

Mole with White Spot in Center

Find out what it could mean if a mole has a white spot in it.
I have a mole that has a white (or actually, flesh or cream colored; it’s hard to tell) spot kind of in the center of it.
I’ve been aware of this for several years since I began doing exams of my skin.
My primary dermatologist wondered if it had always been there and examined it more closely with a dermatoscope.
When I said it had always been there since I began doing skin exams, she didn’t seem concerned, but she pointed out that she thought it appeared to be an area of missing pigment.
She then said it could be a hair follicle.
When pigment appears to go missing is what can be of concern. What appears to be missing pigment could actually be a change in the color of a portion of a mole.
Shortly after seeing my primary dermatologist, I visited a second dermatology office where I get my serial digital dermoscopy done; I was due for another annual visit.
The dermatology resident said it was a hair follicle after I asked him what the “white spot” in my mole was.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Image Point Fr
What if You Get a DVT While on Coumadin (Warfarin)?
Is it possible for someone to get a deep vein thrombosis while on the blood thinner coumadin (Warfarin), and if so, why?
This is a prescription drug that’s so effective at thinning blood, that it carries the risk of internal bleeding, including in the brain.
Once a definitive diagnosis is made, the patient is placed on anticoagulation, which typically is that of coumadin (Warfarin), says Dr. Kurtis Kim, MD, a vascular surgeon with Vein & Vascular Institute of Central Maryland.
A common reason for being placed on a blood thinner is to help prevent DVT as a result of surgery, particularly joint replacement.
Joint replacement surgery is notorious for heightening the risk of a blood clot.
Abdominal surgery is another type of operation that will put the patient at high risk for a deep vein thrombosis.
Dr. Kim explains that a “very small percentage of people who develop DVT” are on a blood thinner.
And when this does happen, “one must ask the following questions:
#1) Is this patient compliant with this medication?” and
#2) “Is the medication at a therapeutic level (for example coumadin needs to be dosed to achieve an INR of 2-3).”
The third check is to review other risk factors for a deep vein thrombosis.
INR stands for international normalized ratio. It’s a numerical value that correlates to how long it takes the blood to clot. The higher the number, the longer it takes.
The first time someone takes coumadin, the INR will not be in the therapeutic (or DVT prevention) range.
It has to build up. And it fluctuates, which is why when someone is prescribed coumadin to take for a while, they must have regular blood draws to make sure that the INR is within therapeutic range.
After my father fell and hit his head, resulting in neurological symptoms, the doctor reduced the coumadin dose to bring the INR down to 1.5.
He had had knee replacement surgery a week prior, and the fall resulted from passing out — for reasons that still remain somewhat of a mystery, though the best theory is that his blood pressure had plummeted as a result of drug interactions.
The INR was dropped to 1.5 because he was at risk for having a brain bleed from the fall.
However, after he was released from the hospital, the doctor increased the coumadin dose and the targeted INR.
Coumadin is very effective at DVT prevention, but it’s not 100 percent guaranteed to prevent a deep vein thrombosis.
 Specializing in minimally invasive procedures, Dr. Kim combines medical expertise with a caring approach to diagnose and treat patients with circulatory issues including leg pain, swelling and blood clots in the legs and lungs.
Specializing in minimally invasive procedures, Dr. Kim combines medical expertise with a caring approach to diagnose and treat patients with circulatory issues including leg pain, swelling and blood clots in the legs and lungs.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
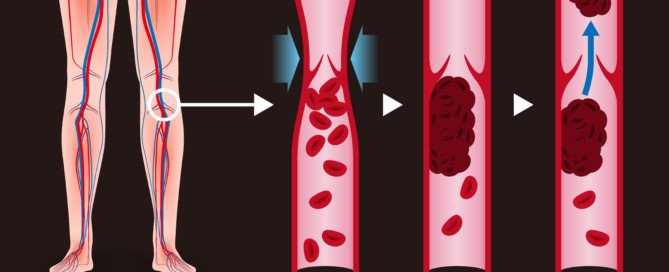
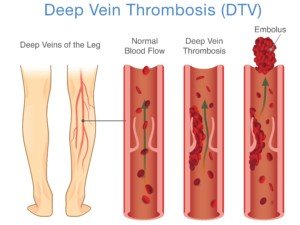
Number of DVTs Missed by Ultrasound
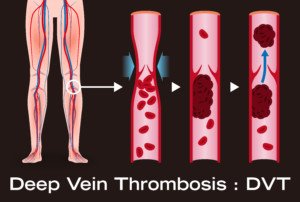
Ultrasound (Doppler scan) is not 100 percent effective at detecting a deep vein thrombosis, a life-threatening blood clot that can dislodge and travel to the lungs and be fatal.
Percentage of DVT’s Missed by Ultrasound
“Sensitivity and specificity of ultrasound detecting DVT in the leg above the knee is 97% and 94%, respectively, meaning, while they are very accurate, it can miss it,” explains Dr. Kurtis Kim, MD, a vascular surgeon with Vein & Vascular Institute of Central Maryland.
Dr. Kim continues, “This stresses the importance of seeing a specialist, as at times, even with negative ultrasound, physicians initiate anticoagulation due to strong clinical suspicion.”
If a physician suspects a deep vein thrombosis – even in the absence of a positive ultrasound result – the doctor will prescribe anticoagulant medication (blood thinners).
What would make a doctor suspect a DVT if the ultrasound is negative?
The physician knows that the ultrasound will, on average, miss a very small percentage of deep vein thromboses detection. But what brought the patient into the exam room in the first place?
Suppose both the patient’s legs are swollen. There is no pain or redness. A week prior the patient had back surgery and reports that for the past week he’s been doing way more sitting than usual.
The ultrasound of his legs is negative; no apparent DVT.
A doctor won’t have a high suspicion of a blood clot due to this patient’s presentation and medical history.
The suspicion for DVT when both legs are swollen equally isn’t very high, especially since excessive sitting (such as that can occur after back surgery) can cause edema or fluid retention in the legs.
But if a patient presents with only one leg newly swollen, and it has a reddish color, and the calf area hurts regardless of activity or rest – the doctor will suspect a deep vein thrombosis even if the ultrasound is negative.
“Unlike CT or X-ray, accuracy of ultrasound is highly operator-dependent, so finding a good vascular specialist and associated vascular lab is important,” says Dr. Kim.
Specializing in minimally invasive procedures, Dr. Kim combines medical expertise with a caring approach to diagnose and treat patients with circulatory issues including leg pain, swelling and blood clots in the legs and lungs.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Artemida-psy

How Do Stockings Prevent Blood Clots after Surgery?

Are you scheduled for surgery and are wondering why you’ll need to wear stockings?
These help prevent blood clots, which can travel to the lungs and be fatal.
The stockings are actually called TED hose. TED is an acronym that stands for thromboembolism deterrant.
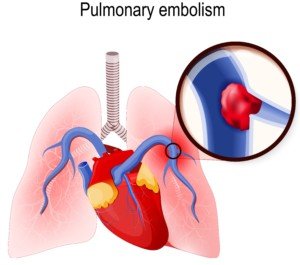
A thromboembolism is the term referred to deep vein thromboses (blood clots) that can travel to the lungs and become a pulmonary embolism.
“Many data support the use of TED hose but has not shown to prevent postoperative DVT on its own,” says Dr. Kurtis Kim, MD, a vascular surgeon with Vein & Vascular Institute of Central Maryland.
“Depending on the situation (how big the surgery was, how immobile the patient was prior to, does this surgery limit patient ambulation, prior history of DVT, age, ongoing medical issues, etc.), some are placed on prophylactic anticoagulation or placement of inferior vena cava [filter] due to significant predictable risk.”
Anticoagulation refers to blood thinners. The IVC filter is placed in the IVC vein to trap any broken-off DVT fragments that are traveling towards the lungs — like a net catching fish.
“Same orthopedic surgery can pose high risk for patients who has limited mobility already with prior history of DVT vs. 40 year old athlete who is walking out of the hospital,” says Dr. Kim.
“While more standardized treatment guidelines seem ideal, individually tailored treatment is far more important.”
If you’re scheduled for joint replacement surgery or any major surgery for that matter, be sure to discuss DVT prevention with your surgeon.
This includes asking questions about the use of TED hose or “stockings.”
Deep vein thromboses are common, and the postoperative period is one of the riskiest times for these blood clots to form.
After surgery, especially for procedures involving the legs or pelvis, patients are at increased risk for DVT due to reduced mobility, changes in blood flow and potential damage to blood vessels.
During recovery, prolonged periods of immobility or bed rest can contribute to blood pooling in the veins, which raises the risk of clot formation.
Symptoms of a Deep Vein Thrombosis
Though about half of all people with a DVT will not have symptoms, this condition is responsible for the following classic signs:
- A portion of the leg is reddish/pink.
- The area of discoloration is swollen.
- The area may also be unusually warm to the touch — warmer than the surrounding normal areas of skin or the same area on the opposite leg.
- Cramping or pain in the lower leg or behind the knee. This cramping does not correlate to movement.
Though TED hose may be part of the postoperative prevention plan for a DVT, blood thinners and pneumatic compression (leg wrap device) are far more effective.
Specializing in minimally invasive procedures, Dr. Kim combines medical expertise with a caring approach to diagnose and treat patients with circulatory issues including leg pain, swelling and blood clots in the legs and lungs.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: James Heilman, MD, CreativeCommons

Acute Subdural Hematoma WITH Pulmonary Embolism!

How is a patient treated if presenting simultaneously with an acute subdural hematoma AND a massive pulmonary embolism?
Can anything be more vexing?
For example, a patient arrives at the emergency room from a motor vehicle accident, with a suspected acute subdural hematoma, but is also showing signs of a massive pulmonary embolism.
Yes, it’s possible. The massive pulmonary embolism wouldn’t necessarily arise from the vehicular accident.
For all we know, the patient had recent knee replacement surgery; or is a smoker on birth control pills; or is obese who very recently ended a long airplane flight—all risk factors for a DVT — which can break apart and lead to a pulmonary embolism.
An acute (not chronic) subdural hematoma is a life-threatening situation that requires immediate surgical intervention.
A massive pulmonary embolism also is life-threatening and must be treated immediately. Both conditions are confirmed with a CAT scan.
However…the treatments are polar opposites!
Give a blood thinner to a person whose brain is bleeding from an acute subdural hematoma, and this will intensify the hemorrhaging.
But if the acute subdural hematoma is treated before the pulmonary embolism is, the PE could kill the patient while the craniectomy is being performed.
What a Vascular Surgeon Says
“You’re describing a patient in severe duress with significant neurologic changes and near-hemodynamic collapse,” begins Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
“These always have to be looked at on a case by case basis, so it is impossible to say what I would do, but the issues would be this: relieving the SDH and restoration of blood flow to the pulmonary artery which is causing the hemodynamic instability.
“If pressors alone were not alleviating this, then the possibility of mechanical thrombolysis (removing the clot from either an endovascular or open surgical technique without the use of systemic anticoagulation) exists and may be the best option.”
- Pressors: medications that increase blood pressure and/or cardiac function, says Dr. Casey.
- Systemic anticoagulation: blood thinner given intravenously; it will circulate throughout entire body, including the brain.
But which doctor (neurosurgeon or vascular surgeon/interventional radiologist) should “go first”?
“It is unlikely that a neurosurgeon would be doing a craniotomy (relieving the bleed in the skull) while anyone else would be doing an angiogram or sternotomy (cracking the chest) at the exact same time.”
A massive pulmonary embolism can require cracking of the chest for access to the lungs.
“Perhaps it has been described in the literature, but it is not common and I’ve never seen or been a part of that combined approach,” says Dr. Casey
Simultaneous pulmonary embolism and acute subdural hematoma would be nothing less than agonizing for doctors to be faced with.
Shutterstock/Designua
 Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ALPA PROD

DVT and Chronic Subdural Hematoma at the Same Time?

How would a patient with both deep vein thrombosis and chronic subdural hematoma be treated?
Now, I don’t mean someone who develops a chronic subdural hematoma from the Coumadin (Warfarin) they were prescribed to treat a DVT.
Rather, I mean a new-onset deep vein thrombosis which is unrelated to the symptomatic chronic subdural hematoma.
The patient has risk factors for DVT, such as smoking, lack of exercise, pregnancy or being on birth control pills, a recent joint replacement surgery and recent prolonged air travel.
The chronic subdural hematoma developed as a result of slipping on ice several weeks prior and hitting the head against concrete.
“These types of clinical situations require a close discussion between the doctors,” says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
“This patient would likely be a good candidate for an (inferior vena cava) IVC filter. This is a small ‘umbrella’-like device which is placed in the IVC.”
The filter “does not prevent the development or propagation of DVTs, but it prevents them from traveling to the lungs and becoming a PE.”
Think of a fish net trapping fish.The IVC is a large vein that leads into the heart.
“An indication for an IVC filter is a contraindication to anticoagulation (as this patient likely would be), allergy to anticoagulation, or development of a new VTE while on therapeutic anticoagulation.”
A chronic subdural hematoma is slow bleeding in the brain, usually caused by impact to the head that creates small tears in the bridging veins near the skull.
It can take up to 12 weeks before symptoms begin appearing, due to the slow nature of the bleeding.
Anticoagulation (anti-clotting) drugs would thin out the blood, which in turn would amplify the bleeding in the brain.
My mother had a DVT and a chronic subdural hematoma — about two and a half months apart, but they could have been concurrent, simply because there had been no reason why they could not have been concurrent. She was lucky in that respect.
What about pulmonary embolism simultaneous with chronic subdural hematoma?
Simultaneous with a chronic subdural hematoma (not acute) — one that’s generating symptoms such as a “crown of thorns” headache, weakness on one side of the body and changes in cognition.
As for the course of treatment for this kind of situation, Dr. Casey explains: “Again, we would have to have a very close discussion about the best options for this patient.
“However, I think that an IVC filter may also serve this patient best.”
The IVC filter would prevent any additional PEs, but would not dissolve the PE that’s already there.
Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rocketclips, Inc.

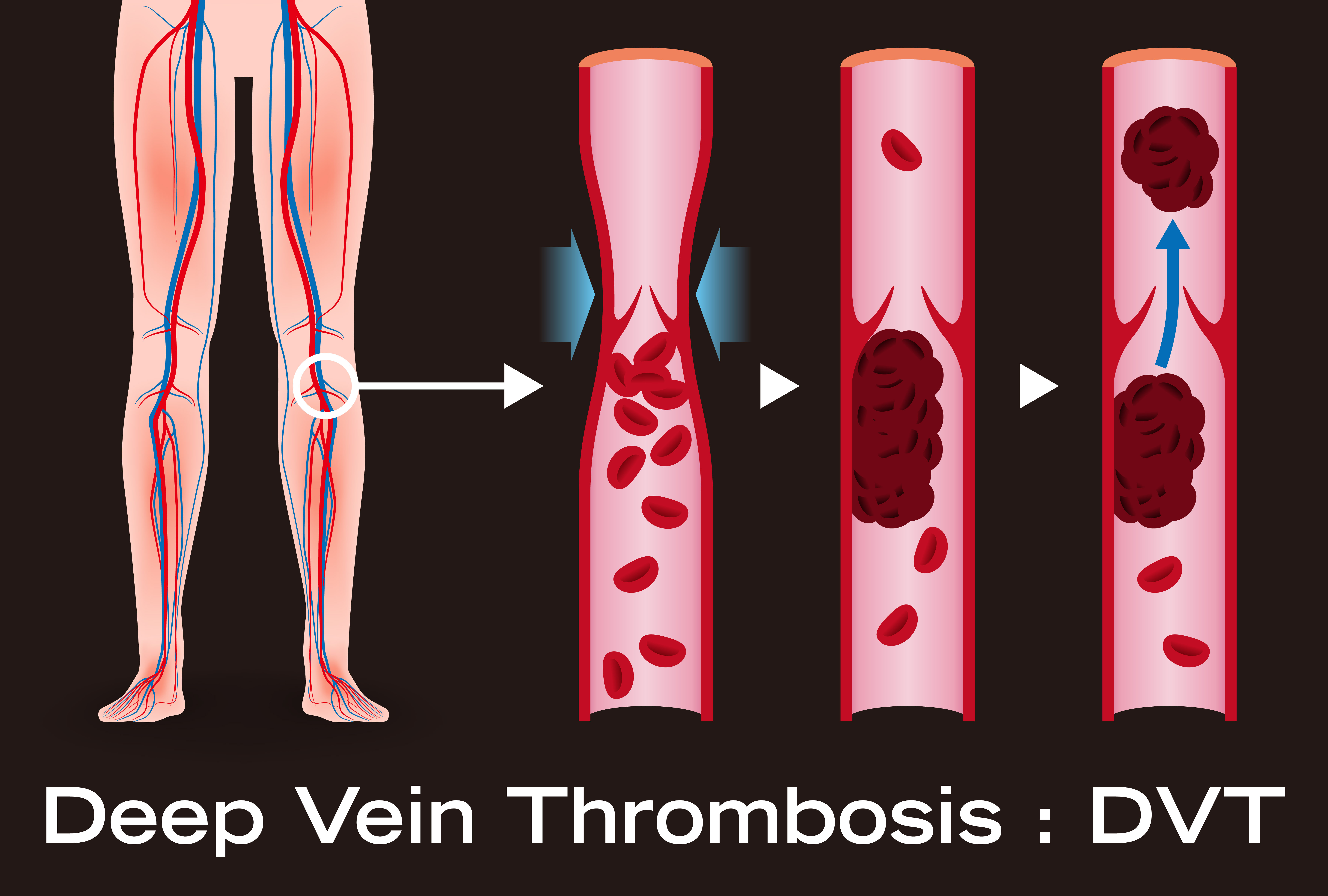
One Calf Swollen, Hurts, Red: Possible Causes

A doctor points out many possible causes (some very serious!) of swelling, pain and redness in just one calf.
If a calf is swollen, red and painful (hurts, aches, or feels crampy), especially if there’s no explanation such as a traumatic injury or snake bite, this could mean a deep vein thrombosis (DVT).
This is actually the first thing an ER doctor will suspect if someone with these symptoms is seen in the emergency room.
An ultrasound will be ordered to check for a DVT, but there are times when a DVT is missed.
Making things even trickier is that “a large portion of patients with an acute DVT don’t present with unilateral calf swelling, pain and redness,” says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
Swelling, Pain and Redness in a Calf not the Only Symptoms of DVT
“Clinical manifestations are variable,” says Dr. Casey, “and range from absence of symptoms to massive pitting edema and blanching (a condition called phlegmasia cerulea dolens which is a surgical emergency with a high risk for limb loss).”
Edema is fluid buildup that causes swelling.
Pitting means that if you press on the swollen area with a fingertip or, say, eraser-tip of a pencil, it will leave an obvious indentation that will take longer than five seconds (sometimes up to a few minutes) to vanish.
However, pitting edema doesn’t necessarily mean DVT.
Other DVT Signs
“Signs and symptoms include pain, edema, erythema, tenderness, fever, a Homan’s sign (pain with passive dorsiflexion of the foot), peripheral cyanosis or prominent superficial veins,” says Dr. Casey.
Dorsiflexion is the ankle joint motion of flexing the foot upward.
“Up to 50% of patients with DVT, however, may lack any specific signs or symptoms.”
What else can swelling, pain and redness in one calf mean?
“The differential is broad and includes muscle strain or tear, Achilles tendonitis, soft tissue trauma/injury, superficial thrombophlebitis, symptomatic varicose veins, lymphedema, arthritis, stress fracture, peripheral arterial disease, renal failure, hepatic disease, heart failure,” says Dr. Casey.
You’ll likely have a memory of an extraneous insult for at least a few of these issues, such as muscle strain or tear, and stress fracture.
If you have kidney, liver or heart failure, you’ll very likely have other troubling symptoms of these conditions.
Blood tests can reveal presence of disease in these organs.
Pain, redness and swelling, especially in one calf, warrants immediate evaluation by a doctor!
Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Joyseulay

TED Hose for Post-op DVT Prevention: The Truth

A surgeon presents easy-to-understand information about TED hose and post-operative DVT prevention.
My father has had, in total, four joint replacement surgeries — a big risk factor for DVT development.
In his case, the perspective on TED hose for helping prevent a deep vein thrombosis varied from surgeon to surgeon, nurse to nurse.
Gee, I wondered, is TED hose very effective or not?
Why did some medical professionals take this tool very seriously, and others weren’t too attentive to it or didn’t seem to put a lot of stock in it?
I also observed mixed perspectives on TED hose regarding my mother’s illnesses that rendered her to a lot of bed rest.
“Mechanical prophylaxis has not been studied as extensively as chemical prophylaxis in the prevention of DVT,” says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
Mechanical prophylaxis refers to non-pharmaceutical preventive aides for DVT. Chemical refers to medications.
“However, they may be the only treatment option for those patients in whom chemical prophylaxis is contraindicated,” says Dr. Casey.
“In addition, many of the studies combine both, rather than examine solely, the graduated compression stockings (e.g., TED hose). This may be why there is some confusion on the matter.
“Graduated compression stockings are effective in DVT prevention. The most notable recent study was a meta-analysis of seven randomized controlled trials which showed a cumulative post-operative DVT reduction, from 29% in the control group to 15% in the compression group.”
In addition to the TED hose…
“I am an equally strong advocate of intermittent pneumatic compression while my patients are in the hospital,” Dr. Casey explains.
“These have also been shown to have an extremely successful reduction in the incidence of DVTs in post-operative patients.
“Unlike stockings, they have a decreased risk of skin breakdown and irritation. Of course, they cannot be used at home.”
Warning: Make sure the nurse or nurse assistant turns back on the IPC device after accompanying the patient to the restroom or taking the patient out into the hall for some walking exercise!
More than once, I noticed that the IPC device was NOT on after my father or mother was returned to their bed!
“The DVT risk does extend beyond the post-operative period,” says Dr. Casey.
“Of course, once the patient leaves the hospital, all doctors encourage them to ambulate as much as possible, certainly at least three times per day. Ambulation is very important in the prevention of DVT.”
My father was instructed to wear the TED hose overnight for several weeks after he got home from his first knee replacement surgery.
For the third surgery, he was told he didn’t have to wear them once he got home!
Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: hutterstock/Lentpjuve

How Accurate Are Doppler Scans for a DVT?

This article is about the effectiveness of Doppler scans (ultrasounds) in detecting a deep vein thrombosis.
I once read of a woman whose inner left thigh was red, swollen and painful; Doppler (ultrasound) was negative, but 11 days later a CT scan (which emits radiation) showed completely clotted veins!
Can a DVT be missed by a Doppler scan?
“ABSOLUTELY,” says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
“I will start by saying that rarely is a test ever 100% accurate. The great aspect about ultrasound is that it is noninvasive, easily obtainable, reproducible and relatively inexpensive.
“However, the drawbacks to an ultrasound are that it is heavily technician-dependent, can be difficult in patients with a challenging body habitus (namely, obesity).
“Having said that, the sensitivity and specificity of duplex ultrasonography in the diagnosis of acute DVT is around 95% and 98%, respectively.”

Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Boyloso

How Long Does It Take DVT to Form from Bed Rest?

Dr. Kevin Casey explains the time lapse for DVT to form from bed rest.
How long might it take for a deep vein thrombosis to develop as a result of excessive bed rest?
“This is a little bit difficult to answer, but I will tell you that it is not long,” says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
“Our bodies are constantly in flux with changing hormones, cytokines and inflammatory markers.
“Under normal conditions the endothelium (vessel lining) provides a vasodilatory fibrinolytic environment.”
Vasodilatory fibrinolytic means suppression of clotting factors via dilation of blood vessels.
Dr. Casey continues, “This prevents coagulation [clotting], platelet adhesion, inflammation and clot formation.
“However, during states of disturbance of the endothelium, a cascade of prothrombotic [pro-clotting] and pro-inflammatory states occur, which can set the stage for amplification of the thrombotic process. Inflammation and thrombosis are interrelated.”
Why don’t we get blood clots in our sleep?
“Depending on the other factors simultaneously occurring in a patient (i.e., major trauma, hypercoagulable state from malignancy, etc.), a DVT can form very quickly.

James Heilman, MD, CreativeCommons
“However, an average person lying in bed for two hours will usually not encounter this problem.”
A healthy person who has not had recent surgery or who does not have other risk factors for DVT such as being a smoker who’s on birth control pills, will not develop a DVT simply from sleeping overnight, seemingly immobilized for many hours.
- The body actually moves during sleep in minute ways.
- Muscles are innervated.
- Subtle shifting occurs.
Air pressure is normal (as opposed to the cabin pressure in an airplane, which some experts believe contributes to increased DVT risk while on long flights).
Normal-length sleep is a required physiological process and thus, does not predispose one to a deep vein thrombosis.
Shutterstock/solar22
If you develop a DVT from excessive bed rest, while still in bed, can getting up and about dissolve the clot?
“Possible, yes; likely, no,” says Dr. Casey. “‘Getting up’ or ambulation doesn’t dissolve the clot. But it will begin to release enzymes which prevent the pro-inflammatory state and propagation of the clot.
“Your body may either slowly dissolve or stabilize the clot after that.”


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}