

Explanation for how a heart attack can happen with or without a blockage:
Why blockages of only 30-50% are a higher risk for a catastrophic cardiac event than severely blocked arteries are.
It’s hard to believe, but it’s true: A big heart attack is more likely to occur when a person has a 30-50% blockage in their coronary arteries than if they are over 70 percent blocked.
But this phenomenon refers to a particular cause of the heart attack.
“A heart attack is when heart muscle cells die,” says Dr. Alvaro Waissbluth, MD, a cardiologist with Alameda Health System in CA.
He continues, “Heart muscle cells die when they don’t get enough oxygen or nutrients or if they get attacked by something and destroyed.” There are basically three kinds of heart attacks.
Heart attacks can happen with or without a blockage.
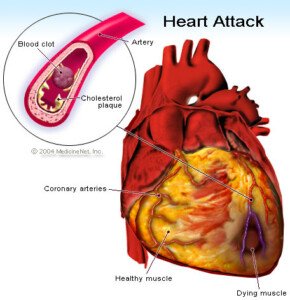
A plaque rupture in the coronary artery can cause a complete “mechanical interruption in the flow of oxygen and nutrients to the [cardiac] muscle,” says Dr. Waissbluth.

Shutterstock/eranicle
Plaque buildup (the “clog” in arteries) results from numerous insults including smoking, lack of exercise, high sugar intake, diabetes and, to some extent, genetics.
Imagine the sludge of plaque gradually building up over time, decreasing the inner diameter of the artery, eventually to a pinpoint diameter—where only a hair-width stream of blood could get through.
And then eventually, the buildup reaches that critical point where the pathway gets sealed off: a complete obstruction, depriving the heart muscle from any blood flow.
Most heart attacks do not occur this way, says Dr. Waissbluth. This doesn’t mean they can’t.
My mother was in danger of this very scenario (as shown on a catheter angiogram). She was 99 percent blocked and had to have emergency bypass.
Dr. Waissbluth explains, “Most heart attacks occur when a plaque blockage is in the 30-50% range and the outer layer of the plaque gets a small tear in it – a rupture.
“This usually happens along the edges of the plaque where they are the softest – called the shoulder region.
“Plaques can range from very soft to very hard depending on how new they are and how much activity they have inside; the inside of a plaque is a very active area – there are white blood cells which absorb fat cells that have snuck into the vessel wall.
“These white cells also produce various inflammatory mediators that cause the plaque to get bigger and also eat away at the edges of the plaque – there are also often blood clots and platelet plugs that form inside these plaques – lots going on.
So why is less buildup (a relatively cleaner artery) a higher risk of a plaque rupture and thus heart attack?
“The longer a plaque has existed and the bigger the plaque, the more stable its surface tends to be,” says Dr. Waissbluth.
“That’s why more major heart attacks happen from plaques occluding 30-50% of the artery than plaques occluding, say, 80% of an artery…the 30-50%’ers are newer and tend to have more active insides and softer outsides – which makes them more likely to rupture.”
Wow! This may explain why the 90-year-old man whose calcium score is a whopping 1,200 (zero indicates zero plaque buildup) has never had a heart attack.
The calcium score procedure measures the amount of hard (calcified and stable) plaque, not the amount of soft (newer and unstable) plaque.
Dr. Waissbluth explains, “When a rupture occurs, your body tries to fix it by creating a plug – just like if you cut your arm you will develop a clot and a scab – this also happens on a ruptured plaque.
“Most of the time the plug seals the tear and then the plaque is fixed and nothing happens.
“BUT if the plug grows and grows it can get very large and shut down the entire artery, and this is how a major heart attack happens.”
Let’s cut in here for a moment. Are you flabbergasted that a 45-year-old person, who hasn’t lived long enough to develop an 80% blockage — and hence is only 30-50% blocked — can actually be at higher risk of a heart attack than is your average 90-year-old?!
And if so, then why aren’t middle-aged and younger adults dropping like flies from heart attacks?
Why are heart attacks much more rampant among people over age 65?
Keep in mind that the age-related risk for heart attack actually begins at 45 for men and 50 for women.
“First and most important, the 90 year old has a lot more 30-50% blockages than the average 45 year old – the older you are the more plaques you get,” says Dr. Waissbluth.
Secondly, by the time a person is old, their heart has been subjected to many factors that could cause or greatly increase the risk of heart attack, whether or not they have excessive soft plaque.
Third, many people under 50 have either a zero calcium score or an indication of only mild heart disease (30-50% is moderate). Keep reading…

Heart attack symptoms
“The 80% blockage is more likely to cause chest pain while you’re exerting yourself but less likely to rupture,” says Dr. Waissbluth.
It’s less likely to rupture because it’s more likely to be made of hard calcifications.
“The 40%’er will probably never cause pain with activity [because there’s still a relatively wide inner diameter of the artery for blood flow], but is more likely to rupture and cause a big heart attack.”
That’s because the sludge buildup hasn’t been around long enough to calcify much.
Science still can’t pin down the cause of plaque ruptures; only what increases the risk (e.g., smoking, junk food diet, lack of exercise).
In the second type of heart attack there’s no plaque rupture, but there’s reduced blood flow to the heart muscle.
Enough reduced blood flow = heart muscle cells die = heart attack.
“But these aren’t typically as catastrophic or deadly as the major heart attacks from plaque rupture occluding the entire artery,” explains Dr. Waissbluth.
The reduced blood flow results when the supply-demand imbalance becomes too great. The supply of blood cannot keep up with the demand for it.
The inadequate supply may be due to bleeding, anemia, or weak pumping of the heart.
The excessive demand may be caused by a fever/infection, high blood pressure, physical injury elsewhere in the body or physical exertion (like shoveling snow).
These cause the heart to beat faster and harder; in turn the heart muscle cells demand more and the blood supply from the heart arteries simply can’t keep up: So cardiac cells die—a heart attack—without a new blockage.
“These kinds of heart attacks can happen in people with completely normal arteries – no plaques at all, or in people with plaques,” says Dr. Waissbluth.
An elderly person is far more likely to experience this situation “due to having more fixed blockages than a younger person – even if the blockages did not change. The change in demand caused the blockages to become physiologically relevant.”
Put another way, the cumulative effect of fixed (stable) 30-50% blockages interfers with the net amount of passageway through which blood flows.
Think of how water flow would be stunted if many wads of gum were stuck throughout the inner walls of a pipe.
“If you create a supply/demand imbalance and you happen to have a 75% blockage, then you are more likely to have a heart attack than if you had a 40% blockage or no blockage at all.
“But yes these kinds of heart attacks can happen with little or no blockages too.
“The last kind of heart attack is when a virus or your own body’s white cells and immune system attack the heart muscle cells without any change in the arteries or in the supply/demand.”
Now you know why a heart attack can happen without a blockage, and why the risk of heart attack goes up with age, even though younger people are more likely to be 30-50% blocked than severely blocked.


































