

Elbow Pain While Bench Pressing: Causes and Solutions

Elbow pain when you bench press DOES have definite causes and definite solutions.
You’ll want to get on board quickly before the injury becomes chronic.
There are specific causes of elbow pain both while, or after, bench pressing.
Edmond Cleeman, MD, is a board certified orthopedic surgeon who specializes in sports medicine and arthroscopic surgery of the shoulder, knee and hip.
Dr. Cleeman explains five possible causes of your elbow pain as a result of doing bench presses. They are as follows:
Though bench pressing is considered the king of chest exercises, it also stresses the triceps muscles.
“I’ve seen many weightlifters with triceps tendinitis and occasionally they develop a bone spur at the insertion site,” says Dr. Cleeman.
Tendons join muscles to bone, and this tendon juncture at the triceps to the elbow bone could be inflamed, causing pain there from bench pressing.
He continues: “Lateral epicondylitis/medial epicondylitis (tennis or golfer’s elbow). Essentially inflammation of the tendons that allow for gripping, flexion and pronation of the wrist.”
With this, the person will feel pain on the inside, or outside, of his or her elbow.
Another source of elbow pain from bench pressing is ulnar nerve irritation.
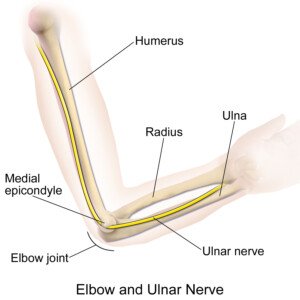
Source: BruceBlaus
This is the “funny bone” nerve that runs on the elbow’s inner side.
Ulnar nerve irritation will cause numbness and tingling in the pinky and fourth fingers, as well as that “funny bone” discomfort in the elbow.
Dr. Cleeman also says that inflammation (overload) of the ligaments and capsule can also be a culprit.

“Some I’ve seen have developed arthritis (wearing away of the cartilage) from the continuous overloading and stress for years.”
Solutions to elbow pain experienced from bench pressing: You won’t want to hear this, but you MUST lay off the bench pressing until the problem heals. Consult with an orthopedic doctor to get the right diagnosis.
Treatment for ulnar nerve irritation, for instance, isn’t the same as treatment for triceps tendonitis.
But in all cases, taking a vacation from bench pressing will be called for. Perhaps another chest routine won’t aggravate the joint, such as inclined dumbbell presses.
While the elbow problem is getting treated, you can replace bench presses with the “pec dec” as well as flyes.
How to Prevent of Elbow Pain from Bench Pressing
Dr. Cleeman advises the following:
“Stretching; Warm-up; Slow buildup in strength/weights;
Work on strength building other muscles in upper extremity besides the pecs;
Avoid bouncing the weights;
Have a personal trainer show you proper technique;
Consider icing down the elbow after a workout to prevent inflammation (similar to a baseball pitcher icing down their shoulder after a game).”
Basic treatment for elbow pain from bench pressing: Dr. Cleeman advises rest and ice, and “NSAIDS (e.g., Motrin, Advil, Alleve) are the key.”
He adds, “Possible injection (PRP-plasma rich platelet, steroid).”
 Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
 Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.

What Causes Foamy Urine: Serious & Benign

Ever had foamy urine?
There are several causes of foamy urine. Is cancer one of them?
If you’ve been noticing foamy urine and have been wondering if it might be a sign of cancer, worry no more; it is not.
However, this does not mean that foamy urine can’t be a sign of a serious medical problem.
What causes foamy urine?
“Foamy urine is caused by excessive protein in the urine, which can result from a person’s diet or kidney disease,” says Dr. Courtenay Moore, MD, a urologist with the Cleveland Clinic Health System.
“It can also occur while voiding rapidly, as foamy urine happens when urine mixes with air.”
When not to Worry
If it happens occasionally and isn’t progressing in terms of noticeability.
As Dr. Moore stated, foamy urine can result from rapid urination, which often occurs when you’ve been “holding it in” for a while and are very eager to let it all out once you’re sitting on the toilet seat.
In fact, more concentrated urine — the result of dehydration — may add to the foamy appearance.
You need not feel thirsty in order to be dehydrated, I might add.
If the symptom concerns you, make sure you drink plenty of fluids.
And void with more control, rather than hard pushing.
See if the bubbling or fizzing still persists.
When to Be Concerned
Now, if the symptom doesn’t go away even after you’ve restocked your body with fluids and have been voiding with less rapidity, this can signal the possibility of the excess protein, called proteinuria, in your urine.
This warrants further evaluation, as this can be a sign of a serious kidney ailment. However, it’s not necessarily a kidney disease.
If you have eaten ample amounts of certain foods, such as chicken, fish and other meats, this can cause the excess protein, as these foods contain muco-proteins.
The protein will end up in your excrement if your body is not efficiently breaking these proteins down.
These proteins then result in the foamy quality.
Cut back on these foods and see what happens. If the symptom persists, or, if in general you are just concerned about your observations, then seek a consultation with a urologist.
If your medical plan requires you first see a primary care physician, request a referral to see a urologist.
If kidney disease can be ruled out by the urologist, you’ll have peace of mind.
If the symptom persists despite the elimination of benign causes, your urologist will give you a urinalysis, which will detect any protein.
Further tests will then be given to find the cause.
 Dr. Moore’s clinical interests include voiding dysfunction, incontinence, female reconstructive surgery and female sexual dysfunction.
Dr. Moore’s clinical interests include voiding dysfunction, incontinence, female reconstructive surgery and female sexual dysfunction.
Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.

Why Does My Stomach Make Strange Funny Sounds?

Does your stomach make all sorts of gurgling, rumbling and other strange, weird sounds?
“Has it reached a point where other people can actually hear your belly making these noises?
I’m not talking about hunger sounds, either, but rather, sounds that come even when you are not hungry.
These stomach noises can occur soon after you go to bed, and they can also occur in the middle of the night while you’re lying in bed, or in the morning as you are approaching the time to get up for the day.
I asked questions about funny belly sounds to Edward Cruz Paredez, MD, a board certified gastroenterologist based in La Jolla, CA.
Dr. Paredez explains, “Funny noises from the stomach or digestive tract are made up of two components: the contents,” and “contractions of the stomach and intestines.”
Your intestines do not sit in a soundproof room; sound will travel through your abdomen and skin, and make it to your ears — and to other peoples’ ears sometimes.
Dr. Paredez explains, “The reason why some people make more funny noises than others is due to the variable amounts of gas/fluid and solid contents, and the strength or spasticity of the contractions.
“The loudest stomach noises usually represent a large amount of intestinal air and fluid, which travel like bubbles through segments of the intestine like hundreds of internal ‘burps.'”
Dr. Paredez also explains that swallowing excess air can cause loud and strange noises from the stomach.
So if you have embarrassing abdominal noises, ask yourself if you gulp air while chewing gum or drinking beverages.
“Many people swallow excessive air because of anxiety or nervous conditions: aerophagia,” adds Dr. Paredez.
Another Question to Ask
Do you gulp your food down but then hold in the urge to burp?
This can lead to funny or strange noises in the stomach.
“Others have excessive intestinal gas due to fermentation of sugars such as lactose, or fermentation of gassy foods such as beans or fiber, and this causes loud intestinal noises,” says Dr. Paredez.
Irritable bowel syndrome is another culprit behind noises in the stomach, leading to excessive contractions.
IBS is a clinical diagnosis derived from symptom based criteria.
“Most of the time no testing is necessary to diagnose a patient with IBS unless there are atypical symptoms or warning symptoms such as severe pain or bleeding,” says Dr. Paredez.
“Classic symptoms include anything from constipation to diarrhea multiple times a day,” particularly soon after eating, and abdominal cramps and abdominal pain.

Dr. Paredez has been named a Top Doctor by San Diego Magazine and has also received a 2016 “People Love Us on Yelp” Award.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Orange Diarrhea: Some Causes Are Serious

Have you had orange diarrhea lately?
That must have been a surprising sight, maybe even an alarming sight, since loose stools are supposed to be brown (though a little greenish is okay), not orange.
Diarrhea can come in an assortment of colors, and orange is one of them.
If you wish to examine the color of your bowel movements, the best way to do this is to make sure, first of all, that the lighting in the bathroom is good.
Next, if possible, urinate before you release your movement.
Next, flush the toilet so that the yellow of the urine won’t taint your perception of the color of your diarrhea.
When viewing the color of your bowel movement, lift the toilet seat up for a better view and better lighting.
“Stool can vary in color for a number of reasons,” says Edward Cruz Paredez, MD, a board certified gastroenterologist based in La Jolla, CA.
“The common colors of brown and green are due to the digestion of food and combination with yellow/green bile secreted by the liver.”
But what about orange diarrhea?

Dr. Paredez explains, “Orange diarrhea can be caused by food or supplements which contain orange food coloring, food with artificial yellow or orange coloring, or foods such as carrots, cilantro, collard greens, fresh thyme, kale, sweet potatoes, spinach, turnip greens, winter squash.”
Do you take turmeric supplements? Bright orange specks may show up in your bowel movements, though this should not actually color your bowel movements orange.
Dr. Paredez continues, “Orange diarrhea may be the result of infectious diarrhea, which causes rapid transit through the intestine, which limits the amount of bile in the stool.
“Less commonly it could also occur from a blockage of the bile ducts, which can be seen in cases of gallstones or bile duct or pancreatic cancers.”
Bile duct cancer and pancreatic cancer are the life-threatening medical conditions that can result in orange diarrhea.
However, this color in your bowel movements rarely means cancer.
“In fact, biliary blockage from cancer more commonly produces ‘white, grey or clay’ colored stools,” adds Dr. Paredez.
Another potential cause of diarrhea that has an orange tinge to it, is microscopic colitis, an inflammation of the lining of the large colon.
This non-serious condition interferes with food absorption (contributes to rapid colon transit).
So if you eat something that’s reddish or orange (not necessarily fruit; this could be the contents of a seasoning packet for rice), some of that may not get digested and will end up in your diarrhea — giving it an orange tinge.
Dr. Paredez has been named a Top Doctor by San Diego Magazine and has also received a 2016 “People Love Us on Yelp” Award.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ShutterOK

Fishy Urine Smell Caused by Infected Vagina: Men Can Get Infected

If your urine has a fishy smell, this isn’t a hygiene problem and will not be solved with extra bathing or more showers.
Fishy smelling urine is a common.
“Sometimes it can be difficult to tell if a ‘fishy’ smell is coming from the urine or the vagina,” begins David H.C. King, MD, Medical Director, Urology Services, El Camino Hospital Los Gatos.
“The most common cause of a fishy smell is usually related to common vaginal infections such as trichomoniasis, gardnerella, or bacterial vaginosis.”
If a man has a fishy smell “coming from” his urine, chances are, he may have picked up the bacterial infection from a woman he had sex with, who had trichomoniasis, or bacterial vaginosis.

Shutterstock/Siriluk ok
Trichomoniasis
This sexually transmitted disease is curable (though reinfection is always possible after successful treatment), and 7.4 million cases are diagnosed yearly.
Women can contract it from men and women, but men only contract it from women.
Men usually don’t have symptoms, but women often do (e.g., yellow-green vaginal discharge), including that fishy odor which may seem like it’s coming from the urine, when in fact it comes from the vagina.
Garderella
This is also known as bacterial vaginosis, which is an overgrowth of the “bad” bacteria that are normally found in the vagina. Vaginal itching and irritation are symptoms, along with vaginal odor, which may be fishy, seemingly originating from the urine.
In fact, this fishy smell is common with this condition.
Dr. King explains, “These conditions are easily treated with antibiotics.
“Sexual partners of these patients will also need to be treated. Condoms should be used until the antibiotics are completed.”
Thus, if you’re a woman who has been noticing a fishy smell coming from your urine, this unpleasant fishy odor is actually emanating from your vagina.
This means that you should be checked by your gynecologist for a vaginal infection. Bacterial vaginosis and trichomoniasis are not life-threatening, and again, they are curable.
If you’re a man who has noticed a fishy odor, have your physician examine you to see if you have picked up the infection from your sexual partner.
Being infected will not make you more immune or extra resistant to a future infection.
Multiple sex partners increase your risk of these infections; a long-term monogamous relationship with a partner who has tested negative will go a long way in helping prevent these infections — and thus, a fishy smell “coming” from your urine.
 With 20+ years in general urology, Dr. King specializes in prostate disorders, kidney stones and urinary problems in men and women.
With 20+ years in general urology, Dr. King specializes in prostate disorders, kidney stones and urinary problems in men and women.
Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Top image: Shutterstock/mistaht
Sources: cdc.gov urologychannel.com

Causes of Orange Urine: Can One Be Cancer?

Orange urine is easy to spot at just a glance in the toilet bowl or as it’s coming out.
And orange urine means something.
Urine should be an almost clear, or very light yellow color.
But when you have orange urine:
“Medications (e.g., Pyridium) may cause the urine to appear orange,” says Dr. Andrew Stephenson, MD, Section Chief and Director, Urology Oncology; Professor (PAR), Department of Surgery, Division of Urology, Rush Medical College.
“Bilirubin is the byproduct of red blood cell metabolism,” continues Dr. Stephenson.
“This is normally metabolized by the liver and excreted into the bowel via the bile duct (this is why the stool appears brown).
“The liver does not efficiently metabolize bilirubin in the setting of liver disease; hence, the bilirubin accumulates in the blood and is excreted in the urine (causing orange urine) by the kidneys.”
Thus, orange or tea-colored urine can be a symptom of liver disease.
However, an orange hue in the urine can also be caused by food such as carrots, carrot juice, winter squash, blackberries and beets.

Orange urine from beets. Jmarchn/CC BY-SA 3.0
Vitamin C, B complex vitamins, beta-carotene (the compound in carrots that make them orange), senna herbs, and foods with orange dye can result in the same appearance as well.
Besides Pyridium, which is used to treat urinary tract infections, other medications can be culprits:
Rifampin, an antibiotic; and
Warfarin (trade name Coumadin), a blood thinner.
In addition, some chemotherapy drugs and laxatives can have the same effect.
Lastly, dehydration can cause a bright, deep yellow, dark yellow, yellow-orange, light orange or medium orange. You need not feel parched to be dehydrated, by the way.
Thirst isn’t the only symptom of dehydration, and you may not even be the slightest bit thirsty during periods that your body has inadequate hydration.
Lack of fluid intake can concentrate urochrome, which is the end product of hemoglobin breakdown.
Urochrome is what gives urine its normal pale yellow color.
When this agent is concentrated, it yields the more intense or dark yellow characteristic of dehydration.

The color change from eating a lot of carrots, carrot juice, beets, etc., is harmless.
Just be sure that you know that this is the cause of the color change.
Ask yourself if you’ve been eating any of these foods or taking the supplements mentioned.
In fact, the foods mentioned in this article, if eaten in enough quantities, can give the palms and soles of the feet an orange tinge.
If after stopping consumption of suspected foods, supplements or dyes for a few days, your urine is still orange, visit a urologist to see if any health issues can be causing the discoloration.
See also if you can make the orange go away by drinking 10, eight-ounce glasses of water a day.
If your medical insurance plan requires that you first see a primary care physician to get to a urologist, then don’t just stop at the primary care doctor; get a referral to a urologist.
 Dr. Stephenson’s clinical and research focus is the treatment of prostate, bladder, kidney and testes cancer. He has published over 100 articles in peer-reviewed journals.
Dr. Stephenson’s clinical and research focus is the treatment of prostate, bladder, kidney and testes cancer. He has published over 100 articles in peer-reviewed journals.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Top image: Shutterstock/Igor Nikushin

What Makes My Gas Smell So Bad?

Pheeuw, do you have really bad smelling gas?
It’s been said that really foul smelling gas means that the offender is very healthy. Of course, this is just a crazy myth.
“Silent but deadly” has been used to describe the smell of human gas. I asked what makes flatulence smell so bad to Edward Cruz Paredez, MD, a board certified gastroenterologist based in La Jolla, CA.
First of all, just what are “farts” made of?
Dr. Paredez explains: “Flatus is made of nitrogen (N2), oxygen (O2), carbon dioxide (CO2), hydrogen (H2), and methane (CH4), which account for more that 99 percent of expelled intestinal gas.”
So what about flatulence, then, is responsible for its awful odor?

Shutterstock/pathdoc
Dr. Paredez continues: “The hydrogen sulfide and other compounds (mercaptan, butyric acid and carbonyl sulfide) make the released gases smell bad.
“Humans actually expel little methane compared to ruminants such as cows and sheep.”
There is another explanation yet, for why the gas of humans stinks so bad.
“Humans hold their gas in much of the day and allow longer periods of fermentation compared to most animals who pass gas every hour!” says Dr. Paredez.
“This is especially true with the modern workforce who work indoors in close proximity to other people (i.e., cubicle workers).”
Interestingly, a person may not even think that his own flatulence smells that bad.
But the odor from the flatulence coming from other people can just about knock him flat on his back.
“A change in diet or a medication can often trigger a period of particularly bad smelling gas,” says Dr. Paredez.
Some people have reported that cutting back on carbohydrates, especially the carbs that are found in processed food, results in less flatulence, and thus, less odor.
Some medical conditions can cause very foul smelling gas, such as irritable bowel syndrome and inflammatory bowel disease.
However, these conditions bring with them other symptoms that are difficult to ignore, such as diarrhea, change in appearance of stools, abdominal cramps and sometimes abdominal pain.
If you’re not able to trace your foul smelling flatulence to foods, then make an appointment with a gastroenterologist, who will then order some tests to see if there is a medical cause.
A stool sample test may be one of the tests ordered.
Your doctor may also recommend a colonoscopy, even if you’re in your 20s or 30s; colonoscopies are useful for detecting inflammatory bowel disease.
Dr. Paredez has been named a Top Doctor by San Diego Magazine and has also received a 2016 “People Love Us on Yelp” Award.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Aaron Amat

Painless Ongoing Diarrhea As Only Symptom: What This Might Be

Are you experiencing sudden diarrhea out of the blue for no apparent reason, and other than the diarrhea, you feel fine?
Is the diarrhea particularly watery or “liquidy”? Perhaps between episodes of this mysterious diarrhea, you feel perfectly normal, even quite fit and healthy.
What medical condition presents with sudden-onset diarrhea that then persists, and no other symptoms?
It may very well be microscopic colitis. However, it may also come with other symptoms: abdominal cramps, nausea and mild joint aches.
But painless diarrhea is the key symptom of microscopic colitis.
“The differential for painless diarrhea would include microscopic colitis, irritable bowel syndrome, cancer, food allergies or sensitivities, some infections, pancreatic insufficiency and medications,” says Alan Gingold, DO, a board certified gastroenterologist with Central Jersey Ambulatory Surgical Center.
“Microscopic colitis is a chronic inflammatory condition of the colon where the inflammation is at the cellular level and can only be seen by microscope.”
I’ve had microscopic colitis, and my gastroenterologist told me that this can be mild to severe.
In severe cases, a person may be having diarrhea many times a day and lose 30 pounds.
“The disease is broken down into two subtypes: lymphocytic colitis and collagenous colitis,” says Dr. Gingold.
“Usually presents in middle-aged females and presents as intermittent bouts of non-bloody diarrhea that typically comes and goes on its own.”
Men and younger women are not immune, though.
The symptoms of microscopic colitis can mimic the symptoms of an intestinal infection that’s limited to the intestines, versus an infection that goes body-wide and causes a fever.
My doctor initially diagnosed me with an intestinal infection — before he performed the colonoscopy. Before the doctor entered the colonoscopy room, his nurse actually suggested that I had IBS — irritable bowel syndrome.
The nurse then thought that my diarrhea might have been caused by mental stress. He told me that he himself suffered from diarrhea for two weeks following his divorce.
But I knew my diarrhea couldn’t have been caused only by stress, because it was not normal-appearing diarrhea.
The diarrhea of my microscopic colitis was light brown, almost tan, and tended to assume a tinge matching the color of the foods I had eaten the day prior.
I saw chunks of food in these loose, flimsy stools. Sometimes the bowel movements were pure diarrhea, spewing out very easily and dispersing all over the place in the toilet water.
Other times it appeared to be in solid pieces, but then when I prodded the pieces with a cotton swab, they instantly dispersed. I saw food bits everywhere.
This was all the result of microscopic colitis, an inflammatory bowel disease.
The Cause?
“The underlying causes of microscopic colitis is unknown,” says Dr. Gingold. “It may be due to an autoimmune condition — although chronic use of NSAIDs (e.g., Alleve) have also been suggested as a possible etiology.
“Because there are many other conditions that can present similarly, it’s a diagnosis made by taking a biopsy of the colon during an endoscopic exam by your gastroenterologist.”
Samples of the inner lining of the large colon are collected and sent to a pathologist.
This is why a colonoscopy is required to confirm microscopic colitis.
If you’ve been experiencing sudden-onset (though this is not always the case) diarrhea, particularly watery in nature, and especially if it contains food particles — and you have no other symptoms — you may very well have microscopic colitis.
But remember — only a colonoscopy can confirm this.
Microscopic colitis may resolve on its own for some individuals. In severe cases, medications can be prescribed. Kefir may also relieve the diarrhea.
 Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Dr. Gingold attributes his success to the extra time he spends with his patients. His areas of expertise include reflux disease, Barrett’s esophagus, capsule endoscopy, chronic liver disease and inflammatory bowel disease. Dr. Alan Gingold is board certified by the American Board of Internal Medicine in Gastroenterology
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

IBS (Irritable Bowel Syndrome) or Colon Cancer Symptom Comparison

Symptoms of IBS (irritable bowel syndrome) and colon cancer are nearly identical.
In fact, they are so similar that I had to wonder if there was a way that a person, who is experiencing troubling symptoms that fit the bill for IBS — but also for colon cancer — can tell at home the likelihood that his symptoms point more towards IBS than colon cancer, or .
.. dreadfully, point more towards colon cancer than irritable bowel syndrome.
The symptoms of irritable bowel syndrome are terrifying to anybody who experiences them and is familiar with the symptoms of colon cancer! They’re virtually the same!
Unfortunately, when it comes to if there are any ways that the patient at home can try to determine if his symptoms point more towards either irritable bowel syndrome or colon cancer:
“None — IBS is a diagnosis of exclusion and should only be made in my opinion after a full evaluation,” says Whitney Jones, MD, a national expert and frequent speaker on early-age onset colon cancer prevention, and Founder, Colon Cancer Prevention Project.
“Blood in the stool (obvious or found in fecal occult blood testing) always requires a structural evaluation (i.e., colonoscopy).”
Suppose a person develops IBS, but out of fear or lack of money, refuses to see a doctor.
Instead, he just hopes that the alarming gastrointestinal symptoms are indeed irritable bowel syndrome, vs. colon cancer.
He decides that as time goes on, if the symptoms don’t worsen, this makes it increasingly unlikely that it’s a malignancy.
He also decides that as long as new symptoms don’t arise, such as jaundice (possible sign that colon cancer has spread to the liver), that his condition is likely benign.
After a long enough time passage, with no worsening symptoms or unexplained weight loss, and still able to function quite well physically, a person in this situation may come to assume that whatever’s going on isn’t colon cancer.
After all, if a long enough time passage has occurred, he is likely to conclude that if it were colon cancer, it would have killed him already, or, at least, rendered him too sick to get out of bed.
This hypothetical situation will put the person through unspeakable anxiety.
Why not just get the colonoscopy for peace of mind, even if you have no insurance?
Dr. Jones explains, “All too frequently, patients have months or even years of symptoms attributable to IBS who are subsequently found to have colon cancer as the underlying cause.
“The ‘it’s better so I’m better’ strategy is not one I would recommend.
“Rather, if there are limited resources, I would seek out a public health care center or clinic and follow through with an evaluation by a health care professional.”
Warning: A person may very well have IBS, but then by sheer coincidence, develop colon cancer, and hence its symptoms.
A diagnosis of IBS should never make a person feel immune to colon cancer.
Too many people are walking around with a diagnosis of irritable bowel syndrome despite never having a colonoscopy to rule out some other cause such as colon cancer.
Dr. Jones says, “My recommendations are that if an improved high fiber diet, supplemental fiber and probiotics over 2-4 weeks do not improve symptoms, patients need evaluation by a digestive health professional.”
Anti-diarrheal or laxative agents should not improve symptoms of colon cancer.
“If we are going to catch some of these atypical earlier colon caners, we must lower the threshold for colonoscopic evaluation.
“And strongly consider lowering the age at which we begin the discussions about colon cancer signs, symptoms, family history, to age 40, with colonoscopies recommended at age 45 for all.”
The argument against this is that colonoscopy is an invasive procedure with risks, namely perforation of the colon.
This is rare, however. Another argument is that colon cancer is uncommon in people under 50, particularly 20s and 30s.
Of such patients, 15.1 percent are diagnosed between age 45 and 54, according to the National Cancer Institute as of 2021.
However, this low incident rate is of no consolation to these younger patients!
“I think this will be a hot topic ongoing in the future and like the new recommendations for breast and cervical cancer, will be debated in the public forum,” adds Dr. Jones.
“I favor finding the polyp and skipping the cancer. Previvor trumps survivor any day in my practice.”
IBS (irritable bowel syndrome) Symptoms
- Abdominal pain/cramping
- Feeling bloated
- Gas
- Diarrhea
- Constipation
- Alternating diarrhea and constipation
- Mucus in stool.
- Symptoms may not respond medical treatment.
Additional Symptoms
Change in stool caliber and consistency including stools that are hard, like pellets or pencil-thin.
After having a bowel movement, you may still feel incompletely voided. More symptoms: fatigue, backache.
Colon Cancer Symptoms
- A change in stool caliber and consistency — including pencil thin stools
- Diarrhea
- Constipation
- Alternating diarrhea and constipation
- Abdominal pain/cramping
- Gas or a bloated feeling
- Sensation of incomplete voiding after a bowel movement
- Fatigue without explanation
- Blood in the stool; may appear red, dark or like a gooey tar
- Leg pain is possible.
Blood in the stools or “tarry” stools is not common with IBS.
However, these symptoms don’t always occur with colon cancer, either.
Unexplained weight loss is another feature of colon cancer, but people with IBS can also experience weight loss from all the diarrhea.
 Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Dragana Gordic

Causes of Thin Narrow Stools Besides Colon Cancer

If your thin or narrow stools have you fearing colon cancer, there are other causes of narrow thin stools besides cancer of the colon.
A number of factors can determine bowel movement caliber (shape, texture, color, etc.), says Whitney Jones, MD, a national expert and frequent speaker on early-age onset colon cancer prevention, and Founder, Colon Cancer Prevention Project.
Dr. Jones explains, “Stool content (e.g., solids vs. liquids), the amount of time stool spends in the gastrointestinal tract (i.e., transit/motility), and the function of the anal sphincter are all known to be involved in this process.
“Alterations in stool consistency and a resultant ‘change in bowel habits’ are known symptoms of a number of disease processes such as inflammatory bowel disease, cancer, and irritable bowel syndrome.”
And the possible causes of narrow or thin stools don’t stop there.
Have you increased your fiber intake lately?
This can cause BMs to come out thinner than usual.
Have you been eating Olestra or anything with sorbitol?
Dr. Jones says, “Ultimately, any process that affects stool consistency (e.g. dietary changes,), bowel transit or motility (e.g. chronic constipation, medicines, inflammatory conditions involving the GI tract), and/or anal sphincter function (e.g., rectal cancers, trauma, and surgeries) could result in long narrow stools.”
Your BMs may even be on the narrow side on a normal basis, and you’ve only noticed recently because perhaps you read an article on colon cancer.
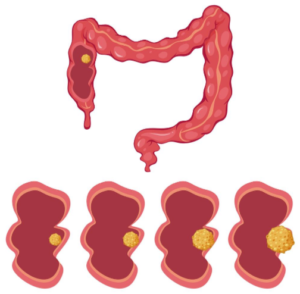
Schematic of colon cancer. Source: vecteezy.com
Dr. Jones stresses that what’s particularly important is whether or not narrow, thin stools are outside the norm for your typical BM appearance.
Don’t delay discussing any change in bowel habits with a gastroenterologist.
Though narrow, thin stools can result from colon cancer, this does not mean that if you have skinny BMs, you probably have colon cancer.
It’s actually most likely from a condition other than colon cancer. This includes diverticulitis.
In fact, it might even be from microscopic colitis, which I’ve had.
One day a very long BM came out and it was on the narrow side, more narrow than usual, but not what I’d consider as thin as or like a pencil.
What made the stool appear more narrow than usual, however, was perhaps its very long length.
I imagined it being segmented, and realized that if broken into thirds or fourths, it wouldn’t seem as “narrow.”
It just so happened that this particular BM didn’t break up upon hitting the water.
Dr. Jones explains, “Regarding the caliber of stool and its correlation with the presence of left sided colon cancer, the data currently available does not necessarily indicate that narrow stools should alert patients or physicians of a possible malignant process.
“The notion that left sided colon cancer or rectal cancer often presents with narrow stools is based upon the anecdotal opinion of expert physicians of the late 19th/early 20th century.”
Dr. Jones adds: “There are no prospective studies and only a few retrospective studies in the literature that indicate that long narrow stools are correlated with cancer.
“This conception has been propagated throughout the medical literature mostly based on tradition.”
Most early colon cancer presents with no symptoms.
This is why there’s the extreme importance of getting screened for this killer with a colonoscopy.
This should begin at age 45 for people at average risk (due to age) for the disease, and then done every 10 years, unless otherwise indicated by the physician.
Anal cancer, which is rare, can also cause “narrowing of the stools,” according to the American Society of Colon and Rectal Surgeons.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}