

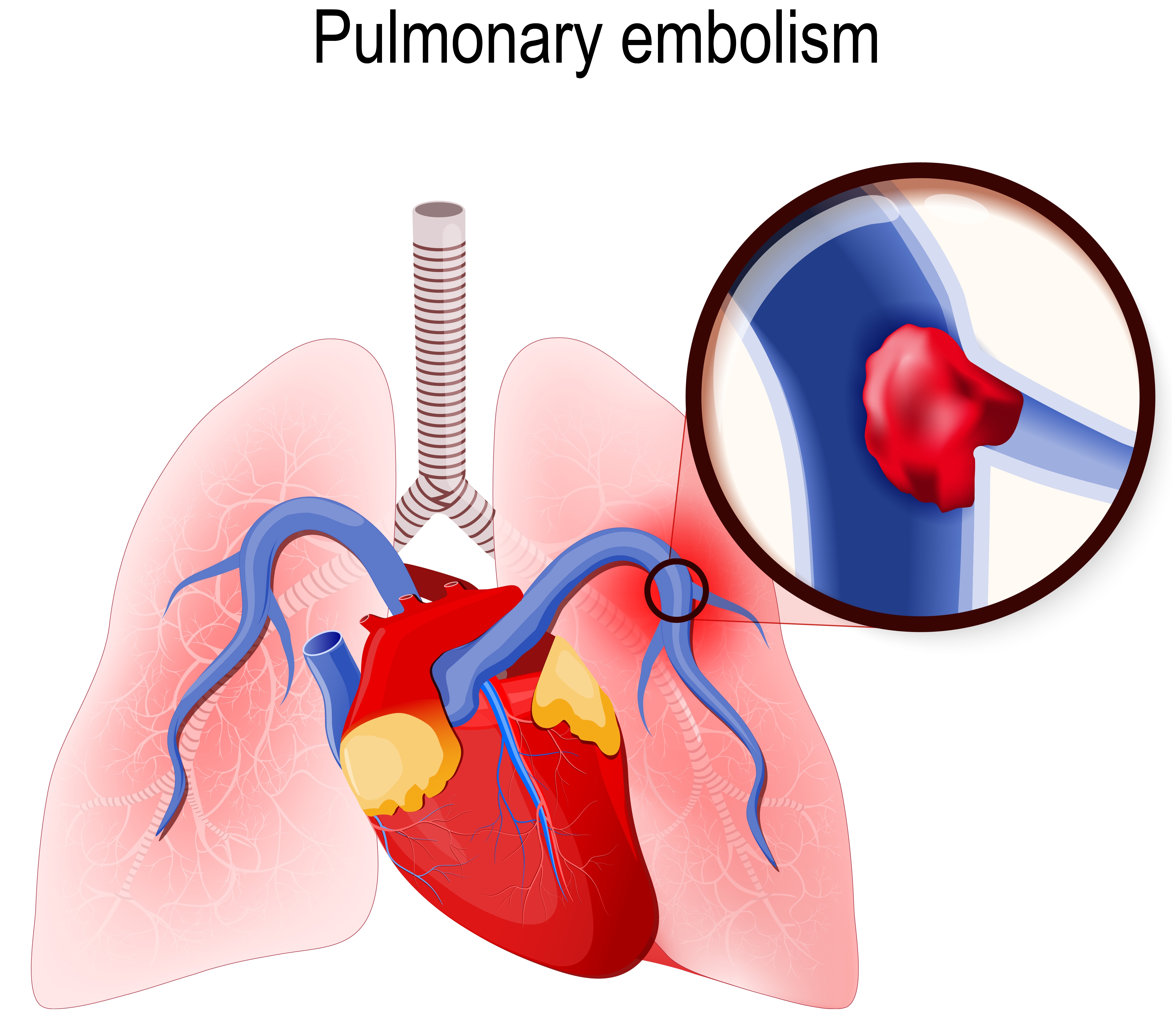
Can a Pulmonary Embolism Kill You on the Way to a CT Scan?
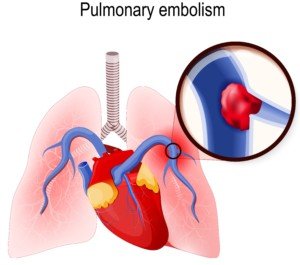
A pulmonary embolism is suspected, and the patient is being taken to the CT scanner to confirm this.
The D-dimer was positive and the patient is exhibiting the classic symptoms of a pulmonary embolism.
But the CT scan is needed for a verification before any powerful clot-busting drug is given. Doctors also need to see where the clot is specifically.
Yet on the way to the CT scan suite, the patient could go into cardiac arrest from the pulmonary embolism.
I wondered why isn’t the clot-busting drug immediately administered, right there in the hospital room — at least at a lower level — and THEN take the patient for his CT scan?
After all, it takes time to get to and on the CT scanner bed, take the image, then get a doctor to read the image results.
Certainly, the pulmonary embolism can cause death while the patient is enroute to the CT scanner or even during the scan?
Regarding the hospital patient presenting with sudden difficulty breathing and chest pain, “Clinically this scenario is one with a high index of suspicion for a pulmonary embolism,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“Of course if the patient is on a cardiac monitor, you can look for tachycardia, EKG changes with signs of right heart strain, etc., to strengthen that suspicion.
“In most cases what you do next is start anticoagulation with IV Heparin immediately if it is not contraindicated; you do not need a confirmation with a CT to start treatment.”
Anticoagulation drugs are contraindicated in patients prone to internal bleeding.
Dr. Gashti explains, “In certain post-op patients such as spine surgery or neurosurgical patients, thrombolytics — clot busting drugs, and to some extent even Heparin is absolutely contraindicated because of risk of bleeding.”
Filter Can Prevent Pulmonary Embolism
“In these patients, you would place a filter, and if they are not in cardiac shock, you would support them.”
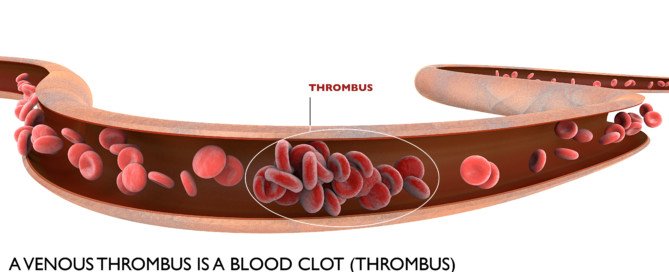
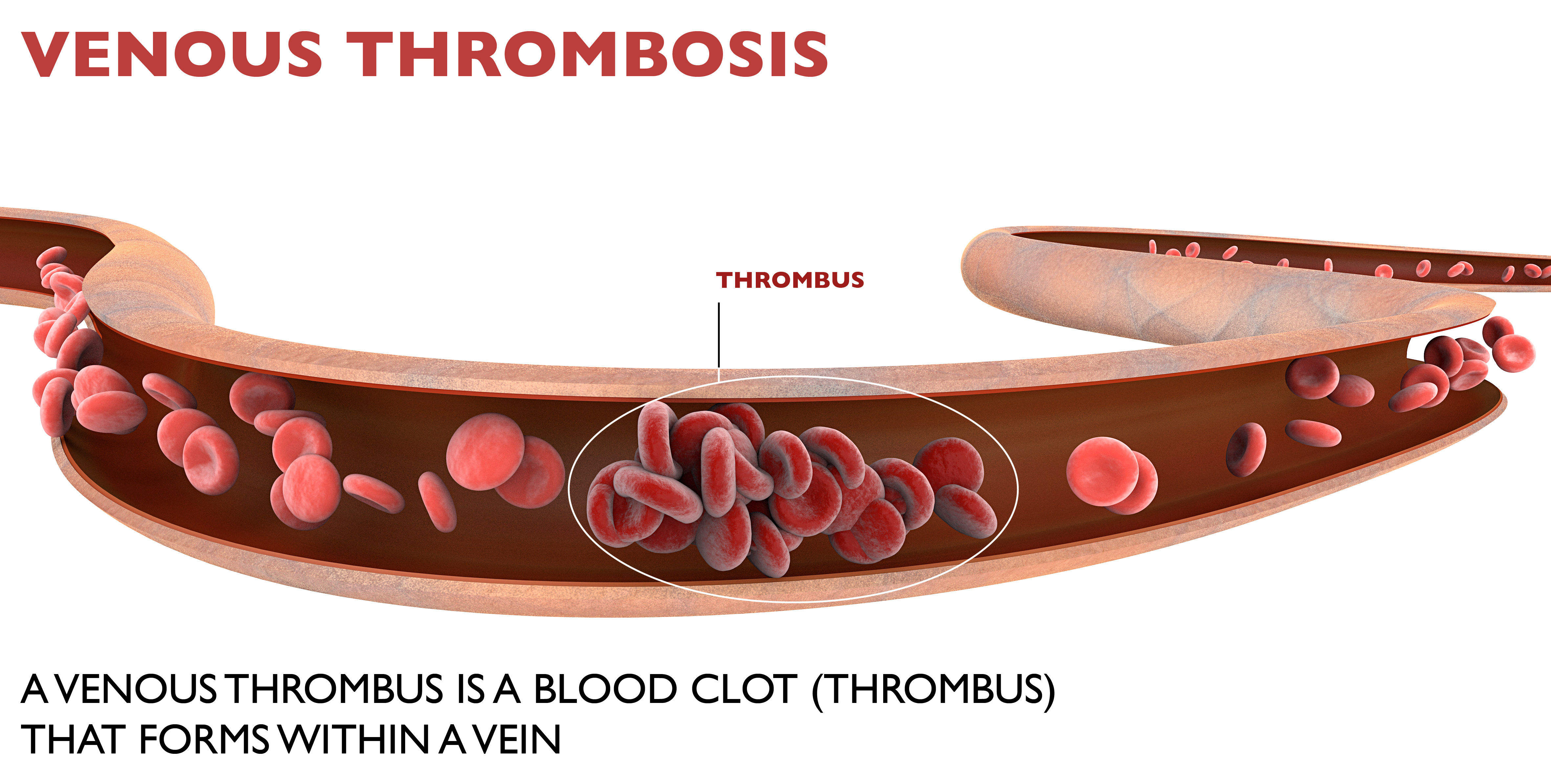
This filter (shown below) will prevent any deep vein thrombosis from getting into the lungs and embolizing.

IVC filter. BrusBlaus/CreativeCommons
Other patients may have hemodynamic problems. “If they are hemodynamically unstable, then they will need surgical thrombectomy — mechanically removing the blood clots (from the lungs),” says Dr. Gashti.
A patient who’s hemodynamically UNstable is NOT necessarily at risk for internal bleeding from thrombolytic drugs. Hemodynamics refers to primarily blood pressure.
“In a patient with hemodynamic instability in whom thrombolytics are not contraindicated, you can start IV thrombolytics, but this is not as effective as performing an angiogram and placing a catheter into the pulmonary artery where the blood clot is and delivering the medicine directly there; this of course requires a trip to the angio suite.”
This procedure is called intra-arterial infusion (of the thrombolytic drug), and is not to be confused with the surgical thrombectomy, which involves opening the chest, accessing the pulmonary artery and physically removing the blood clot—a major surgery.
Two Ways to Deliver Thrombolytics
IV and intra-arterially (through the femoral vein in the upper leg, feeding a catheter up to the pulmonary artery and delivering the clot-busting drug).
Dr. Gashti emphasizes that “in a patient with suspected or confirmed pulmonary embolism, who is hemodynamically stable (and not at risk for internal bleeding), all that is needed is systemic anticoagulation (which can be delivered via IV or intra-arterially). Most PE’s will not be fatal.
“So as you can see, this is not a condition where one treatment fits all. It really all depends on how the patient is doing.
“As you correctly mentioned, some patients are not stable enough to travel to the CT scanner, but a CT is only done for confirmation.
“If you suspect it, then treat it and worry about confirming it later.”
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Designua

Is Chest Pain, Breathing Trouble After Pulmonary Embolism Treatment Normal?

Is it normal to have trouble breathing and chest pain after successful treatment of a pulmonary embolism?
Might these symptoms reflect anxiety over the pulmonary embolism, or is it more likely that this means you have a new blood clot in your lung?
What a Doctor Says…
“If you are diagnosed with a DVT and a pulmonary embolism and being treated for it with systemic anticoagulation, and you are therapeutic on Heparin or Coumadin, the chance of having recurrent pulmonary embolism is low, but not zero,” says Seyed-Mojtaba (Moji) Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“So recurrent symptoms mandate new diagnostic workup—most likely a chest CT, and if recurrent PE is confirmed, patient has to have an IVC filter because this constitutes ‘failure of treatment,’ one of the indications to insert a filter.”
IVC stands for inferior vena cava. This is a large vein that carries blood into the lungs so that it can be re-oxygenated.
How long does the filter to prevent a pulmonary embolus stay in place?
Dr. Gashti explains, “If they suffer a PE, first or recurrent, while being anti-coagulated and therapeutic on their Coumadin, then this is a case of failure of therapy, and in most cases you would not remove their filter—it would be permanent.
“Having said this, you also need to look at the patient.
“If they are young and if their deep vein thrombosis was provoked, you may consider removing the filter but need to be careful with this.
“In any case, with current filters, the longest they can stay before having to be removed is 365 days.”
Symptoms of a Pulmonary Embolism
In addition to sudden chest pain, the patient may experience a sudden difficulty with breathing or getting air in, or may even pass out.
Coughing up blood is another possible symptom of a pulmonary embolism.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik/peoplecreations

Pulmonary Embolism: What Can You Do Besides Call 9-1-1?

Would you know what to do, besides call 911, if someone near you seemed to be showing signs of a pulmonary embolism?
After all, a PE can kill in minutes.
“Sudden onset of shortness of breath and chest pain are hallmarks of pulmonary embolism,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Another symptom may be coughing (including with blood).
“If you just had major surgery and you are at home and experience these symptoms, especially if one of your legs is also swollen, this would be a PE unless proven otherwise.
“Of course there are numerous other causes in a post-op patient with these symptoms—pneumonia, atelectasis, cardiac issues, CHF, etc., but a PE has to be on top of the differential and you need to call 9-1-1.”
But is there anything else that you, as the layperson, can do to help this individual with the suspected pulmonary embolism?
Dr. Gashti says, “Unfortunately, if you are not in a hospital, perhaps not a whole lot.”
Perhaps you’ve viewed a scene in a fictitious TV drama where it appears that someone with medical training thinks a collapsed person is suffering from a pulmonary embolism.
The bystander then takes a sharp object, incises the chest somewhere and inserts a makeshift medical device (such as a drinking straw), and performs crude surgery.
Dr. Gashti explains, “The situation you are describing on a TV show sounds like treatment for a pneumothorax—collapsed lung, rather than a pulmonary embolism.
“With a collapsed lung, the problem is getting enough air to the lungs ,but a PE prevents blood from getting to the lungs from the right side of your heart. So placing a ‘tube’ in your chest would not work.
“Other possibility is that they were talking about a ‘tracheostomy’ tube through the middle of your neck into your trachea to ventilate the patient.
“But the general public should not attempt this since there can be more harm than good if you do not know what you are doing.
“So the best thing the general public can do if they suspect PE is to call 9-1-1 and to provide basic CPR if patient is unconscious.”
We may have to wait several decades before “Star Trek medical technology” allows a bystander to whip out the pulmonary embolus dissolution kit from their handbag and apply it to the collapsed victim.
In the meantime, know the warning signs of a pulmonary embolism.
If someone is at risk, check their legs several times a day for swelling, redness, a blanched or pale appearance, warmth in the area or tenderness to the touch.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/fizkes
When Are IVC Filters Used for Pulmonary Embolus Prevention?
How many hospital patients would die from a pulmonary embolism every year if from this point on, all surgery patients received an IVC filter — patients undergoing surgeries that increase the risk of a DVT?
Surgeries that strongly increase the risk of a deep vein thrombosis include knee replacement, hip replacement, abdominal and cardiothoracic.
Inferior Venacava Filter
The IVC filter prevents a pulmonary embolism from developing by “trapping” a migrating DVT before it can enter a lung.
The IVC filter will not prevent development of deep vein thromboses.
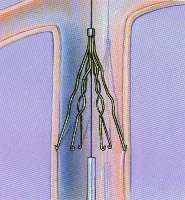
IVC Filter
Use of IVC Filters Prophylactically to Prevent Pulmonary Embolism
“We are doing this more and more in patients who are at very high risk for DVT (such as obese patients) or those who cannot be adequately anti-coagulated,” says Seyed-Mojtaba (Moji) Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Some patients, such as trauma, are at high risk for dangerous internal bleeding if put on blood thinners.
“These filters are retrievable and would prevent a PE if they were to develop a DVT. Once they have recovered, the filter can be removed.”
Placement of the IVC filter for high risk patients has been the medical standard for years.
For example, a patient undergoing hip replacement may have a genetic blood clotting disorder that puts that person at high risk for a DVT even in normal everyday life. Such a patient would get the IVC filter.
However, placement of IVC filters is not the norm, not the standard, for the typical patient — one who does not have a high risk for DVT outside of what risk the surgery will bring on.
But such patients are not immune to DVT, and many indeed develop a blood clot that then becomes a pulmonary embolism.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Heart Attack after Normal Stress Test: How Does this Happen?

Yes, a person can have a normal stress test but a heart attack shortly after, says a cardiologist.
Ever wonder if you can have normal stress test results, then suffer a heart attack soon afterwards?
It can happen, says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.

Plaque buildup in artery. Shutterstock/Explode
Dr. Sayeed explains, “A stress test can miss blockages that are less than 50% of coronary artery luminal diameter because they may not cause enough compromise in blood flow to be detected on a stress test.
“But it is these less severe blockages that tend to be more unstable and prone to rupture, causing a sudden heart attack when they do rupture, such as in the setting of vigorous exercise–snow shoveling.”
The reason these are more unstable is because when plaque buildup is less than 50 percent, it hasn’t been around long enough to harden.
Soft plaque is prone to breaking off in tiny fragments, and those fragments can obstruct a coronary artery, causing a heart attack by preventing blood flow to the portion of the heart that the affected artery feeds.
Strenuous exercise can cause the soft plaque to rupture in a person who’s not accustomed to strenuous activity such as shoveling snow.
This can explain why a seemingly “healthy” person literally drops from a heart attack while shoveling snow.
You may be thinking, Gee, if blockage under 50 percent can be so harmful, maybe I should eat up the cheeseburgers and fries to get that percentage up to like 80 percent.
But Dr. Sayeed points out, “No, what this means is that in some people, whether they have mild or severe blockages, if the plaque is soft, meaning it has not been around long enough to become calcified — natural response by the body — the soft plaques tend to be more susceptible to rupture or erosion compared to a hardened calcified plaque that is slightly more stable.”
To learn how much of your coronary arteries have calcified, get a coronary calcium score test.
“The higher percentage plaques tend to be more calcified because they have been around longer and have been increasing in severity over time, and have become calcified and remodeled and more stable over time if the person never had a plaque rupture and heart attack.
“This can occur in those with silent coronary artery disease where the plaques slowly develop, become calcified over years and the person is just lucky they never had an event.
“And they only develop symptoms once these calcified severe lesions block blood flow enough to cause symptoms such as chest pain.
“This is usually in someone who is pretty well-conditioned and healthy but had risk factors.”
This doesn’t mean that a very high coronary calcium score means you’re safe from a heart attack.
Dr. Sayeed adds that in general, smokers won’t last long enough for their coronary artery plaque buildup to reach a severely calcified state “because the cigarette smoke will cause a soft plaque to rupture.”
He also explains that “heart attacks can occur from other types of plaque pathology such as plaque erosion, not just rupture from a plaque that may not be detected on a stress test.”
What percentage of people, after being told their stress test was normal, have a heart attack soon after?
Dr. Sayeed says, “Hard to say what the percentage is, but probably around 5-10% depending on the sensitivity and specificity of the stress test that was performed.”

Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Andrey_Popov
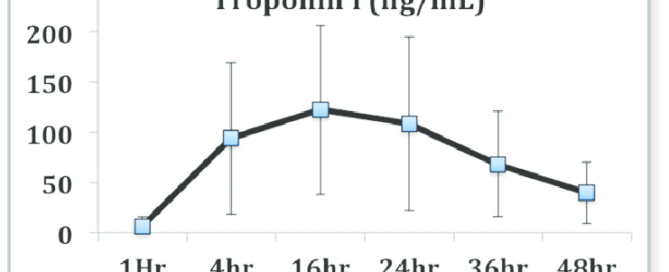
Can Troponin Elevation Mean Something Other than Heart Attack?

Patients who present in the emergency room with chest pain are given a troponin test (blood sample is taken by nurse).
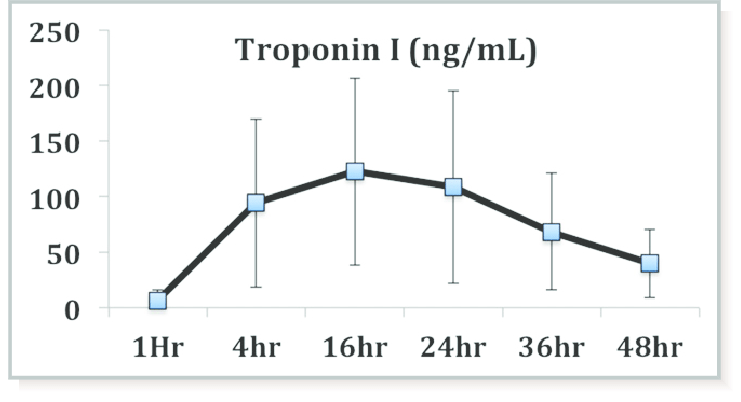
Troponin is a protein enzyme that leaks from the heart when this muscle is damaged.
If the test result is elevated (in a range that indicates damage to heart tissue), this can mean that the patient had a heart attack very recently.
However, elevated troponin doesn’t always mean cardiac damage.
In fact, the test result isn’t either normal or elevated; there is another range — an in-between range.
It’s sometimes referred to as a gray area or indeterminate area, which (along with elevated status) warrants a follow-up blood draw several hours later to see if the result is of a higher value (meaning that even more troponin has leaked from the heart).
If elevated troponin doesn’t always mean damage to the heart, what else might it mean?
“It can mean a long list of non-cardiac things, the most common being from renal failure, heart failure, pulmonary embolus, cardiac contusion, sepsis, cardiotoxins, CNS disorders, excessive exercise,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Generally, with modern assays and automated laboratory systems, troponin results can be returned within a few hours, often between one to three hours after the sample is taken.
Some rapid tests and point-of-care systems can provide results in as little as 20 to 60 minutes.
Other causes of elevated troponin not related to the heart muscle include:
1 High blood pressure (hypertension)
2 Drug toxicity
3 Low thyroid (hypothyroidism)
4 Rheumatoid arthritis
5 Transient ischemic attack and stroke
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
‘
Top image: Shutterstock/designer491
Source: nzma.org.nz/journal
Does Zero Calcium Score Always Mean Clear Arteries?
If your calcium score is ZERO, how confident should you feel about not having heart disease, and having nice clean arteries?
Did you recently get your coronary calcium score measured and it was zero, but you’re wondering if this absolutely for SURE means you have crystal clear arteries?
“It may not mean totally clear arteries,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“There may be some very mild plaques that are essentially clinically insignificant and are not calcified enough to be detected on the calcium score,” continues Dr. Sayeed. “Technically it does mean clear arteries in the big scheme.”
How to Help Prevent Clogging of Your Coronary Arteries
So if you are concerned that you may still have some mild heart disease or not perfectly clear arteries despite having a coronary calcium score of zero, there are several things you can do to dramatically reduce the risk of eventually developing significant levels of coronary heart disease.
AVOID TRANS FATS AT ALL COSTS.
While consuming trans fats a few times a month might not seem harmful, it’s crucial to ensure that this frequency doesn’t escalate to a few times a week.
Even occasional consumption can add up over time, leading to significant trans fat intake over a decade.
Since there is no definitive data on the long-term risks associated with occasional trans fat consumption, it’s prudent to err on the side of caution.
To protect your health, it’s best to avoid trans fats altogether and focus on a diet rich in healthier fats, such as those from nuts, seeds and fish.
LIMIT PROCESSED FOODS (even if they don’t contain trans fats) as much as you can.
Make a homemade chicken pot pie; forget Marie Callender’s.
To limit processed foods, focus on preparing fresh, whole foods at home.
Choose fruits, vegetables, lean proteins and whole grains. Read ingredient labels carefully to avoid hidden sugars, unhealthy fats and additives.
Plan meals ahead of time and cook in batches to reduce the temptation of convenience foods.
Gradually replace processed snacks with healthier alternatives like nuts, yogurt and fresh fruit.
Replace bottled juice with whole fruit.
There are numerous other ways to protect against developing coronary artery plaque buildup and maintaining clean arteries and keeping your calcium score at zero.
These include taking the supplements of green tea extract, turmeric, garlic and krill oil, and eating omega-3-rich fish several times a week.
Fish offers numerous benefits, including reducing inflammation, improving heart health by lowering blood pressure and cholesterol levels, supporting brain function and enhancing joint health.
It can also contribute to better mood and cognitive function.
And finally, DO HIGH INTENSITY INTERVAL TRAINING.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Why Does Anxiety Cause Premature Ventricular Contractions?

Anxiety can cause PVCs (premature ventricular contractions), especially if you have anxiety over PVCs.
But just how does this happen; what is the mechanism?
“Anxiety causes increased stimulation of beta receptors on the heart, which can cause increased heart rate and cause other parts of the ventricle to have electrical impulse formation (PVCs) due to increased beta agonism,” explains Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Beta receptors are located on the cells of the heart. They are part of the physiological response that occurs when a person suffers from anxiety or stress.
Beta receptors are part of the sympathetic nervous system; this is the system that causes changes in the body to prepare it for a fight or flight (e.g., heightened senses, increased respiration, rapid heart rate).
So amid these physiological changes, the ventricles of the heart may end up not quite pumping in perfect rhythm.
“Beta agonisms” simply means that the beta cells are stimulated or activated.
You can get PVCs simply by worrying about them.
Just like sometimes muscles will begin twitching when a person with health anxiety begins fretting about twitching muscles, one’s heartbeat will start feeling jumpy or like there’s an extra or skipped beat — simply due to the anxiety that comes with worrying about this.
For the typical person, the biggest problem that premature ventricular contractions present is the way they feel.
Nobody likes to feel a fluttery or erratic type of beating in their chest. This is called cardiac awareness. And it is not easily ignored.
However, PVCs are rarely a significant issue or something that a cardiologist will worry about.
PVCs can occur in healthy hearts. Most cause no symptoms, don’t impair heart function and don’t increase risk of cardiovascular issues unless they are linked to structural heart disease.
In a heart with clogged arteries, PVCs are more relevant to your cardiologist.
The duo of premature ventricular contractions and plaque buildup in the coronary arteries can mean a higher risk for irritated heart muscle, reduced heart pumping ability or the development of an arrhythmia.
Cardiologists evaluate heart flutters in the context of patient history and any co-occurring conditions.
Your doctor will be concerned with any other symptoms with the premature ventricular contractions such as shortness of breath, chest pain, undue fatigue, dizziness, nausea or fainting spells.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Y Photo Studio

Can PVCs Be Caused By Seasonal Allergies?

A cardiologist addresses whether or not premature ventricular contractions can be caused by seasonal allergies.
Many people who have PVCs want to know if seasonal allergies can cause this sometimes very disturbing symptom.
“This would be quite rare, and only if the allergies really caused a lot of stress and anxiety and excessive adrenaline release from a more severe allergy,” explains Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
PVCs can have a bark that’s bigger than their bite, which is why individuals who experience these can become quite alarmed.
Seasonal allergies are far more likely to cause headaches than premature ventricular contractions.
If you’ve been experiencing “cardiac awareness,” then you need to have a thorough checkup by a cardiologist.
They may then recommend additional testing that you’d need to make an appointment for.
Do not let all of this frighten you; multiple tests are modern medicine at work to help find the root causes of troubling symptoms.
Tests that turn out normal will give you substantial reassurance that you have a healthy heart.
PVCs may be relevant in people who have heart disease, but even then, this association has not been clearly defined by research.
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can Angina Cause Vomiting?

Find out why angina can cause vomiting.
Angina is a condition in which insufficient blood flow occurs in the heart due to narrowing of the coronary arteries from disease (plaque buildup), and hallmark symptoms are chest pain and shortness of breath.
However, angina can also cause vomiting.
In fact, vomiting can signal an imminent heart attack (more on this shortly).
“Angina, especially if severe, can cause excessive stimulation of the autonomic nervous system leading to vomiting,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
“The anginal vomiting would likely be accompanied by some other anginal equivalent such as excessive sweating or shortness of breath or chest pain,” continues Dr. Sayeed.
A few days before my mother was diagnosed with unstable angina, she upchucked.
That same morning she had an alarming episode of difficulty breathing.
Two days later (after being diagnosed with unstable angina) she had emergency quintuple bypass surgery and had been days away from a massive heart attack, said three doctors.
The day prior to the symptoms, she had not eaten anything unusual; why was she upchucking?
This was so unlike her. I quickly connected the dots: difficulty breathing plus vomiting, although mild — an imminent heart attack!
Usually, vomiting signals a benign cause, such as a bad food source or substantial anxiety.
Dr. Sayeed explains, “In some cases, it may be hard to differentiate from bad food or anxiety, but in general, the patient would likely have risk factors for angina or a prior history of heart disease.
Anxiety and bad food would be short-lived causes, while the vomiting from angina could occur with each episode and perhaps persist until the underlying problem was fixed.”
Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}