

Sudden Brief Pain at the End of Sternum: Possible Cause

Sudden brief “dings” of pain that occur in the divot at the bottom of the sternum might have a benign cause.
I can only speak from my experience, but it’s very fair to conclude that the cause of the brief “dings” of pain in that little divot between my breasts, at the bottom of the breastbone, had a musculoskeletal cause.
When you experience interesting sensations of pain or aching, you should record when this happens and anything that might have occurred that day or the day prior, so that over time, if these events keep recurring, you’ll maybe be able to see a pattern.
I began having the short sudden pain at the end of my breastbone, and had not recollected that I had documentation of this going back more than three years.
There were only a handful of notations in my health log, but as I did a “search and find” on the keyword divot, several entries popped up in the log.
The description was the same for all the entries, and there was such a long time lapse between them and my most recent episodes, that I had no choice but to conclude that it was the same benign cause.
However, I had not established a pattern for the previous incidents.
But this time, I did. It came from doing narrow to medium grip pull-downs at the gym on the “lat machine.” There was a correlation.
It seemed that whenever I had this divot pain at the end of my sternum — either earlier that day or the day before, I had done pull-downs.
The clincher came when about 40 minutes after doing pull-downs, when I was in the grocery store next door to the gym, I got sudden dings in the divot.
But why would this be happening when I’ve been lifting weights for most of my life? Well, that’s just how the musculoskeletal system sometimes behaves.
Another consideration is that I had NOT been doing any kind of pull-downs (let alone chin-ups and pull-ups) for a very long time, due to tendonitis in my elbow. So I was just getting back into heavier pull-downs.
As the tendonitis has been clearing up, I’ve been increasing the resistance on the pull-downs.
I’m able to deadlift quite a bit, but my rehab isn’t complete when the pulling is done from above my head.
If you’ve been experiencing sudden brief episodes of pain (it wasn’t stabbing or sharp; I’d call it more like a strong ache) right at the divot that’s located at the bottom of your breastbone, document when this occurs and what exercises you’ve been doing recently to see if a pattern shows up.
This isn’t about a diagnosis. It’s about documentation and seeing if an association or pattern emerges over time. This can help you should you decide to see a doctor.
If you’re dumbfounded and/or the pain gets worse or more prolonged, do see a doctor.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/ShotPrime Studio
Mole Shave Biopsy on Lower Leg Healing Time
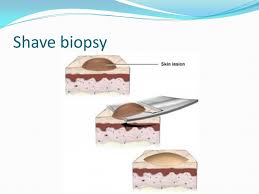
Find out how long it may take for a mole shave biopsy on your lower leg to heal.
I had a shave biopsy on my lower leg for a mole that I was concerned about (it turned out to be harmless; benign).
Sixty days later the scab was still on it and still did not look like it was ready to naturally fall off (never pick off a scab!).
It looked as though if I picked the scab off, it would bleed beneath, because it appeared that the scab was filling in a depression.
The next time I looked at the site (73 days out from procedure), which was on the front part of my upper shin, the scab was gone, and what remained was a dry, pink, very slightly depressed area.
For at least two weeks after the shave biopsy for the mole, the site still did not appear that it was healing much. It had a fresh look about it, almost raw, moist.
I also kept a Band-Aid on it all day and overnight, changing it every three to four days because every time I changed it, it seemed as though the bandage part of the Band-Aid would lift off minute particles from the site.
Finally, after three weeks, it looked like a scab was definitely beginning to form.
However, for the longest time, the site’s appearance seemed to be the same. I’d view it every three or four days when I removed the Band-Aid.
The shave biopsy for the mole either didn’t seem to be healing, or, it was healing so slowly that it was imperceptible to me.
But gradually over time, the forming-scab took on an increasingly dry, sturdy, browner appearance, and also very gradually seemed to be getting smaller.
Then it began getting a slightly crusty look—meaning that healing of the shave biopsy was continuing to progress.
“Lesions below the knee take longer to heal in everyone, particularly as we age,” says Adarsh Vijay Mudgil, MD, double board certified in dermatology and dermatopathology, and founder of Mudgil Dermatology in NY.
“The predominant reason is that circulation at the most distal parts of our body (namely below the knee) is not as robust as parts of the body more proximal to the heart; this fact intensifies as we age.”
Via e-mail, I asked my dermatologist, who performed the shave biopsy, if the fact that the Band-Aid had been covering the site for about four weeks before I decided to stop using Band-Aids, had slowed the healing time.
She said it did not slow the healing time, and in fact, it would have helped keep the site moist, which is important for optimal healing.
If you’re wondering when on earth the shaved area of your mole is going to heal…well…it may take nine and a half weeks for the scab to be ready to fall off.
 Dr. Mudgil treats infant to geriatric patients, and is versed in all aspects of medical, surgical and cosmetic dermatology. He has published extensively in the medical literature plus has lectured at numerous national meetings.
Dr. Mudgil treats infant to geriatric patients, and is versed in all aspects of medical, surgical and cosmetic dermatology. He has published extensively in the medical literature plus has lectured at numerous national meetings.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Life Span of Morbidly Obese vs. Normal Weight People

More truth shows that there’s no such thing as a healthy extremely obese individual and that obesity cuts life span SHORT.
People who are extremely obese (class III) are more likely to have a much shortened life span than are those of normal weight.
But there is no formula for determining exactly how many years — for any particular overweight person at a given weight, height and age — will be taken off their life span.
“I generally don’t get specific with my patients about how long they will live; there are too many variables to really answer a question like that,” says Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“I will tell them that their lifespan is likely shorter — as they are at risk to develop complications from morbid obesity over time — such as hypertension, diabetes, heart disease, liver disease and so on.”
Extreme obesity is referred to as class III, and it’s on the rise. It translates to being more than a hundred pounds over a person’s recommended weight range for their height.

A body mass index (BMI) of at least 40 is class III. “Normal” is 18.5 to 24.9.
Obesity Shortens Life Span: Study
This study comes from the National Cancer Institute, and the full report is in PLOS Medicine (July 8, 2014).
The NCI analyzed 20 studies that included adults from the U.S., Australia and Sweden.
The researchers eliminated smokers and subjects with a history of certain medical conditions to balance the results.
The risk of a shortened life span was looked at in over 9,500 subjects with extreme obesity and 304,000 who were at normal weight.
Findings
As BMI rose within the extreme obesity group, so did the risk of death overall, as well as death from most major diseases.
In the class III group, the prevalent causes of death were from cancer, heart disease and diabetes.
A BMI of 40 to 44.9 meant 6.5 years of life lost; a BMI of 55 to 59.9 meant 13.7 years lost.
Accuracy of the Study
Accuracy was contingent upon self-reported weight and height values (though if anything, this would suggest that the findings are even more alarming than they seem to be, since a person who weighs 255 pounds isn’t likely to inflate this number).
Use of BMI only, for the obesity measurement, also limits accuracy, though once BMI hits 40, you can be assured that this reflects obesity rather than a high degree of muscle mass.
It’s easy to see, without the medical research, why the people in the images above have a shortened lifespan due to their obesity.
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Image source: canweallgo.com
Source: sciencedaily.com/releases/2014/07/140708153902.htm

How Safe Are Hip & Knee Replacements for People Over 80?

Here’s what you need to know if you’re over 80 and wondering if it’s worth it to have a hip or knee replacement electively. How safe is it?
It’s one thing if an 80-plus person absolutely has to have a total hip or knee replacement due to an acute injury such as from a fall or motor vehicle accident.
But what about people over age 80 who are plagued by the pain of osteoarthritis in their joints and are wondering about the mortality rates of a hip or knee replacement?
“Studies seem to indicate that total joint replacement in the elderly, provided all factors regarding the patient’s health are similar, are really quite safe,” says Barbara Bergin, MD, board certified orthopedic surgeon at and co-founder of Texas Orthopedics, Sports & Rehabilitation Associates.
“There may be a slightly higher potential for post-operative complications, which would seem intuitively apparent,” continues Dr. Bergin.
“However, when compared to the benefits of improved quality of life, increased mobilization and reduced use of pain relievers, consideration of these operations in folks over 80 is becoming a reality.”
One such study is in the Journal of Bone and Joint Surgery (July 2014), affirming that these kinds of surgeries for people over 80 are generally safe.
This applies to patients with few to zero accompanying medical conditions.

“It is especially important when we also consider the aging population, as well as the activity of the elderly now, as compared to decades in the past,” says Dr. Bergin.
“It is harder to recover from a total knee replacement than a total hip replacement.
“We have to consider the rigors of rehabilitation and a patient’s ability to comply with a program when discussing total knee replacement.
“Dementia and overall physical disability certainly influence our decision to recommend surgery.
“Not so with total hip replacements. In fact, we frequently do basically the same operation for hip fractures [when compared to hip osteoarthritis] in the very elderly, and they do quite well. They’re able to bare weight and mobilize very quickly.
“My dad had his knee replaced when he was 79. He was golfing three months later. He is now 87 and still golfing a couple of times a week!”
The BJS study, which involved hundreds of thousands of patients spanning a number of years, showed that in people with no other medical conditions/diseases (comorbidities) or only a small number of comorbidities, the in-hospital complication rate decreased significantly for total knee replacement in patients over age 80.
However, the in-hospital complication rate for total hip replacement, with these same variables, remained about the same.
For overall patients (i.e., including those with many comorbidities) over 80, the complication rate for total knee replacement went from 9.9 percent to 9.1 percent, and for total hip replacement, it went from 9 percent to 10.3 percent.
Again, these figures include the patients with more comorbidities (e.g., diabetes, congestive heart failure, poor kidney function).
The in-hospital death rate for patients over 80 who had a total knee replacement was 0.3 percent, and for total hip replacement, 0.5 percent.

Dr. Bergin is a general orthopedist, surgically and conservatively treating all manner of bone and joint conditions. She enjoys educating patients so they can emerge stronger than they were before their orthopedic injury or surgery.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Boryana Manzurova
Source: sciencedaily.com/releases/2014/07/140717125051.htm

IBS Cramps vs. Menstrual Cramps (PMS)

A female GI doctor who specializes in women’s GI issues addresses IBS vs. menstrual cramps related to PMS.
What are the differences between IBS cramps and those from premenstrual syndrome?
“The main difference between menstrual cramps and IBS cramps would be the timing,” begins Diana Y. Wu, MD, a gastroenterologist and assistant professor of medicine at Brown Medical School.
“Menstrual cramps usually occur a few days before onset of menstruation, whereas IBS cramps can occur at any time, especially in the mornings, after eating, or in times of stress/anxiety.
“IBS cramps can often be relieved by having a bowel movement. Menstrual cramps tend to be lower in the pelvis and not necessarily relieved with defecation. It tends to resolve after the menstrual cycle is completed.”
The cause of the cramps in irritable bowel syndrome and in PMS differs.
In PMS the cause is hormones called prostaglandins, which is why the anti-prostaglandin drug, ibuprofen, is so effective at relief.
The prostaglandins cause uterine contractions, and that’s the “cramping” that a woman feels.
“Irritable bowel syndrome is characterized by chronic abdominal pain, and associated with changes in stool frequency or consistency (e.g., diarrhea or constipation) in the absence of any physical cause that is detectable by our current medical investigations,” explains Dr. Wu.
“The pain is usually relieved or ameliorated with a bowel movement.”
Perplexing
“The pathophysiology of IBS remains unclear and is believed to be multifactorial,” continues Dr. Wu.
“Despite multiple investigations, data have been conflicting and no abnormality has been found to be specific for this disorder.”
I’ve never had IBS so I can’t describe what the cramping feels like. But I’ve had cramping from premenstrual syndrome and microscopic colitis, and they feel identical.
Ironically (though not surprisingly), prostaglandins are implicated in flare-ups of microscopic colitis, though research in this area is scant.
I know that the cramping I had, during the microscopic colitis flare, was related to this benign inflammatory bowel disease because when it happened, I had already completed menopause. Very fascinating!
But prostaglandins don’t seem to be involved in the cramping of IBS.
Causes of IBS are not clear.
“The traditionally favored hypotheses are: alterations in gastrointestinal motility (no predominant pattern of motor activity has emerged as a marker for IBS), visceral hypersensitivity, alteration in fecal flora (such as after gastrointestinal infection/food poisoning), bacterial overgrowth, food sensitivity or a genetic predisposition,” explains Dr. Wu.

Shutterstock/KDdesignphoto
Bacterial overgrowth and food sensitivities are theorized to be causative factors behind microscopic colitis, which is often misdiagnosed as IBS…and vice versa.
Dr. Wu further explains, “Visceral hypersensitivity (increased sensation in response to stimuli) is a frequent finding in irritable bowel syndrome patients.
“Several studies have focused on increased sensitivity of visceral nerves in the gut, triggered by bowel distention or bloating, as a possible explanation for IBS symptoms.
“About half of patients with IBS experience bloating in addition to abdominal pain.
“They may have a measurable increase in abdominal girth associated with bloating (sensation of abdominal fullness), and this may be due to impaired transit of intestinal gas loads.”
Is there a way a woman can tell if the cramps she feels are IBS related or from PMS or mid-cycle cramping?
“There is no way to know for sure. However, typically IBS cramping is relieved with defecation.”
 Dr. Wu is a graduate of Harvard Medical School and is board certified in gastroenterology and internal medicine. She is well-versed in multiple endoscopic procedures and all GI disorders.
Dr. Wu is a graduate of Harvard Medical School and is board certified in gastroenterology and internal medicine. She is well-versed in multiple endoscopic procedures and all GI disorders.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

How to Lessen Anxiety over Moles and Melanoma

Are you so afraid of your moles that you no longer can look at them, for fear of what you might see?
Serial Digital Dermoscopy
This wonder of technology will give you great peace of mind. I’ve had this procedure electively done and will continue having it done.
Moles are photographed, then examined on the computer screen under high magnification by the dermatologist.

Not only that, but (depending on the specific system) the computer database compares the image to data from melanoma and then comes up with a rating. The rating can be a number or color.
The computer does NOT diagnose melanoma, but it indicates that a mole is suspicious or has characteristics that resemble melanoma more than it resembles a benign lesion.
Based on the rating, the doctor will then decide on further action (or not).
Now imagine the reduction in your anxiety when the doctor tells you, “All of your moles look very stable. You don’t have to come back for another 18 months.”
Serial digital dermoscopy is done yearly, every 18 months or even every two years (depending on the doctor’s recommendations, though you can have it done as often as you’d like).
The same moles are photographed, and the computer program compares new photos to previous images and will detect changes — earlier than a dermatologist possibly can, even with their handheld dermatoscope.
SDD may run about $250, depending on where it’s done.
Home Mole Mapping
Map out your lesions at home (if you don’t have too many), using a large sketch book.
Even if your drawings of various body parts are crude, at least this way you’ll have an idea of where you have moles, so that you will know if new ones have appeared.
This will reduce a lot of anxiety.
Illustrate
If you can illustrate, then draw and render your moles; this will significantly reduce anxiety.
I’ve done this (I can illustrate shape and texture, plus draw scaled-up images; I knew someday this skill would come in handy).
Many artists may not think to do this.
Whip out your favorite illustrating tool and draw your moles, capturing variations in color, patterns, texture, border, etc.
Then, when it’s time to do monthly self-exams, you’ll have a better chance of detecting a change.
Monthly Self-Exam
“An at-home approach to monitoring moles may include the ever popular selfie!” says Emily de Golian, MD, a board certified dermatologist with Forefront Dermatology in Atlanta, GA.

Shutterstock/pixinoo
“Take a photo of any moles in question from a distance for orientation, so you can tell which body part is being photographed, and close-up to capture what the mole looks like in detail,” continues Dr. de Golian.
“You can compare your skin to these selfies periodically, such as during a monthly skin self-exam, and if any changes have occurred, call your dermatologist for an appointment.”
Commit to a self-skin exam every month without fail. This way you won’t wonder, “When did this mole begin changing?” or, “Did this mole look this way only a few weeks ago?” The monthly selfie will cut a lot of anxiety.
Annual Clinical Exam
Have a dermatologist examine your skin from head to toe, and make sure they use a dermatoscope. This will lower anxiety.
“Annual skin exams and any required follow-up are typically covered by insurance,” says Dr. de Golian.
“Patients should call for a sooner follow-up if they notice any new or changing spots.”

shutterstock/wavebreakmedia
Know that only 30 percent of melanomas arise in pre-existing moles (Yale School of Medicine).
Next, to reduce mole anxiety and if you’re tech savvy, you can get an application for your smartphone that works in a similar way to digital serial dermascopy.
There are many apps like this, but they do NOT replace the type of digital serial dermoscopy that was described previously.
Consider it an adjunct to your skin health surveillance program.
Finally, to rid yourself of mole anxiety, have the spot removed and biopsied.
Don’t put this off. Just get it done. Depending on your insurance plan, you won’t have to pay for this other than the copay.
If you want to get rid of mole anxiety as much a possible, the money invested to do this will be well worth it.
 Dr. de Golian focuses on the surgical treatment of skin cancer via Mohs surgery, cutaneous oncology (melanoma and basal cell carcinoma), surgical defect reconstruction and cosmetic dermatology.
Dr. de Golian focuses on the surgical treatment of skin cancer via Mohs surgery, cutaneous oncology (melanoma and basal cell carcinoma), surgical defect reconstruction and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio
Source: medicine.yale.edu/dermatology/

Elderly Parent Refuses to Go to ER: How to Make Them

Here is how to make a stubborn elderly parent go to the emergency room.
Have you ever heard of a case in which an elderly person died because their medical treatment was delayed, because family members couldn’t get that individual to visit the emergency room?
I’ve always wondered how it’s not possible for the adult child of an elderly person, who’s compromised by an illness or injury, to make them get into a car and be driven to an emergency room.
I made my elderly mother, who refused to go to the ER, get in the car and be driven to the ER.
She was delirious and wouldn’t keep still, requiring nonstop supervision.
The delirium ultimately had been diagnosed as a side effect from a type of medication that, in a very small percentage of recipients, causes a reactive “psychosis.”
The drug had been prescribed by a neurosurgeon to mitigate fluid buildup in her brain as a result of a recurrence of a chronic subdural hematoma.
So to this day, we’ll never know how much of that “psychosis” was brought on by the increasing blood and fluid in her brain (sounds frightening but she fully recovered).
My elderly mother flat-out refused to go to the emergency room, even though I and my father were insisting on this.
My father had orthopedic issues and was not in a position to use a hands-on approach to make my mother get into the car.
Look, if you have an elderly parent who needs to go to the ER, and he or she refuses, there is NOTHING stopping you from doing what you intuitively know is the right thing to do!
I forced my mother into the car. This sounds like I used violence, but all I did was stand behind her, place my hands on her upper arms, and “force” her to walk out of the kitchen, through the laundry room and into the garage. There was no way she could break loose.
Holding her upper arm with one hand, I opened the car door with the other hand, and I made her get into the front seat.
I turned her body to face the open door and gently pushed downward, making her lower.
I guided her into the seat, lifting her legs into the car, then quickly closing the door. I then put her seatbelt on.
My father and I knew she’d try to get out. I quickly got in behind her as my father put on the automatic lock for all the doors.
This way my mother couldn’t open her door. She was still verbally delirious and insisting she be let out.
The drive to the hospital took 40 minutes, during which I kept my hands firmly on my mother’s shoulders while I sat behind her.
Several times she reached for the door handle, and I didn’t quite trust that automatic lock.
I kept her pinned against the seat with my hands. She kept saying she wanted to jump out.
The CAT scan at the emergency room revealed the chronic subdural hematoma, and since the scan looked pretty much the same when compared to the one that had been taken a few days ago, the ER doctor deemed my mother’s behavior to be an adverse reaction to the drug.
She was admitted and underwent a second burr-hole operation to evacuate the cSDH, then fully recovered within a few weeks.
You do NOT have to injure or bruise an elderly parent in order to “force” them to walk to a car, get in, and be driven to the ER.
If your elderly parent can’t walk (my mother had no problem walking), then pick them up.
If your parent is heavy, then of course, picking them up won’t always be an option.
If it’s impossible to get them into a chair with wheels or a wheelchair and roll them to the car, then hoist them in, or if two people find they can’t dually carry the person, then call 9-1-1.
If an elderly person falls and can’t move much, leave them be and let professionals do the moving!
When my elderly father blacked out, fell, hit his head and had an altered mental status at 3:00 in the morning, I found him on all fours (elbows on floor).
This was a week after he had total knee revision surgery.
Though he was conscious, all 190 pounds of him, combined with the inability to realize he needed to try to get into a seated position on the floor, made his body dead weight.
I took the mobile phone into another room and dialed 9-1-1.
He didn’t want me to call 9-1-1, and my mother was even swayed by his insistence that he was alright (by then she had talked him into making his way, along the floor, to a seated position on the floor with his back against the bed).
But I wouldn’t have it. Within minutes, four EMTs arrived and properly transferred my father, neck brace and all, into a special chair and secured him in it, then carried the chair down a flight of stairs and out the front door. He fully recovered.
So as you can see, there’s really NO reason why you can’t somehow, some way, get an elderly parent to the emergency room, no matter how much they refuse to go.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Racing Heart after Climbing Stairs: Cause & Solution

If your heart races after you climb a flight of stairs, here’s one reason why and how to solve this problem.
When I worked as a personal trainer at a large gym, I’d have my clients simply walk up a flight of stairs to see if they’d get a racing heart.
I just want to first encourage those who experience a racing heart after going up a flight of stairs to have a complete exam by a cardiologist.
A healthy person (no heart troubles) who is de-conditioned due to lack of exercise will experience a racing heart after climbing stairs fast enough.
Even a slow pace can get the heart rate shooting up in an otherwise healthy person.
When I was in a volleyball club years ago, consisting of primarily 20-somethings, these young people hated having to climb five flights of stairs to get to the fifth story of the building where the courts were set up — and these were experienced volleyball players.
Going up flights of stairs is no picnic, even to athletes.
Climbing stairs, to any out-of-shape individual, is a bear, and it’s expected that their heart would be racing at the top.
If climbing stairs produces other symptoms besides a racing heart, this would be cause for concern, such as chest pain, nausea and feeling faint.
A heart that’s not conditioned will race under exertional circumstances, even in the absence of an abnormality, heart disease or other medical condition.
The Fix Is to Exercise
You may already think you’re getting plenty of exercise, including “going up and down the staircase at home a hundred times a day.”
But use of a staircase in the activities of daily living is not sufficient to overcome the racing heart issue.

Casual use is not enough. Shutterstock/Javani LLC
Program for Preventing a Racing Heart from Climbing Stairs in a Healthy Individual
Incorporate twice weekly sessions of high intensity interval training. HIIT will teach your heart to get used to brief high loads of exertion and to recover quickly from them.
HIIT is superior to inducing this kind of cardiac fitness when compared to steady state aerobic sessions.
For best results, conduct HIIT using a staircase.
One of the versions of this that’s very effective is to dash up a flight of stairs while holding dumbbells or weight plates.
The “dash” can be a walk, if that’s all you can do with the weights.

The objective is to move as fast as you can (even if it’s a slow pace) while holding the weights.
At the top of the stairs following one of these dashes, your heart should be racing. That’s the objective.
If it’s not racing, go faster or use heavier weights. (Of course, if you get chest pain, nausea or otherwise feel sick, stop the activity.)
So if holding 10 pound dumbbells no longer is difficult even with a fast trot, then see what happens when you use 12- or 15-pounders. Use more weight over time.

At the top, set down the weights and walk around for one to two minutes, then do another set (four or five total). Do not sit or stand still during the rests. Keep moving during the recovery.
For healthy beginners, you should have a rating of perceived exertion of 6-7 at the top of the staircase.
For fitter people, aim for an RPE of 8-9. This is based on a scale of 1 to 10, where 1 = how you’d feel soaking in a hot tub, and 10 = how you’d feel after trying to outrun a train.
The ideal staircase is at least 30 steps (two or more flights), but don’t climb so many steps that after 30 seconds, you’re still climbing.
This is supposed to be short, brief bursts of exertion, not a pacing type of movement.
To prevent your heart from racing from casual use of a staircase (like on the job or around the house), you must get your heart racing via HIIT, and twice a week is all you need.
On one or two additional days, yes, I encourage steady state cardio. But if you rely only on steady state (long duration aerobics), it won’t produce the spectacular results of HIIT.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/Orawan Pattarawimonchai

Is Daily Aspirin Beneficial if You Have a Zero Calcium Score?

Here’s information if you’ve ever wondered if it would be worth it to take a daily aspirin even though you’re calcium score is zero.
Are you wondering if there would be any benefit to taking a daily aspirin because your coronary calcium score is zero?
Would popping a small aspirin every day make your risk of heart attack even lower?
I wondered about that, as I my calcium score is zero; I figured that adding a daily aspirin would really, really make me resistant to a heart attack.
Now, a study has come out answering this question. Michael D. Miedema, MD, the study’s lead author, says in the paper, “Many heart attacks and strokes occur in individuals who do not appear to be at high risk.”
Dr. Miedema points out that treating only those people with a high risk of heart attack with a daily aspirin means that a “substantial portion of patients” without high risk will go on to have a heart attack that maybe could have been prevented with daily aspirin therapy.
Aspirin, because it’s a blood thinner, can cause internal bleeding. This is the problem with taking this drug when you aren’t at high risk for a heart attack; you risk internal bleeding to prevent a heart attack that would have never occurred in the first place.
The American Heart Association recommends aspirin for those who have known cardiovascular disease or who are at high risk for a heart attack. This drug is not advised for those at low or even intermediate risk.
Dr. Miedema’s study looked at over 4,200 participants who were followed for about seven years.
They were grouped according to their calcium scores. Heart attack rates in each group were calculated.
Results
Subjects with calcium scores over 100 were two to four times more likely to benefit from daily aspirin than to be harmed, even if they didn’t qualify for daily use according to the current AHA guidelines.
Subjects with a calcium score of zero were two to four times more likely to suffer harm from aspirin than any benefits.
These results stood ground even when traditional risk factors were accounted for.
The results mean that significant plaque buildup means this individual is “much more likely to prevent a heart attack with aspirin use,” says Dr. Miedema in the report, “than to suffer a significant bleed.”
But conversely, if you have a zero calcium score, the daily aspirin would result in more harm than anything good — even if you have any risk factors for heart disease (e.g., high cholesterol).
Dr. Miedema says that a zero calcium score “is associated with a very low risk of having a heart attack.” He adds that such individuals may not benefit from preventive drugs.
Well, that does it for me. I have not yet taken the daily aspirin, and I have decided not to.
Why risk internal bleeding, which I’d more likely suffer than a heart attack, what with my zero calcium score?
Nevertheless, if you’re not sure what to do, consult with a board certified cardiologist.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Photographee.eu
Source: sciencedaily.com/releases/2014/05/140509172919.htm

Dent in Middle of Thigh Muscles Is Benign, Harmless

There’s no cause for alarm about that dent in the middle of the front of your thigh; there’s a benign explanation.
As a result of consulting with Dr. Google, many people are in a state of panic upon discovering a “dent” in the middle of their upper thigh.
Check out the woman below; does she have the same kind of dent in the middle of her upper thighs as in yours?
This athlete’s thigh has an elongated dent.

The lower central dent is caused by the tendon that’s between the two pennate structures of the rectus femoris muscle.
The rectus femoris is a pennate type of muscle. This means that the muscle fibers attach diagonally to the central tendon that divides the two sections of this muscle.
So more specifically, the rectus femoris is a bipennate structure (“bi” meaning two). You can clearly see this in the anatomical illustration below.

The more muscle fiber in any given cross-section, the more force that can be generated.
Quadriceps muscles are pennates in order to be very potent force producers (think sprinting, squatting, jumping, leg pressing, kicking down doors).
The reason that the muscle fibers attach diagonally to that central tendon is to get as much of the muscle fiber as possible in any given cross-section.
The central tendon will be more visible in a person who has lower bodyfat, in combination with toned muscles.
If you see a dent that wasn’t in your middle front thigh before, you’ve either lost some bodyfat and/or increased the tone of your muscles.
Dents in the thighs actually go by several names in the bodybuilding/physique-sculpting community: cut, crack and definition. The goal of such athletes is to get as deep a cut as possible.
There’s a reason why you’ve never seen flabby, mushy thighs with dents in them.
Soft, untoned muscles aren’t firm enough to create this impression, especially if there’s a higher level of bodyfat.
Thus, a “skinny fat” person can be minus a visible dent in their thigh.
People who’d be considered “fat” won’t have a visible dent in their thigh, middle or anywhere.
Do not freak out or feel fear upon looking at your thigh dent.
Instead, reassure yourself with anatomy illustrations and images of physique athletes.
Google “sculpted thighs,” and similar keywords, such as “bodybuilders’ legs,” and “lean muscular quads,” etc. You’ll see plenty of dents.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}