

Can the Burning Pain in Your Upper Back Be Caused by GERD ?

Unexplained pain of any type in your upper back needs to be checked by a doctor, since this can mean an imminent heart attack – or just some GERD or even occasional heartburn.
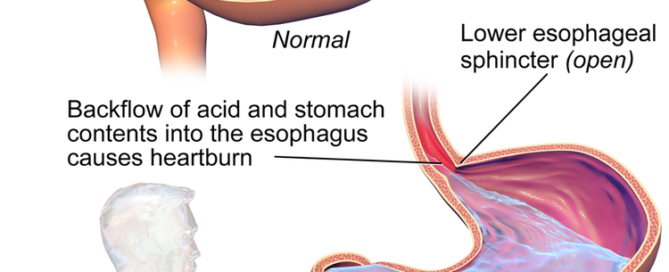
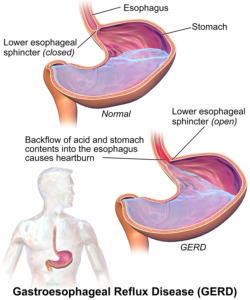
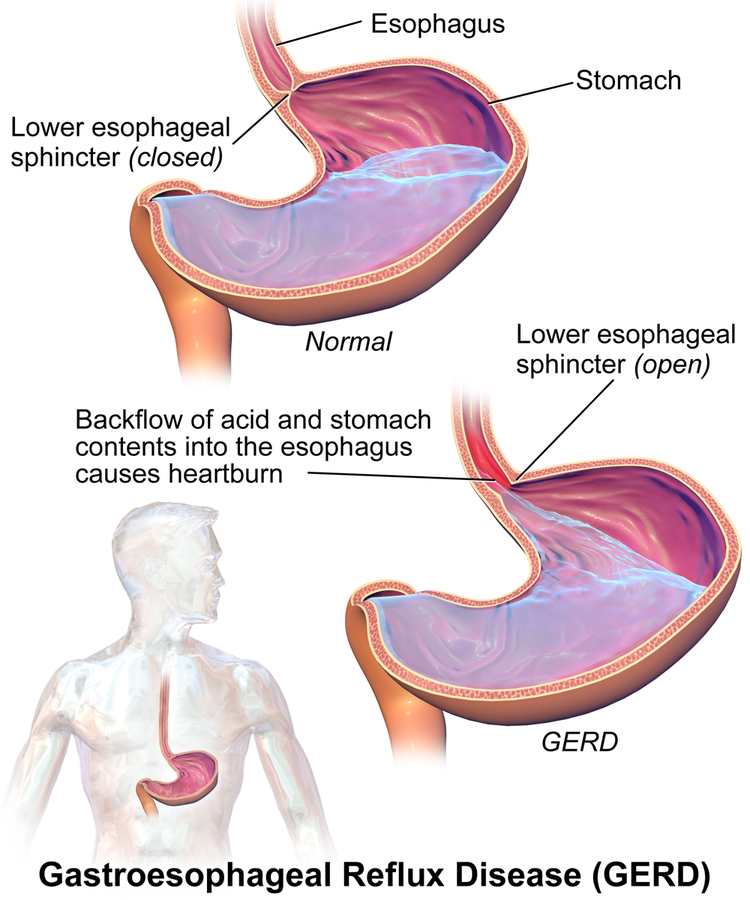
GERD stands for gastroesophageal reflux disease and is not the same as periodic heartburn or acid reflux.
GERD is when the acidic contents of the stomach reflux upward into the esophagus (the so-called food pipe) on a chronic or ongoing basis.
Over time this can lead to a condition called Barrett’s esophagus, which is a risk factor for esophageal cancer.
The hairy problem with GERD or occasional heartburn is that both can cause chest pain – which scares people into thinking they’re either having a heart attack or have something else going on with their heart.
“First and foremost recurrent chest pain should be examined by a physician to rule out heart disease,” says John P. Geibel, MD, Professor of Gastrointestinal Surgery at the Yale University School of Medicine.
GERD, acid reflux and a pending heart attack or even stable angina (deprived oxygen flow to the heart upon physical exertion) can also cause pain in the back.
Dr. Geibel explains that “acid reflux can and most often leads to irritation of the esophagus lining that causes mild to severe erosion that can give a widespread burning pain that affects the chest, abdomen and sometimes even the upper back.”
Upper back pain can be caused by an assortment of medical conditions, and even though it can be caused by acid reflux, this is not common.
However, if you’ve noticed that your upper back pain occurs only when you experience occasional heartburn (and a heart problem has been ruled out), see what happens when you begin treating this heartburn.
TummyZen is an over the counter zinc-based formula that’s validated by Dr. Geibel’s research.
TummyZen provides fast relief that lasts for hours and also supports the esophageal lining.
With the lining of the esophagus being supported by the zinc salts, this will help prevent the back pain caused by acid reflux.
TummyZen is for occasional heartburn rather than for GERD and is minus the side effects typical of PPI drugs.
Dr. Geibel is the author of over 250 publications and presents his research findings both nationally and internationally, and has made the America’s Top Doctors list numerous times.
is the author of over 250 publications and presents his research findings both nationally and internationally, and has made the America’s Top Doctors list numerous times.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/staras

Can Walking Too Long on a Treadmill Harm Your Knees ?

Just how much must you walk on a treadmill before this becomes potentially harmful to your knees?
Of course, this assumes that you have healthy knees to begin with, rather than the painful bone-on-bone disease of osteoarthritis and in need of knee replacement surgery. (more…)

What Never to Say to Women with Permanent Hair Loss from Chemo
To some women, their hair is a beloved part of their identity, and permanent hair loss from chemo is nothing short of devastating, especially if their hair was previously thick and glorious. (more…)

Skinny but Stomach Still Fat? Exercise vs. Diet for Solution

A thin person who’s healthy should not have a fat stomach.
Usually, the excess belly fat in an otherwise thin individual is caused by a problem with their exercise routine.
This article is about healthy people who have slender legs and arms, but mysterious pudge or rolls in their midsection.
They can pinch a lot more than an inch, and their belly and waistline feel like bread dough.
Sometimes there are literally rolls of fat, yet their legs are lean and may even be firm.
What in the devil is going on?
Let’s assume that such an individual is healthy, since there are medical conditions that can cause distended bellies.
The skinny but stomach is fat phenomenon is more prevalent in people over 40.
But I’ve seen plenty of it in 20-somethings.
Cause of Fat Belly in a Skinny Healthy Person
Quite simply, it’s lack of muscle tissue. This becomes very easy to understand when you ask yourself the following questions:
• Have you ever seen a person with “ripped” shoulders, arms and legs, but a doughy bloated belly of pudge?
• Have you ever seen a person with ripped abs and a tight trim waistline, but pudgy arms and doughy soft legs?
Muscle is the body’s best fat burner.
The more muscle you have, the faster will be your resting metabolism.
The solution is to lift weights and build muscle to stoke your resting metabolism.

Shutterstock/BLACKDAY
The body will siphon the fat in your stomach to subsidize muscle growth that’s needed to support a weightlifting program!
Do not think, “I must bulk up to get rid of my fat stomach!”
Exercise vs. Diet
- Cutting calories will not add the muscle that your thin-side body needs to boost metabolism.
- Eating more fresh produce and protein will not build more muscle — your body’s metabolic furnace — though a clean plant-based diet with adequate protein should be part of a muscle-building plan.
When I was a personal trainer, I saw the chubby stomachs of my clients shrink as they increased lean muscle mass in their legs, back and chest. No sit-ups or crunches were necessary.
A program for building lean muscle tissue will raise your body’s energy needs.
Unless your diet is too caloric, your body will pull much of this energy from stored body fat.
This is what causes the stomach to shrink. You just pummeled your legs in the gym with weights. Your muscles are now screaming for recovery energy.
Where is that energy stored?
Your belly. Your belly will shrink as you increase lean muscle tissue and adopt healthy eating habits.
This means after a thrashing back and chest workout, you don’t go running off to Dairy Queen and getting a double cheeseburger and Blizzard.
You instead have a chicken salad sandwich on two slices of whole grain bread and some fruit.
I can go on and on about diet, but this post is about why exercise wins over diet when it comes to shrinking a fat stomach.
Ever notice that competitive bodybuilders, of all athletes, have the tiniest waists?
That’s because all that muscle prevents fat accumulation in the stomach and waistline – just barely enough for functional purposes.
Bodybuilders go on strict “cutting” diet phases to prepare for competition or photo shoots, but even when they’re not in competition mode or doing any fitness modeling, they can maintain very small and tight waists and stomachs by maintaining the muscle mass and controlling their diet.
However, you need not sculpt your physique into competitive caliber to dramatically shrink your stomach.
But I point out the bodybuilders so that you can appreciate just how effective increasing muscle mass is for melting off stomach fat.
If you’re already kind of skinny but have a plump belly, dieting is not the solution. Exercise is.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Suwan Wanawattanawong

“You’re So Fat” vs. “You’re So Tall”: Which Is Ruder?

Being told “You’re so fat” should never be compared to being told “You’re so tall,” even though many tall women equate these comments from strangers. (more…)

Is 5’9” the Height Cut-off when Tall Women Won’t Get Comments?

Tall women the world over get comments and questions (some of them rude or stupid) about their height—even from strangers, but what about 5-9 women? (more…)

Why Does Acid Reflux Cause Pain in the Upper Back?

Pain in the upper back along with more common acid reflux symptoms might actually be a sign of heart trouble.
The upper back pain may be a coincidence and totally unrelated to the acid reflux or heartburn. (more…)

How to Convince Elderly Parent to Go from Walker to Scooter

At what point should an elderly parent, prone to falls, go from walker to scooter? After they take a hard fall that kills them?
This is a vexing situation, a slippery-slope dilemma that many mature adults face with their elderly parents. (more…)
Ensure and Boost Will NOT Help GERD or Cause It
Ensure and Boost can be thought of as glorified liquid candy, which is why it’s no surprise that these sugary drinks cannot treat GERD in any way.
A lot of GERD sufferers and those with the occasional heartburn or other symptoms caused by acid reflux would like to know if Ensure (or its mimicker, Boost) can help tame the symptoms.
I have no idea where this idea came from, because Ensure and Boost – though touted as healthful – are literally liquid candy.
Just read the ingredients!

“I am not aware of any evidence that those products can cause or help relieve acid reflux,” says Lauren Gerson, MD, board certified gastroenterologist formerly with California Pacific Medical Center in San Francisco.
Dr. Gerson is a nationally recognized researcher in the field of general gastroenterology including management and treatment of GERD.
Don’t reach for the Ensure or Boost to treat your heartburn any more than you’d reach for a candy bar.
People with occasional bouts of acid reflux need to figure out what their trigger foods are and avoid them. Overeating, too, is a trigger.
Dr. Gerson lists the following foods as potential causes of acid reflux:
“Coffee, tea (caffeinated or decaffeinated) and other carbonated beverages; fatty, fried or spicy foods; and other foods such as chocolate, peppermint, tomatoes, citrus fruits, garlic and onions.
“If symptoms persist after making these diet changes, it is important to speak with your doctor because there are long-term treatment options that can help.”
Ensure is targeted towards older people who don’t get enough nutrition. Boost is very similar.
These products, though laden with synthetic ingredients, have their place for people who are losing too much weight due to a refusal to eat.
For example, when my mother was disabled by clinical depression, she didn’t want to eat, but found it tolerable to sip through a straw an entire bottle of Ensure or Boost – a quick 350 calories that she desperately needed. Meanwhile she wouldn’t even eat a single slice of bread.
But remember, Ensure, Boost or similar products have no place in the treatment of heartburn or other symptoms caused by acid reflux.
Dr. Gerson passed away in July 2017 after a valiant battle against metastatic melanoma. Dr. Gerson devoted herself to solving her patients’ most difficult and longstanding health challenges.
passed away in July 2017 after a valiant battle against metastatic melanoma. Dr. Gerson devoted herself to solving her patients’ most difficult and longstanding health challenges.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Bruce Blaus
Hoarse Voice Causes: from Cancer to Reflux to Enlarged Aorta
Throwing up in the Mouth While Asleep: Benign Cause, Solutions

Can Secondhand Smoke Cause Acid Reflux?

With all the problems that secondhand smoke has been linked to as well as proven to cause, it would be no wonder if it also can cause acid reflux.
If you’re exposed to secondhand smoke and seem to think this is triggering episodes of heartburn or acid reflux, you’re in for a surprise:
“There is no sufficient evidence that smoking [and secondhand smoke] causes heartburn or acid reflux, although it may relax the lower esophageal sphincter pressure in some patients,” says Lauren Gerson, MD, board certified gastroenterologist formerly with California Pacific Medical Center in San Francisco.
She is a nationally recognized researcher in the specialty of general gastroenterology including management and treatment of GERD.
Dr. Gerson adds, “However, there have been studies showing that smoking and secondhand smoke cessation does not alleviate acid reflux.”
Avoid secondhand smoke as much as possible. It doesn’t cause heartburn, but if you’re around it enough, it will raise the risk of lung cancer. It will also make your clothes, hair and skin stink.
Meanwhile, if you’re suffering from the symptoms of acid reflux, see a gastroenterologist if you already haven’t.
A doctor can recommend the right treatment that will help alleviate your acid reflux symptoms, which by the way, can actually make their way to the throat and cause a condition known as LPR: laryngopharyngeal reflux disease.
This can cause unnerving symptoms that mimic serious diseases.
Dr. Gerson passed away in July 2017 after a valiant battle against metastatic melanoma. Dr. Gerson devoted herself to solving her patients’ most difficult and longstanding health challenges.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}