

Glucerna Ingredients Include Soy & Artificial Sweeteners

Is Glucerna really healthy for people with diabetes, since these products are so highly processed?
The Glucerna trademarked slogan is “Smart nutrition for people with diabetes.” Perhaps you’ve seen TV commercials for Glucerna, and if diabetic, have concluded that these products are super healthy for the human body.
Below are the ingredients for Glucerna’s “snack shake,” chocolate — and these ingredients are similar to those of Glucerna’s chocolate bars.
Water, corn maltodextrin, fructose, milk protein concentrate, glycerine, high oleic safflower oil, cocoa powder (processed with alkali), less than 1% of: sodium caseinate, canola oil, soy protein isolate, fructooligosaccharides, soy fiber, cellulose gel, natural and artificial flavors, sodium chloride, magnesium phosphate, potassium citrate, calcium phosphate, soy lecithin, cellulose gum, choline chloride, ascorbic acid, carrageenan, acesulfame potassium, potassium chloride, gellan gum, sucralose, and the remaining ingredients are vitamins and minerals, though ascorbic acid is vitamin C.
A health conscious person, whether diabetic or not, will notice several ingredients in Glucerna’s products.
These would be the soy, canola oil, artificial flavors, sucralose (an artificial sweetener), acesulfame potassium (another artificial sweetener) and fructooligosaccharides (yet another artificial sweetener).
Canola oil contains hexane and trans fats. Though this oil has some redeeming features, it makes sense that a health conscious person would want to avoid ingesting hexane and trans fats.
And soy — the unfermented kind — has been linked to some health issues, and its effect on the body is debatable as far as beneficial vs. potentially harmful. Plus, some people are allergic to it.
Processed soy in a bottle is not the same as tempeh or miso soup.
Need I say anything about artificial sweeteners? Well, one thing’s for sure: Scientists are divided on the safety and risks of artificial sweeteners, even though animal studies are quite compelling.
A diabetic may figure that controlled blood sugar trumps any possible harm linked to canola oil, soy or artificial sweeteners.
Final Verdict About Glucerna for Diabetes
The carbohydrates in Glucerna’s products are designed to be more slowly absorbed into the bloodstream, something that would appeal to diabetics for blood sugar management.
As far as strictly blood sugar absorption, a serving of Glucerna chocolate products are much better for a diabetic’s glucose metabolism than would be, say, a chunky piece of Betty Crocker devil’s food cake.
Both items are highly processed, but Glucerna is more preferable when you look at the overall picture.
So when you compare it to Duncan Hines, Betty Crocker or Walmart’s chocolate baked goods, Glucerna is the best option, relatively speaking.
The Glucerna “snack shake” is gluten- and lactose-free, and an 8 ounce can offers: 140 calories, 5 grams fat, 230 mg sodium, 19 grams carbohydrates, 3 grams fiber and 7 grams protein.
 Katie Tomaschko, MS, RDN, has a master’s degree in nutrition & dietetics and has studied nutrition for 12+ years. She owns a private practice where she conducts 1:1 private nutrition counseling. She is also the owner and contributing writer for sportingsmiles.com.
Katie Tomaschko, MS, RDN, has a master’s degree in nutrition & dietetics and has studied nutrition for 12+ years. She owns a private practice where she conducts 1:1 private nutrition counseling. She is also the owner and contributing writer for sportingsmiles.com.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sources hsph.harvard.edu/nutritionsource/2015/04/13/ask-the-expert-concerns-about-canola-oil/
thewholesoystory.com/index.php?pageID=Media

Childless Adults Qualified to Give Parenting Advice

After you read this, you’ll be convinced that sometimes, childless people are heavily qualified to dole out parenting advice!
But first, are you one who believes that people who’ve never had children are out of line for giving parenting advice?
According to this line of reasoning, any person who’s raised kids is qualified to give parenting advice. But come on, we know this is so far from the truth. Would YOU take parenting advice from Britney Spears, Kate Gosselin, Mama June or Bobby Brown?
Think of one of the most selfish, narcissistic, impatient and uncaring adults you know. Does that person have kids? What kind of parenting advice do you think they’re capable of giving?
Good parenting advice will come from loving, clever, creative, patient, affectionate and rational people.
And bad parenting advice will come from bitter, emotionally distant, self-centered individuals, especially those with anger management problems.
It doesn’t make any difference if this latter group has raised 10 children. This quantity simply means they’ve imposed their crippling traits on 10 kids, not zero.
“A person does not have to have walked in another person’s shoes in order to give them advice,” says Stacy Kaiser, a southern California-based licensed psychotherapist and relationship expert with a special interest in the topic of bullying.
“You do not have to have been an alcoholic to have suggestions for someone who drinks too much,” continues Kaiser with this analogy. “Similarly, you do not need to have a child to offer up parenting suggestions.”
Or as the saying goes, One need not be wearing your shoes to see that your shoelaces are untied.
It’s important to note that Kaiser says that “having lived the experience of being a parent, one does pick up tools and ideas that they may not have had,” in the absence of parenthood.
You may know of someone who has five kids and want parenting advice from them simply based on this.
- What if you learned that this adult was prone to temper outbursts and had little patience?
- What if you learned this individual never read to her children when they were very young?
- Never tucked them in bed?
- And when her daughter goofed up during a piano recital, the mom shamed her afterwards?
- Would you still want this woman’s parenting advice?
My brother sought parenting advice, prior to having children, from a psychiatrist who had no children.
My brother’s three kids are among the most self-confident, emotionally stable human beings I’ve ever met. They are what you’d say are “going somewhere big in life.”
Still think people without kids have no business telling others how to raise theirs?
Whom would you want as your young child’s nanny?
A 45-year-old narcissistic, impatient, arrogant, high-strung woman who’s quick to criticize over every little thing—but has raised four children?
Or a same-age woman who’s never had kids—but, is very tender, calm, patient, warm and cozy to be around, is quick to praise and is fun-loving and kind-hearted? The answer is a no-brainer.
Sometimes, a childless person is in a prime position to give parenting advice simply because they are skilled at creative problem solving. Sometimes they simply have common sense.
Sometimes it’s because their parents made enormous mistakes. An example might be a man named “Rob” giving advice to a buddy, “Steve,” who has a 13-year-old son on how to handle the son’s complaints that he’s getting bullied at school.
Maybe Rob was brow-beat by his father for being a “wimp” at school, and this made him even more vulnerable to the bullies, feeling more powerless.
This poor guy, as an adult, may very well have stellar advice for Steve that could lead to empowering the 13-year-old.
Isn’t it funny that the criticism of, “What do YOU know? You don’t have kids!” never applies to when the childless person gives advice that the parent actually agrees with? Now that’s something to really reflect upon!
An adult is either a bad person or a good person. Having kids usually will not alter that status.
With so many parents out there “screwing up” their children, how can anyone denounce the concept of childless people giving parenting advice?

With over 100 TV appearances on major networks including CNN, NBC, CBS and ABC, Stacy Kaiser brings a unique mix of provocative insight to many topics such as anger management, office relationship issues and parenting.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Why Parents SHOULD Try to Be Popular with Their Kids!

There are reasons why you SHOULD try to be popular with your kids, including teens!
How many times have we all heard, “Parenting is not a popularity contest”? What this refers to is the observation that parents try to get their kids to “like” them, or are upset that their children or teens seemingly don’t “like” them.
They are reminded by other parents that being a parent isn’t a popularity contest.
But actually, it should be. Now think about that for a moment: If you’re popular with your kids…you’ll be the first, or at least one of the first, people they will come to for advice and counsel.
If you’re NOT popular with your children and teens, then gee…why on earth would they ever trust YOU with the big problems in their life (and by “big,” I mean not only what seems monumental to them, and what truly is monumental)?
So yes, parenthood should be a popularity contest.
The issue, then, is how to be popular with your kids. This is where some parents get off track.
But just because they get off track doesn’t mean it’s a mistake to try to be popular with your children or teenagers.
It’s simple: They won’t come to you for guidance if they don’t like you. They won’t listen to you if they don’t like you. They will tune you out if you’re not popular with them.
And I don’t mean technical guidance, such as how to cook something, how to do something on the computer, how to work with your phone’s new app, or help with some story problems in math.
I’m talking about life advice. Parents who are popular with their kids will be the first picks when it comes to life advice.
- If your children like you, they will take your lead and admire you.
- They will trust you.
- They will talk to you.
- They will listen. And isn’t all of that what you want?
Would YOU ever seek counsel from another adult—if you didn’t like that person?
Of course not! Imagine how uncomfortable you’d feel if you tried to pour out your troubles and worries to someone whom you did not like. Think about that.
And even if they offered good advice, you’d be hearing it through a skewered lens, and thus would miss its merit.
Now imagine how difficult it would be for someone whose brain isn’t even finished developing to share their concerns and anxieties with someone they didn’t like.
As a parent, your goal should be to get your kids to like you—and this is accomplished by making them feel they can come to you about anything without facing ridicule, criticism, judgment or anger.
You cannot buy your child’s trust and admiration.
So why do some parents scowl at the idea of being “popular” with their kids?
Other than the fact that some parents believe that in order to be “popular” with their children, they must spend a lot of money on the coolest gadgets and clothes for them (wrong, wrong, wrong!), the issue may very well be semantics.
“I prefer to say that parents want to be well-connected and close with their children than using the word popular,” says Stacy Kaiser, a southern California-based licensed psychotherapist and relationship expert with a special interest in the topic of bullying.
Kaiser continues, “Parents who are well-connected with their kids typically end up having children who are open with them, who will share things with them, and who will go to them for advice.
“As a parent, it is very important to always maintain the parental role. While we can be close with them and have a friendship with them, we must always remember that there is a hierarchy and that we are a parent.”
With over 100 TV appearances on major networks including CNN, NBC, CBS and ABC, Stacy Kaiser brings a unique mix of provocative insight to many topics such as anger management, office relationship issues and parenting.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Convincing a Doctor Dense Breasts Are a Serious Cancer Risk

Not all doctors are on board with the studies that clearly show dense breasts are a significant risk factor for breast cancer.
If your doctor isn’t convinced, here’s material you can present to your doctor.
The issue of high breast density as a significant increase in the risk of breast cancer, and as something that makes it more difficult to be identified on a mammogram, is right about where the issue of smoking was about, say, 60 years ago.
At some point, maybe in the 1950s or 1960s, a lot of doctors began raising concerns about the dangers of smoking.
This hardly caught on like wildfire. It took many years for the entire medical establishment to catch on and have a universal consensus about the hazards of smoking.
We’re seeing this very slow spread of the truth with the breast density thing. Some gynecologists and gynecological nurses take this issue quite lightly and even recommend AGAINST the additional screening tools such as the ultrasound, for women with extremely dense breasts. They are WAY BEHIND the research.
They act as though, ho hum, it’s no big deal that a woman has extremely dense breast tissue.
Never mind that extreme breast density comes in third place for non-modifiable risk factors (after family history and BRCA mutations, in middle-aged women for whom advanced age is not yet a significant risk factor).
If you have such a physician or gynecological nurse who is in denial over the mounting evidence, below is information you can present to that individual. It will be very difficult for him or her to deny it:
We hope this study raises awareness that dense breast tissue is a risk factor for breast cancer and that alternative technologies, including automated whole-breast ultrasound and contrast-enhanced mammography, are available to aid in screening women with dense breasts.
Haatal B. Dave, MD, M.S., resident physician at Yale University School of Medicine in New Haven, Conn
sciencedaily.com/releases/2012/11/121127003317.htm
As far as screening programmes are concerned, it is already known that breast density is a risk factor for the occurrence of breast cancer and that it decreases the sensitivity of mammograms.
Our study confirms the importance of taking breast density into account in the screening setting.
Dr. Louise Eriksson, MD, Stockholm South General Hospital
ncbi.nlm.nih.gov/pmc/articles/PMC4010151/#:~:text=Although%20it%20remains%20the%20gold,dose%2C%20cost%20and%20patient%20anxiety.
Although mammography remains the gold standard for breast cancer screening, there is increasing awareness that there are subpopulations of women for whom mammography is limited because of its reduced sensitivity based on an individual’s breast density and other factors.
Jennifer S. Drukteinis, MD, assistant member in Moffitt’s Department of Diagnostic Imaging
news-medical.net/news/20130405/Researchers-say-breast-cancer-screening-requires-a-personalized-approach.aspx
Increasing age and high breast density are among the strongest risk factors for the disease.
Karla Kerlikowske, MD, a professor of medicine at UCSF and a physician at the UCSF-affiliated San Francisco VA Medical Center
ucsf.edu/news/2013/03/13682/biennial-mammograms-best-after-50-even-women-dense-breasts
The sensitivity of mammography is inversely proportional to breast density.
Blaise P. Mooney, MD, an assistant member in Moffitt’s Department of Diagnostic Imaging
moffitt.org/newsroom/press-release-archive/2013/moffitt-cancer-center-researchers-discuss-new-frontiers-in-breast-cancer-screening/
Clinical literature says that mammography eventually finds 85% of breast cancers, but for women with dense tissue, it’s often too late by the time the cancer is detected. MRI is near 100% sensitive for finding cancer in dense breast tissue. It’s the exam we’ve been waiting for, and it’s been available all along.
Dr. David Strahle, president of Regional Medical Imaging in Flint, MI
auntminnie.com/index.aspx?sec=ser&sub=def&pag=dis&ItemID=105131
“Women with radiologically dense breasts (heterogeneously dense or extremely dense in the terminology of the Breast Imaging Reporting and Data System [BI-RADS]) have a threefold to six fold increased risk of breast cancer compared with women who have fatty breasts.”
webmd.com/breast-cancer/tc/overview-risks-breast-cancer?page=3
Women with dense breasts are four to five times more likely to get BC, say these sources:
– Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 356(3):227-36, 2007.
– Yaghjyan L, Colditz GA, Collins LC, et al. Mammographic breast density and subsequent risk of breast cancer in postmenopausal women according to tumor characteristics. J Natl Cancer Inst. 103(15):1179-89, 2011.
“Tumors also are dense tissue and appear as solid white areas on the mammogram. This can make it more difficult to detect a tumor in dense breasts because it looks a lot like the dense tissue that surrounds it.”
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
ocregister.com/articles/breast-540118-dense-cancer.html
Top image: Freepik

Low Back Pain in the Morning: Causes & Solutions
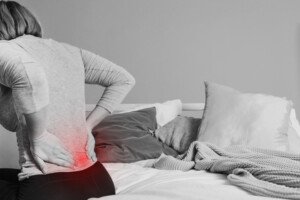
If you’re fed up with morning back pain, a chiropractor explains the causes and how to treat this problem.
“When low back pain predominantly begins in the morning, the source is often from arthritic facet joints and degenerative changes,” begins Dr. Jeff Langmaid, DC, Founder/owner of The Evidence Based Chiropractor, LLC, in Florida, a research-based marketing and practice growth company that serves thousands of chiropractors across the world.
“Often, patients will tell their health care provider that it takes them a while to ‘get their engine going,’ or sometimes it takes a few minutes before they are able to stand up without fear of a painful episode.
“Others will say that they have to take a hot shower before ‘things loosen up’ enough to get moving throughout the day.”
Cause of Morning Back Pain Explained in Detail
Dr. Langmaid says, “When we go to sleep at night, the capsules around the facet joints of our spine essentially shrink because we don’t move as much at nighttime as we do during the day.
“When we wake up in the morning, it can take a little bit of time to get the blood pumping to the surrounding muscles and tissues to lubricate those facet joints.
“This is the same for any degenerative spine condition that creates stiffness or pain that predominantly takes place in the morning.
“As we go through our normal ranges of motion, it pumps blood to the area and creates a more dynamic environment as we get our day started.”
Solutions
“Common solutions are to take a hot shower, which will increase the blood flow to the area and can loosen up that tissue as you start your day,” says Dr. Langmaid.
“Some of the other things that can be extremely helpful are going through a stretching routine that is approved by your health care practitioner.
“One thing that I think has been of great value to some of the patients I have had in the past is to perform a stretching routine before you go to sleep at night.
“Many people report waking up with less pain, stiffness and dysfunction when they’re able to do some stretching before they go to sleep at night and when they wake up in the morning.”
 Jeff Langmaid, DC
Jeff Langmaid, DC
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

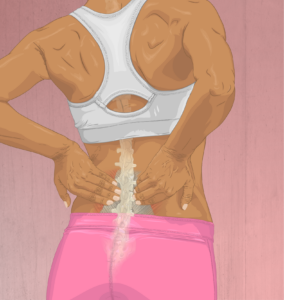
Back Cracks During Sit-Ups: Causes & Solutions

Find out from a chiropractor, not a layperson or “fitness expert,” why your back cracks during sit-ups and what to do about this annoying and to some people, unnerving response to the exercise.
A personal trainer is perhaps not the best person to explain why your back makes cracking sounds when you do sit-ups.
“Back cracking during sit-ups, or during any activity, is commonly caused by the facet joints gapping or spreading,” explains Dr. Jeff Langmaid, DC, founder/owner of The Evidence Based Chiropractor, LLC, in Tampa, FLA, a research-based marketing and practice growth company that serves thousands of chiropractors across the globe.
Dr. Langmaid continues, “The facet joints are load-bearing joints on the posterior, or the backside, of the spine.
“As they go through their range of motion, they can release gas, causing a ‘pop,’ ‘click’ or ‘cracking’ sound — similar to a knuckle.
“Most often that sound does not indicate pain, but on occasion, it certainly can.”
The cracking sound is due to the release of gas bubbles from the synovial fluid which helps lubricate the joints.
So when your back cracks while you do sit-ups, this is normal as long as there is no pain, and it’s nothing to worry about. However, for some people it can be annoying.
Source: myupchar. com
Dr. Langmaid explains, “In terms of solutions to eliminate back cracking, one option would be to not extend into that full range of motion, as cracking often occurs when the joint is stretched.”
The stretching can make one of those gas bubbles pop.
“Occasionally, cracking can be accompanied by pain,” says Dr. Langmaid.
“Not going through the full range of motion and staying in a safe and controlled range of motion can prevent the joint from fully gapping and reduce the snapping, popping, clicking or cracking sound.
“Additionally, when performing sit-ups, it is imperative to use proper technique.
“This will allow you to maximize the workout and gain optimal muscle strength without placing too much stress on your spine.”
Proper Technique for Sit-Ups
To perform a sit-up correctly, start by lying on your back with your knees bent and feet or heels flat on the floor.
Place your hands behind your head, at its side or across your chest, making sure not to pull on your neck or head.
Engage your core muscles and slowly lift your upper body towards your knees without rounding your back, ideally keeping your lower back pressed to the floor.
Exhale as you come up and pause briefly at the top before lowering your back down with control.
Finally, you should avoid using momentum or jerking movements.
Proper technique with the sit-up is not a guarantee that your back won’t crack, but at least now you know that it’s just a normal occurrence when bubbles form in the synovial fluid and they get popped.
Jeff Langmaid, DC
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/wavebreakmedia
What REALLY Happens when a Mole “Appears” Overnight
So you’ve discovered a “new” mole that has appeared overnight; however, things aren’t always as they seem.
“There really isn’t such a thing,” says Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
“People often talk about something appearing overnight, but it’s not possible,” he continues.
“There are some tumors that grow rapidly, such as keratoacanthoma, but even these take several weeks on average.
“Most growths appear over time, but the person may not notice these, and then all of a sudden notices the lesion and thinks it appeared overnight.”
Don’t Get Caught off Guard
Here’s what you should do to ensure that you aren’t caught off guard by a mole that seemingly develops overnight: Create a mole map of your body.
This won’t be practical if you have a high number of moles, but even then, you may want to construct a map of perhaps one portion of your body that isn’t heavily peppered with moles.
Or, you can map out specifically those moles that are bigger.
Look at various parts of your body and, with a large sketch pad and a pencil, indicate the location of the moles (it helps to be able to draw, but even if you’re not skilled in this area, do your best; it will certainly help you get to know your moles).
If you find this task too daunting, you may want to consider serial digital dermoscopy, a technology for tracking suspicious changes in moles over time.
There are various apps available as well that can help track changes in moles.
These apps are not meant to diagnose. They are only meant to provide a visual guide to any changes in a pigmented lesion over a course of time.
You should also be consistent with monthly or at least, every two months, self-exams of your skin, including awareness of areas that don’t have any moles.
Keep in mind that a very tiny scab can pass as a mole that appears overnight.

Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Dark Spot on Lip Can Be Melanoma

A new appearing dark spot on your lip can be melanoma, the most serious form of skin cancer, says a dermatologist.
But a new appearing dark spot on the lip can have benign causes.
The older you are, the more concerning a new appearance of any kind of “freckle” or “mole” is.
Dr. Janet Prystowsky is a board certified dermatologist in New York, NY, with 30+ years’ experience.
She says that a dark spot on the lower lip usually is not a melanoma, but at the same time, you should have a dermatologist obtain a biopsy.
“Lip cancers metastasize [spread] more readily than other skin cancers,” says Dr. Prystowsky. A melanoma on the lip, therefore, “has a much higher risk of causing death.”
Do not let fear of a scar from a biopsy stop you from getting this procedure done.
A dark spot on the lip is suspicious for melanoma if it has the following features, says Dr. Prystowsky.
It’s new, rather than always having been there for as long as you can remember. As mentioned, concern is heightened the older you are.
“Has it been growing or changing in some way?” she questions. If the answer is affirmative, this could signal a problem.
Bleeding is another factor. If you pick at a benign lesion, it could bleed, but in melanoma, the bleeding comes more readily.
“Does it have an irregular appearance or border?” asks Dr. Prystowsky.
If you bisect it from any point, are the sides notably unequal?
Does the border look serrated or erratic?
Is it more than a few millimeters, and especially, has it been getting bigger over just a few months?
Does this dark spot on your lip have one or more other colors in it? For instance, is part of it blue, white or red?
Don’t try to self-diagnose.
Though the absence of some features may bring reassurance that the dark spot on your lip is not a melanoma, only a biopsy could rule it out for sure, though the benign “venous lake” (blood vessel concentration that forms a dark spot) can be diagnosed without a biopsy. A “melanocytic macule” is also benign.

In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/New Africa

Small White Itchy Bumps on Palms: Explanations

The good news is that cancer does not cause little itchy white bumps on the palms.
The not-so-great news is that it may not be easy to find out what’s causing this very annoying symptom.
There are several possible causes of small, itchy white bumps appearing on your palms, says Dr. Janet Prystowsky, board certified dermatologist in New York, NY, with 30+ years’ experience.
She explains, “Small white bumps on your palms are usually flat warts, although they may not itch.”
Warts are caused by a viral infection with the human papillomavirus (HPV).
These warts are typically smooth and only slightly elevated, making them less noticeable compared to other types of warts.
Flat warts, which can appear in clusters, are common and can spread through direct contact with infected surfaces or from person to person.
“Dyshidrotic eczema commonly occurs on many people’s palms,” continues Dr. Prystowsky.
“It is a collection of fluid-filled bumps that look like tiny, flesh-toned blisters.”
The little bumps of dyshidrotic eczema may also have a slight pinkish tinge.
These can itch like mad and may also appear on the edges of one’s fingers, toes and the bottoms of the feet.
The image below shows dyshidrotic eczema on a finger.

dyshidrotic eczema, Maslesha,CC BY-SA
Dyshidrotic eczema — which you should never scratch — has no cure but it’s manageable with proper care. The condition is not contagious.
If the situation with your palms can accurately be described as “lots of very small white-flesh, flesh-toned or flesh-pink colored bumps that itch,” then it’s a good bet that you have dyshidrotic eczema.
A dermatologist can easily make the diagnosis.
Dr. Prystowsky adds, “Contact allergen may also cause fluid-filled, flesh-toned bumps on the palms and sides of your fingers.”
Take inventory of any chemicals that might be coming in contact with your hands throughout the day. This includes household cleaners.
If you’re wondering if the problem is poison ivy, Dr. Prystowsky says, “Poison ivy rashes, however, do not usually cause a reaction on the palms or soles.”
It’s important to see a dermatologist to get the precise diagnosis.
Don’t Make the Itching Worse
The itching could be quite annoying with these conditions — but it can’t be said enough: Do not scratch!
When you scratch an itch, it activates certain nerve endings in the skin, which can initially provide temporary relief by interrupting the itch signal.
However, this action also stimulates additional nerve receptors and increases the release of inflammatory substances such as histamine.
The more you scratch, the more those small, white bumps on your palms will itch, regardless of their origin.
Additionally, scratching can damage the skin, leading to further inflammation and irritation, which can intensify the itch.
In combination with her focus on early skin cancer detection and removal, Dr. Prystowsky provides a wide range of revitalizing and rejuvenating treatments.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

6 Excuses Parents Make for Their Out of Control Children

Classic Statements that Parents Make that Are Code for “I can’t control my kids!”
Parents who can’t or won’t control their children almost always hide behind age-old statements in an effort to get off the hook.
Over the years, I’ve heard these half-baked statements, and I’m sure you have too, that parents make when they’re in denial that they have no control over their kids.
Remember, it’s never the young child’s fault. People call out-of-control or rude kids “brats” and other not-so-nice names, but the way that children behave is directly the result of how their parents are raising them. So cut the young ones some slack.
“Kids will be kids.”
This is as old as the hills. Funny thing, though, when parents use this line, they’re very selective about it.
If they truly believe that kids will be kids and therefore, let’s let them get away with doing whatever they please — then why not let them eat whatever they want? Ice cream for dinner and never any vegetables, for instance?
And let them get filthy from playing in a mud puddle and let them put glue in their hair while you’re at it. After all, kids will be kids!
“You obviously don’t have kids.”
This remark comes from parents who believe that every parent on earth thinks exactly as THEY do, and anybody who disagrees is childless. This is binary thinking and totally lacks logic.
The message with this defense is that in order to recognize that a child is out of control or behaving badly or inappropriately, the observer absolutely must have children of their own.
The funny thing is, is that often, this defense is directed towards people who do, indeed, have children—simply because most adults have kids!
“She’s just a free spirit.”
Letting your child be a free spirit is great (think running in the park flying a kite), but being permitted to dash all about a restaurant like a pinball and shriek and holler, disrupting diners’ eating experience, doesn’t qualify as free spirited.
That’s like calling your child a “free spirit” when they decide to splatter paint on your new $500 sofa.
“You know how little boys are.”
How are they? Are they supposed to trample the neighbor’s flower bed?
Are they supposed to chase each other in and out of store aisles, nearly colliding with customers?
“It’s good to let kids express themselves.”
True, so that’s why wise parents will buy their children implements for expressing themselves such as art supplies, musical instruments, a diary and sign them up for various classes like clay working, water color painting, jewelry making, woodworking, dramatic arts, etc.
But running haywire through a health club while people are working out? This is an out-of-control child whose parents have their head in the sand.
Otherwise, why not give this same excuse to adults who are wild and loud?
What if your adult neighbors are hollering and whooping it up at 10 pm on their porch, the heavy metal music cranked up?
What if when you asked them to tone things down a bit, they responded, “We’re just expressing ourselves!”?
“I suppose YOUR kids are perfect?”
The behavioral nature of the critic’s children is not relevant to the matter at hand.
It’s not relevant to, for example, someone’s five-year-old shrieking and bouncing all over the lobby at the DMV because the child’s mother has her thinking it’s a playground.
Allowing the little girl to behave this way is wrong, whether the critic’s own five-year-old trampled the neighbor’s garden yesterday or not.
“Sometimes parents will minimize their children’s behavior by saying things like, ‘He was just playing when he hit her,’ or, ‘She watches a lot of television and that is where she learned to swear,’” says Stacy Kaiser, a southern California-based licensed psychotherapist and relationship expert with a special interest in the topic of bullying.
Kaiser explains, “Oftentimes, parents will just throw up their hands and imply that they have no control over their children and they simply do not know what to do.
“This is a way of denying responsibility and acting as if their child is outside of their control.”


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}