on the Philips HF 3520 Wake-up Light.
After tinkering around with it again the next day, I gave up and called customer support.
The support person, once she had a duplicate unit in her hands…took a while to figure it out! Even SHE was stumped!
How do you set the pm and am time on the Philips HF 3520 Wake-up Light?
Select menu, select the clock icon, select 12H. The time in hours and minutes will blink, prompting you to select the correct hour and minutes.
If you do this at this point…you’ll be able to set the correct numbers. But not whether it’s pm or am.
The instruction booklet omits a step that should come right after you select the 12H but before you select the correct hour and minutes.
Right after you select the 12H, hold the “+” and “-” signs AT THE SAME TIME AND FOR A FEW SECONDS.
If you have the Philips HF 3520 Wake-up Light in your possession, you’ll know exactly where these signs are located.
Go ahead, check out the instruction booklet. I challenge you to locate where it states the aforementioned instructions about holding the plus and minus signs at the same time for a few seconds to get the pm and am set up.
After about two seconds (maybe less), the hour number will start moving.
Hold the plus and minus signs long enough to see the hour number move into the pm or am range (depending on time of day you’re doing this).
When you get to the pm (or am), then release the plus and minus signs. Whatever hour number it’s at will continue blinking—the prompt for you to set the correct hour time.
Select it, then select for minutes. You’ve now have the correct time of day.
Page 12 of the Philips HF 3520 Wake-up Light instructions has visual instructions for setting the clock, but nowhere mentions anything about simultaneously holding the plus and minus signs.
Page 15 has visual instructions for “adjusting” the clock. Again, no instructions about holding the plus and minus signs at the same time.
Go ahead, check out page 12 and 15, and see if you can find the +/- instructions, either illustrated or written. You won’t.
It also doesn’t help that the unit lacks a “back button.” If you need to go back a step, you must go back all the way and start over.
However, if you’re in the middle of the menu and are doing nothing while you think, you’d better very soon hit something because the unit times out quickly, forcing you to start all over.
Yet another issue is that on page 15, there’s a brief mention of the 12H and 24H settings.
How many civilian consumers know that “24H” refers to military time? I certainly didn’t.
For years I’ve known how to convert military time to civilian time (easy), but never knew that “12H” refers to civilian time and that “24H” refers to military.
Yet whomever put together the instruction booklet for the Philips HF 3520 Wake-up Light erroneously assumes that civilians know the 12H and 24H terminology.
Another issue: The instructions should also point out that it will seem that the light and sound don’t come on at the same alarm time; that the light comes on first, and several minutes later the sound (birds, piano, ocean) kicks in. I wondered why there was this sound delay.
The support woman told me they start at the same time, but the sound begins at such a low volume that you at first cannot hear it.
So here I am, thinking the device is malfunctioning. The instruction booklet should point this out. There’s plenty of unused space on the pages to do this.
The fact that the booklet includes a toll free support number is no consolation for poorly written instructions.
I was on the line for almost an hour about these issues and several more, including why the lamp is at its brightest after being on for only several minutes even though the “dawn duration” time is set for 30 minutes.
Another problem: The “dawn duration” time, despite being set for 30 minutes, runs for at least 55 minutes — I say at least, because I haven’t left it on to see how long it will go.
The instruction booklet says you can set the time for UP to 40 minutes. Go figure.
The lighting to display the time cannot be turned off. The lowest setting is 1 out of 4.
So if you want to sleep in a perfectly black room, the lit-up time display will prevent this. Though the light is dim at setting 1, it still mimics a night light.
This flaw in design defeats the purpose of the totally black room — assuming that you want to maximize your melatonin production.
The presence of a night light (believe it or not) will disrupt melatonin production.
Covering the display will partially shield the light you want to wake up to, and also, the consumer should not have to hassle with finding a suitable concealment.
In my case I cut one-fifth the length off of a large sponge and will set the bigger portion before the time display to shield it.
So even though the Philips HF 3520 Wake-up Light may be the best sunrise simulator on the market (and maybe I’m wrong), it’s flawed, and the instructions are poorly written and confusing.
I might add that the “ocean” sound is mostly that of screeching seagulls. The ocean waves are secondary.
Maybe you like the sound of ongoing screeching seagulls, but when the product description says “ocean,” you should get THE OCEAN, not screeching seagulls that drown out the ocean.

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}