

Bulbar Onset ALS vs. Normal Tongue Twitching

Does a twitching tongue have you fearing you might have bulbar onset ALS?
When a person initially becomes aware of tongue twitching, he or she normally has no idea what bulbar onset ALS even is.
The problem arises when the person does an Internet search on tongue twitching, and links to ALS sites come up in the search results.
The individual immediately sees, upon scanning the search results, that a twitching tongue can be a sign of bulbar onset ALS.
Another way this is discovered is when the individual is already aware of muscle twitching being a symptom of ALS, due to having done an Internet search on twitching muscles one day — and seeing ALS links come up in the search results.
They fixate on possibly having this neurological disease, learning about bulbar onset along the way.
Then one day they notice a twitch in their tongue, and so begins a fixation on the bulbar onset version.
If you’ve clicked on this article, then you already know that this motor neuron disease is an incurable, fatal affliction in which muscle twitching is a symptom.
The tongue is a muscle, and, like any other muscle in the body, it can be prone to twitching for benign reasons.
Bulbar onset ALS is an extremely rare condition, afflicting about 10 percent of ALS victims, and this motor neuron disease overall is a rare disease, with about 5,600 cases diagnosed yearly in the U.S. What’s 10 percent of that?
Only about 600 people per year in America are diagnosed with bulbar onset.
If you’ve noticed a twitching tongue lately, it would be quite irrational to jump to the conclusion you might have bulbar onset ALS.
Remember, the tongue is a muscle, and muscles, by nature, are prone to twitching for benign reasons such as fatigue, stress, dehydration and mineral imbalance.
There is far more to bulbar onset ALS than the twitching tongue.
“ALS with bulbar onset is unusual but presents with subtle speech changes and difficulty controlling chewing/swallowing of various consistencies of food,” says Kristina Lafaye, MD, a board certified neurologist specializing in clinical neurophysiology and neuromuscular medicine with Tulane Doctors Neurosciences.
Dr. Lafaye continues, “This is also a gradual process. There is coughing which may prompt consideration of a respiratory condition such as asthma or COPD.
“Unless an individual is having the aforementioned symptoms, then they do not have bulbar onset ALS.”
In short, if you’ve developed the habit of persistently examining your tongue in a mirror, you are wasting valuable time if your only symptom is twitching.
You may be perceiving difficulties chewing and swallowing food, but there is a huge difference between perception and performance.
If the food is getting chewed in a reasonable amount of time, and swallowed without gagging and choking, then you do not have bulbar onset ALS.

Dr. Lafaye is triple board certified: neurology, clinical neurophysiology and neuromuscular medicine from the American Board of Psychiatry and Neurology. Her expertise and leadership continue to make a significant impact on patient outcomes.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Hit Head? Bleeding in Brain Symptoms Can Occur Six Weeks Later

If you hit your head and don’t have immediate symptoms or even symptoms for a few weeks after, you can still develop symptoms of bleeding in the brain at least six weeks later that are the direct result of hitting your head.
Hit your head but everything is fine and you have no symptoms?
Mark the date you hit your head because you can still develop symptoms weeks later – six weeks later, even, from a very slow bleeding in your brain caused by the blunt trauma to your head.
This is what happened to my mother.
She blacked out (from a blood pressure drop) while standing in the bathroom, and collapsed from the loss of consciousness (which lasted only moments, but long enough to turn her body into dead weight) — hitting her head on the bathtub on the way down.
I heard the awful “THUD!” and rushed into the bathroom to see her lying on the floor (conscious), with her shoulders propped up against the side of the bathtub.
There was no way she could have ended up like that without hitting her head.
I examined her head and discovered a generous-sized matting of blood in her hair.
A few hours later in the ER she had a CAT scan that was normal.
The CAT scan was to see if there was bleeding on her brain (subdural hematoma).
Up to that point my mother reported no symptoms, not even a headache.
There was no nausea, dizziness, unsteadiness, slurred speech, vision problems or change in mental status.
She stayed overnight for observation and next morning, another CAT scan was normal.
I expressed concern about the possibility of a very slow bleeding that might start showing symptoms “a few months out.”
But the ER doctor said the chances of this were very tiny, and that the next-morning CAT scan results were very encouraging, and that there probably wouldn’t be any complications — but to keep a close watch on my mother over the next few days.
Over the next few days I kept a close watch: no symptoms, no headache, gait problems, slurred speech, cognitive changes, nothing.
I then completely forget about the idea that her hit on the head could cause any bleeding in the brain.
Until 6.1 weeks later.
The symptoms came out of the blue. She awakened at 7 am with a headache so bad that she was weeping.
It persisted. I did not connect the dots and think of the fall on her head six weeks prior.
I just thought it was one of her bad headaches (every now and then my mother has always reported a bad headache), and that the weeping was just her being overly-sensitive (she’d had quintuple bypass surgery 12 week prior and the recovery had been very bumpy).
The headache was so bad that my mother was unable to get ready for the day.
But I noticed that she had difficulty walking across the room; very weak. Then she upchucked.
Then I noticed her left leg had a slight drag to it.
It still did not occur to me that these symptoms were the result of a slow, delayed brain bleed from hitting her head six weeks ago. Instead, I thought it was a mild stroke.
So did the ER doctor. A CAT scan was ordered and the surprised ER doctor informed us that there was bleeding in the brain.
“Did you hit your head recently?” She asked my mother.
I said she fell about six weeks ago and hit her head on a hard surface.
The diagnosis was a chronic subdural hematoma.
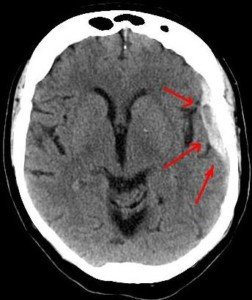
Arrows show the bleeding in a patient with head trauma. Source: Lucien Monfils
And ultimately, the medical reports from two ER visits (this one and another one when the brain bleed recurred after the fluid was drained) named the fall in the bathroom as the cause of the chronic subdural hematoma.
Between the time my mother had hit her head, and the night before she awakened at 7 am with an excruciating headache, she had shown absolutely no symptoms characteristic of bleeding in the brain or head injury!
“Yes, everyone who hits their head traumatically should be evaluated by a physician,” says Danielle DonDiego, DO, a family physician with SteadyMD, an online program where patients can call, text or video chat with their doctor anytime.
“If there is any loss of consciousness, ‘worst headache of their life,’ confusion, feeling faint or vision changes — these are all major signs to go to the ER immediately.
“Even if someone loses consciousness and regains consciousness quickly, they could still have a head bleed that can be deadly. It’s always best to be evaluated,” especially if the individual is elderly, even if initially they don’t seem to have any symptoms and insist “I’m fine.”
Dr. DonDiego continues, “If a CT head is negative initially, especially in the elderly or someone taking blood thinners, and a slow worsening headache persists for days to weeks, it is possible there is a slow bleed, and a re-evaluation is necessary.
“Our veins weaken as we age, so they are likely to be higher risk for hemorrhages.”
If someone hits his or her head, they should record the date.
Any peculiar symptoms that occur even weeks later should be documented.
This includes nausea, vomiting or lingering dizziness.
A normal CAT scan 24 hours after getting hit in the head doesn’t mean that bleeding in the brain won’t eventually occur.
 Dr. DonDiego, who’s also a certified personal trainer, focuses on weight management, fitness, nutrition, reproductive health, preventive medicine and managing end stage disease. Learn more about SteadyMD.
Dr. DonDiego, who’s also a certified personal trainer, focuses on weight management, fitness, nutrition, reproductive health, preventive medicine and managing end stage disease. Learn more about SteadyMD.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik
Muscle Twitching Help; Foot Drop Strength Tests & ALS

If you have muscle twitching and have googled twitching muscles, you’ve most likely stumbled upon some links for the deadly disease ALS.
You now might think you have ALS, since muscle twitching is a symptom of the incurable ALS.
But if you read more about ALS, you’ll come upon information that indicates that muscle twitching comes after muscle weakness.
However, you may now suddenly be experiencing what you believe to be weakness in your muscles.
In ALS, one of the first muscles to go is often that which controls foot movement, particularly up and down movement: clinical muscle weakness.
The muscles that control the joint action of dorsiflexion no longer work, and thus, the foot becomes limp.
A person suffering from fear he or she has ALS might start thinking they have this foot drop.
If he stumbles upon bunched-up carpet, right away he’ll think foot drop.
They’ll perform endless strength tests for these muscles to check for the drop, and no matter how well they do these muscle strength tests, they’ll never be assured that they don’t have ALS.
Strength Tests for Foot Drop Obsession and ALS Fear
“If a patient has a foot drop, they would not be able to perform any active exercise, meaning any exercise that can be performed unassisted or that would require resistance such a standing on one’s toes or utilizing a resistance band to stretch out the calf,” explains Dr. Alan L. Bass, DPM, Medical Director of NEMO Capital Partners, LLC.
Using the Foot Pedal While Driving
Yes, as simple as this is, a person with ALS foot drop will not be able to do this efficiently.
This action requires continuous dorsiflexion, the very muscles that, when healthy, prevent foot drop.
Though these muscles don’t work hard to operate the car’s pedal, the continuous use of these muscles is significant.
This test applies only if the person already normally uses the foot on the pedal (depending on driving habits).
Stair Jumping
Stand at bottom of staircase. With both feet at the same time, jump to next step. Land with both feet at the same time. Repeat to the next step. Go all the way to the top.

Shutterstock/G-Stock Studio
This isn’t a fitness test. It’s a “Can I even do this?” test. If you’re clumsy (and you WILL be, due to anxiety of passing this test), this doesn’t matter, because MOST people cannot do this without a little (or even a lot) of clumsiness.
As a fitness trainer I’ve had only a few clients who were able to smoothly hop up a flight of stairs: boing boing boing boing boing.
Other clients were sloppy and uncoordinated. A person with ALS foot drop will NOT be able to what the women in the image above are doing.
Standing on One Foot
Muscles required to do this are the same that prevent foot drop.
If you can stand on one foot, it’s time to stop obsessing about ALS. If you stand on one foot, you’ll feel these muscles at work.

ShutterstockJacob Lund
Expect to lose balance quickly the first several attempts, because anxiety will loom. But keep at it and sooner or later you’ll find yourself balancing nicely.
A person with ALS foot drop will NOT be able to balance and improve, no matter how many times they attempt it.
Stair Running
Run up the stairs as fast as possible, then down. If the muscles that control dorsiflexion are dead, you won’t be able to do this…at all.

Shutterstock/Vadim Martynenko
Seated Ankle Flexion
Have a seat on the floor as shown below. If your “weak” foot can’t flex to match your “good” foot, then there IS a drop problem — but it can have many causes.

Pagemaker787/CreativeCommons
If you can perform all of these routines (regardless of clumsiness or number of attempts required), then you can free yourself of ALS panic, assume your twitching muscles are healthy, and that the foot drop is all in your imagination.

Dr. Bass is with Central Jersey Foot & Ankle Care, and is a Fellow of the American College of Foot and Ankle Orthopedics and Medicine.
basspodiatry.com/our-foot-doctor
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Multiple Sclerosis vs. Sjogren’s Syndrome Symptom Comparison

Sjogren’s syndrome can be misdiagnosed as multiple sclerosis; symptoms are similar.
Sjogren’s syndrome can actually cause symptoms similar to multiple sclerosis (MS).
Sjogren’s syndrome is an autoimmune disease that is commonly associated with dry mouth due to decreased salivary gland secretion, and dry eyes due to decreased lacrimal gland secretion.
However, SS (like multiple sclerosis) can become systemic, affecting many areas of the body, including the nervous system.
As a result, symptoms similar to multiple sclerosis can result from Sjogren’s syndrome.
“Neurological manifestations of Sjogren’s syndrome are protean (considerably variable). Parkinson’s-like is unusual, but MS-like is not uncommon,” explains Ali D. Askari, MD, Professor of Medicine – Case Western Reserve University; Chief, Division of Rheumatology – University Hospitals Case Medical Center; Director, Rheumatology – University Hospitals Case Medical Center. Because SS commonly affects the joints, specialists in this disorder are often rheumatologists.
“In one study 20 percent of patients with what was called primary progressive multiple sclerosis turned out to have Sjogren’s syndrome.”
MRI findings on the brain, says Dr. Askari, can be very similar between Sjogren’s syndrome and multiple sclerosis.
“Other important neurologic manifestations seen in Sjogren’s syndrome include Parkinson’s-like or hemi-Parkinsonism with movement abnormalities including stiffness and tremors.
“Although in Parkinson’s there are not much MRI changes, in Sjogren’s syndrome there are MRI changes of the brain and therefore it could be a very helpful differential diagnosis point.”
And this is because brain lesions are also seen with multiple sclerosis.
“Neurologists are paying careful attention to these possibilities, and in cases of abnormal demyelinating findings on the brain MRI, which looks like cotton balls or smaller, they check the laboratory tests for the presence of antibodies which are commonly seen in lupus or Sjogren’s syndrome.” SS, MS and lupus are all autoimmune diseases.
“We have seen a number of patients with those findings and we have treated most successfully.
“The problem is when the lesions (on the brain) are chronic and they have caused permanent damage to the nervous system and it is difficult to be treated.”
Here is a general symptom comparison between Sjogren’s syndrome and multiple sclerosis.
Multiple sclerosis. Freepik/brgfx
Both diseases can present with many more symptoms than in the following list; the list is to show the striking similarities between Sjogren’s syndrome and multiple sclerosis as far as symptoms:
Sjogren’s syndrome symptoms:
Difficulty with chewing, swallowing or talking
Joint pain
Fatigue
Difficulty walking
Tremors
Numbness and tingling
Balance difficulties
Kinesthetic awareness problems (sense of body positioning in space)
Electric shock sensations in the face
Multiple sclerosis symptoms:
Numbness and weakness
Fatigue
Tingling
Pain
Electric shock sensations that arise as a result of particular movements of the head
Unsteady gait
Tremors; difficulty with coordination
Note: Some SS patients do not experience debilitating issues.
For these individuals, the disease is cause for annoyance (e.g., dry eyes and mouth, dental decay), rather than disability.
Update: As of April 2024, Sjogren’s syndrome is now known as Sjogren’s disease.

Dr. Askari’s special interests include diseases of the muscles, fibromyalgia, general rheumatology, lupus and Sjögren’s syndrome.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Lightspring
Sources:
sjogrens.org/home/about-sjogrens-syndrome/symptoms
sjogrensworld.org/sjogrensdefn.htm
mayoclinic.com/health/multiple-sclerosis/DS00188/DSECTION=symptoms

Sudden Onset Dry Mouth Causes & Solutions

Out of nowhere I began developing dry mouth.
What can sudden onset dry mouth mean?
Could it mean the beginnings of Sjogren’s syndrome?
One day during the midst of working out at the gym, I began noticing that I was thirsty.
This might sound normal for someone working out, but for me, it was unusual.
I never crave water while lifting weights, but this time, I seemed to be thirsty and drank water.
I was still “thirsty,” and by the end of the workout, realized that this wasn’t actual thirst.
My mouth was dry. I didn’t think much of it until the day progressed and the dry mouth seemed to be getting worse.
There is an autoimmune disorder called Sjogren’s syndrome, and it’s characterized by a persistently dry mouth.
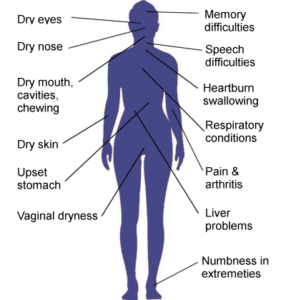
Symptoms that can be caused by Sjogren’s disease.
I wondered if I was developing Sjogren’s, because I already thought I might have a risk factor for it: microscopic colitis.
After being diagnosed with microscopic colitis, I learned that Sjogren’s is associated more with people who have microscopic colitis, though a definite link has not been established.
It’s actually not considered a risk for Sjogren’s, but still, my imagination went a little overboard.
The dry mouth was worse the next day, and the next, especially overnight.
It felt as though there was cotton in my mouth.
Drinking a lot of fluids was not the answer. This was not thirst. It was not dehydration.
Here is how you can tell the difference between dehydration and true dry mouth.
If you’re dehydrated or just plain thirsty, then the thought of a very chilled glass of your favorite thirst-quenching beverage will be extremely enticing.

Freepik.com/Racool_studio
If you have dry mouth, then imagining this tall, cold glass of your favorite drink won’t do anything for you.
I’d envision a tall ice-cold glass of lemonade, orange juice or water … and it did nothing for me; this confirmed (even though I already knew) that I had a mysterious case of really dry, cottony mouth.
My salivary glands weren’t working. I wondered if all four gland stations were being affected, or maybe two or three were.
If I deliberately held off on swallowing, this would allow some saliva to build up, but this didn’t correct the problem.
I also noticed that often, eating made the dry mouth worse, and my lips were also affected. The lips have salivary glands in them.
In Sjogren’s, biopsies of the lip are taken to diagnose for this disease.
On the fourth day I began placing a piece of diced lemon in my mouth to stimulate salivation, and this did a good job of relieving the dryness.

I’d keep the piece in there for a while, and when it was used up, I’d put another one in, and just keep it in there while working at the computer.
Funny thing, while working out at the gym, I noticed that the dry mouth subsided somewhat.
On the fifth day the dry mouth was noticeably suppressed, but I still sucked on a piece of lemon.
By night time there was a noticeable improvement, and on the sixth day, I no longer had dry mouth.
Causes of Sudden Dry Mouth
A sudden development of dry mouth is often caused by “salivary stones,” which are mineral deposits that settle at the salivary gland portal through which saliva is secreted.
But what is the origin?
“Dry mouth occurring in this way is usually the result of a nervous reaction, most commonly with a fit of anxiety,” says Morton Tavel, MD, Clinical Professor Emeritus of Medicine, Indiana University School of Medicine, and author of “Health Tips, Myths, and Tricks: A PHYSICIAN’S ADVICE.”
“I cannot think of any other or serious problems that could account for such a problem,” Dr. Tavel adds.
Often, the crystal-like debris resolves on their own. Other times, dentists must remove them.
One way to force these crystals to get lost is to suck on a piece of lemon.
This stimulates saliva production, and the saliva literally dislodges the crystals and hence, frees up the through-way for saliva, thus resolving the problem of dry mouth.
I took this assessment to my dentist at my next checkup, and she confirmed this process.

Dr. Tavel’s medical research includes over 125 publications, editorials and book reviews in peer-reviewed national medical journals. He was formerly director of the cardiac rehabilitation program at St. Vincent Hospital in Indiana. mortontavel.com
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/InesBazdar

Could Sudden Dry Mouth Be Sjogren’s Syndrome?

Has your mouth become cottony dry out of the blue, just like that? And is Sjogren’s syndrome constantly on your mind?
Sjogren’s syndrome is an autoimmune disorder that primarily affects the salivary glands and the lacrimal glands (responsible for keeping eyes moist), impairing the glands’ ability to produce fluids.
“Dry manifestations including the eyes and mouth can happen in the absence of Sjogren’s syndrome,” says Ali D. Askari, MD, Professor of Medicine – Case Western Reserve University; Chief, Division of Rheumatology – University Hospitals Case Medical Center ; Director, Rheumatology – University Hospitals Case Medical Center. Sjogren’s syndrome also often causes joint pain.
“There are a variety of other reasons causing dryness of the mouth and enlargement of the parotid glands that includes the stages before the development of Sjogren’s syndrome in total.”
Sjogren’s (pronounced show-grens) syndrome afflicts 2-4 million Americans. Ninety percent of patients are women, for reasons not known.
If you’re wondering if your dry mouth might be Sjogren’s syndrome, first make sure that what you’re experiencing is, indeed, dry mouth.
For first-time sufferers of dry mouth, this sensation can easily be mistaken for thirst or dehydration, especially if it’s mild.
However, an easy way to distinguish dry mouth from thirst (though it’s very possible to coincidentally have both at the same time), is to imagine a tall, chilled glass of your favorite, thirst-quenching beverage.
If this does something for you, you’re probably dehydrated.
If imagining chugging that chilled glass of lemonade, ice tea, soda or iced-up water doesn’t enthrall you, then you likely have dry mouth.
Another hallmark feature of dry mouth, when bad enough, is that it feels like cotton is lining the inner parts of your cheeks.
Plus, drinking large amounts of fluids won’t relieve the dry mouth, but will relieve thirst.
Dr. Askari continues, “In other words, dry mouth could be the first manifestation and one could take it in the context of the presence of other manifestations (of Sjogren’s syndrome) including Raynaud’s phenomenon, arthritis or arthralgia, skin rashes, neurological abnormalities, etc.
“Should all these findings be negative, then dry mouth may be a single problem due to age, dry air, mouth breathing, use of instruments for sleep apnea like what is called CPAP, and history of radiation to the neck and upper chest.”
Hundreds of prescription medications can cause dry mouth, and so can mineral deposits (salivary “stones”) that build up, blocking the secretion portals of the salivary glands. Salivary gland infection is another culprit.
“Furthermore, in somebody with only dry eyes and not Sjogren’s syndrome, the test for antibodies in the blood should be negative.
“These tests include anti-nuclear antibody, rheumatoid factor and specific antibodies of Sjogren’s syndrome including SSA and SSB.”
Update: As of April 2024, Sjogren’s syndrome is now known as Sjogren’s disease.
Dr. Askari’s special interests include diseases of the muscles, fibromyalgia, general rheumatology, lupus and Sjögren’s syndrome.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: ©Lorra Garrick

Why Does Ovarian Cancer Cause Appetite Loss?

A gynecological oncologist explains appetite suppression caused by ovarian cancer.
Ovarian cancer can suppress appetite; this is a hallmark feature of this disease, the deadliest of all gynecological malignancies.
I was wondering just what mechanisms are involved that make ovarian cancer lead to appetite suppression.
First of all, realize that if you’ve had a suppressed appetite lately, don’t torture yourself by jumping to the conclusion that you probably have ovarian cancer, which is very rare in premenopausal women.
“Advanced ovarian cancer can sit on the surface of the stomach or the intestines and this can make the patient feel full early,” says Diane Yamada, MD, Chief, Gynecologic Oncology, University of Chicago Medical Center.
“Tumors, extensively involving the omentum, known as an ‘omental cake,’ can also make the patient feel full all the time.”
The omentum is a fold in the abdominal cavity connecting the stomach to other organs.
Dr. Yamada continues, “This full sensation, called ‘early satiety,’ may suppress the patient’s appetite. Ascites fluid can also make the patient feel constantly full, which can suppress the appetite.”
In the case of ascites, which can result from ovarian cancer (and other malignancies such as pancreatic), and non-malignant disease processes such as cirrhosis of the liver, up to two liters of fluid may be present, suppressing appetite, causing a bloating feeling and creating visible distention or swelling of the abdomen.
“In advanced and recurrent ovarian cancer,” continues Dr. Yamada,
“Tumors can also cause a bowel blockage or obstruction, which may make the patient feel nauseous and not want to eat.”
Thus, once ovarian cancer begins causing suppression of appetite, the disease may very well have already spread beyond these walnut-sized organs, into the abdominal area.
Survival rates for ovarian cancer are dismal because usually, this disease is discovered after it has spread.
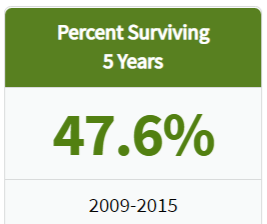
seer.cancer.gov/
This is because there are no screening methods for detection.
If you’re wondering about ultrasound, this tool cannot create an image definitive enough to differentiate between a malignant and a benign mass.
Neither can an MRI or CAT scan. A confirmed diagnosis is made via biopsy (tissue is removed surgically).
Only 19 percent of cases are discovered while the disease is still localized to the ovaries.
These discoveries are made incidentally from imaging tests that the patient receives for other reasons, such as a pregnancy checkup, or X ray of the pelvic area after a car accident.
A “suspicious” mass is detected, and diagnostic follow-up reveals malignancy.
However, such masses aren’t always malignant, either (e.g., benign cysts). Surgery (biopsy) confirms OC diagnosis.
- 68 percent of cases are discovered after the disease has spread to other organs.
- Five-year survival rate for localized disease is 93 percent, and for metastases to distant sites is 29 percent.
Again, if you have appetite suppression, don’t lose sleep thinking it might be ovarian cancer.
Appetite suppression has a myriad of causes, including the fear that you might have ovarian cancer!
You then read up about symptoms and discover that appetite suppression is one of them; suddenly, you can’t eat! Anxiety kills appetite.
 Dr. Yamada specializes in the diagnosis and treatment of gynecologic cancers including ovarian, uterine and cervical. She is also an editorial reviewer for numerous academic medical journals.
Dr. Yamada specializes in the diagnosis and treatment of gynecologic cancers including ovarian, uterine and cervical. She is also an editorial reviewer for numerous academic medical journals.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/piramidonforte
Source: ovarian-cancer.emedtv.com/ovarian-cancer/ovarian-cancer-survival-rate-p2.html
Ovarian Cyst vs. Ovarian Cancer Detection
A Harmless Ovarian Cyst Can Show Up on an Ultrasound and Masquerade as Cancer
Short of surgery, can a doctor tell the difference between an ovarian cyst and cancer?
Some time ago, I had an MRI for a suspected groin injury. I got a phone call and the exact words were: “You have an ovarian cyst.”
It was then recommended I have a follow-up ultrasound to get a better look at the finding. Right away I began wondering about cancer.
The ultrasound showed the “mass” alright, but the gynecologist was not able to determine with 100 percent conviction that this was just a harmless benign development.
He could not rule out ovarian cancer, but he also could not rule out a dermoid cyst, either, which is benign.
Another possibility (the most likely, according to him) was a “follicular cyst,” which was leftover from the menstrual cycle.
I was told to have a follow-up ultrasound in 30 days to track the image, to see if it was getting bigger or smaller. Size changes are suggestive of composition.
Ultrasound cannot definitively diagnose masses in ovaries, and this includes the corpus luteum cyst (different from the follicular), which is the empty “shell” of a follicle from which an egg is released every month.
“The quality of ultrasound interpretation also depends on the experience of the ultrasonographer,” says Diane Yamada, MD, Chief, Gynecologic Oncology, University of Chicago Medical Center.
Due to its unreliability, ultrasound has created many “false positive” results.
This has caused tremendous anxiety and even unnecessary exploratory surgery for patients who turned out to have nothing wrong.
Subsequent ultrasounds in my case revealed that the mass was “growing,” and this had me freaking.
The gynecologist told me that a follicular cyst will start shrinking, and that’s what we were looking for. So why was this thing getting bigger?
The doctor explained that if it was a follicular cyst, it had not yet reached its maximum size, but once it does, it will start shrinking.
He also held onto the possibility that it was dermoid in nature, which is much denser than the follicular.
I should have realized at the time that a tumor doesn’t grow as fast (in terms of millimeter measurements) as this “cyst” was growing. But I wasn’t thinking that way.
All I knew was that they couldn’t rule out ovarian cancer, but that it was most likely an ovarian cyst, and I had to keep having ultrasounds. Finally, the thing started shrinking. And shrinking.
I was cleared and the diagnosis was a follicular cyst. It’s interesting to note that several of these can show up on an ultrasound at the same time, in various stages.
Dr. Yamada specializes in the diagnosis and treatment of gynecologic cancers including ovarian, uterine and cervical. She is also an editorial reviewer for numerous academic medical journals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Pixel-Shot
Sources:
mayoclinic.com/health/ovarian-cysts/DS00129/METHOD=print&DSECTION=all
ovarian-cancer.emedtv.com/ovarian-cancer/ovarian-cancer-survival-rate-p2.html
Why Does Ovarian Cancer Cause Bloating?

Ovarian cancer can cause bloating: not just a feeling of bloating, but a visible abdominal distention.
If you have unexplained bloating sensations or your stomach seems to be growing, even though you haven’t been eating more or are not pregnant, make an appointment with your gynecologist, as this could signal fluid buildup in the abdominal cavity.
Though bloating usually is not caused by ovarian cancer, one of this disease’s hallmark symptoms is bloating.
Ovarian cancer is rare, being diagnosed in about 20,000 U.S. women yearly, with 90 percent of them being over age 50.
However, about 70 percent, according to one study, indeed experience bloating as a symptom of their ovarian cancer.
How does ovarian cancer cause bloating?
“Advanced ovarian cancer, where the cancer has already spread to other organs, can cause bloating because a liquid, called ascites fluid, is produced,” explains Diane Yamada, MD, Chief, Gynecologic Oncology, University of Chicago Medical Center.
“This may result in a few extra liters of fluid in the abdominal cavity, which can make the patient feel bloated or pregnant.
“Presumably, bloating may also be caused by extensive cancer sitting on the surface of the intestines.”
Ovarian cancer is the deadliest of all gynecological malignancies (killing almost 15,000 U.S. women yearly), because there is no known reliable screening tool.
Even ultrasound is not reliable, as some ovarian tumors can appear benign, while a benign mass, such as a dermoid cyst, can be “viewed as worrisome for cancer,” says Dr. Yamada.
In fact, ultrasound can’t even definitively diagnose a corpus luteum cyst, which is the empty “shell” of an ovarian follicle from which an egg is released every month.
“The quality of ultrasound interpretation also depends on the experience of the ultrasonographer.”
Because of its unreliability, ultrasound has caused many “false positive” results, creating unspeakable anxiety and even unnecessary exploratory surgery for women who turned out to have nothing wrong.
Even the CA 125 blood test is unreliable for detecting this stealthy killer, in that a woman with the disease can have a normal CA 125, and one without the illness can have a high CA 125.
If you are experiencing bloating, don’t jump to the conclusion that it must be ovarian cancer.

Freepik.com
There are many medical conditions that cause bloating, including a benign cyst.
However, if after a few weeks, the bloating does not seem to be resolving, do schedule an appointment with your physician.
Ask your gynecologist if your ovaries are okay.
By the time symptoms of OC start appearing, many times the disease has spread beyond the ovaries, drastically reducing survival rates.
When malignancy is found on one ovary only, some women will elect to have both of the walnut-sized organs removed, while other women will choose to retain the healthy ovary so that they can become pregnant.
However, another option exists:
Harvesting eggs from the healthy ovary, and then having the organ removed.
“This should only be considered after extensive discussion with a cancer specialist, however,” says Dr. Yamada.
Ovarian Cancer Risk Factors
- Postmenopausal age
- Obesity
- Infertility
- Inherited gene mutation
- Family history of the disease
- Breast cancer
Symptoms Other than Bloating
- Digestive disturbances
- Pelvic pain
- Pelvic heaviness
- Nausea
- Fatigue
- Unexplained weight loss
- Feeling full after small meals
- Frequent urge to urinate
Dr. Yamada specializes in the diagnosis and treatment of gynecologic cancers including ovarian, uterine and cervical. She is also an editorial reviewer for numerous academic medical journals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ShotPrime Studio
How to Tell if a Doctor Misses a Breast Cancer Diagnosis

How can you ever know if your breast cancer has been missed by your doctor?
There are potential tell-tale signs of a breast cancer misdiagnosis that every woman should know.
It is entirely possible for a physician to be in the process of mistaking a malignant breast lump for a harmless cyst.
The information in this article is from a medical malpractice case litigation transcript that I proofread page for page for its court reporter.
This particular case involved misdiagnosed breast cancer.
By the time it was diagnosed properly, the disease was at stage 3 and a poor prognosis.
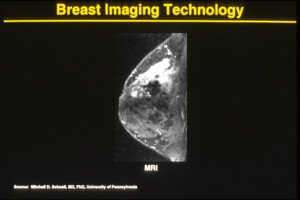
MRI showing a malignant tumor (white area). Cancer.gov
How Breast Cancer Might Be Missed
In this particular case, the plaintiff discovered a lump in her breast. Many women do feel lumps that they believe were never there before.
A mammogram was ordered by the general physician, but the mammogram results were negative.
Women should know that 2D mammograms can miss up to 20% of malignancies.
A needle biopsy of this patient was negative, the mass was drained, and it was assumed to be a cyst.
Several years later the doctor discovered a second lump in the same breast, but not quite in the same location.
For some reason, which was not disclosed in the doctor’s testimony, a mammogram wasn’t ordered.
However, several months later, a mammogram was then ordered. It came back negative.
This time, the doctor did not order a biopsy.
The doctor failed to point out to the radiology center (where the mammogram was performed) that he had felt a mass, yet the mammogram was negative.
He never questioned this conflict. Instead, he literally let it go, and testified that there was no need to follow up because the mammogram had been negative.
The attorney multiple times pointed out that it’s a well-documented fact that mammograms fail to detect 10-15 percent of breast cancers.
Nevertheless, the doctor kept stating that the mammogram was negative, and, to further support the defense, this defendant stated that the radiology center did not offer any recommendations, such as a follow-up ultrasound.
How Things Should Be Done
“Any lump that is felt on exam must be evaluated and explained as either a cyst or a solid,” begins Dr. Kimberly Langdon, MD, OBGYN, medical advisor at Medzino Health, an online doctor and pharmacy site.
“If the mammogram is negative, then an ultrasound will pick up a cyst in general. You can do a fluid aspiration of the breast cyst.
“A lump must be identified as either benign or malignant. It cannot be ignored.”
Testimony was that the physician had believed that the breast lump was probably another cyst, because (once again, here we go) the mammogram was negative, and that he let things go because the radiology lab offered no further recommendations.
Bombshell
The patient’s records indicated that her mother had died from cancer, but the doctor never asked his patient what kind of cancer had killed her mother.
The attorney revealed that it had been breast cancer!
The breast lump seemed to disappear, but then a year and a half later was palpable once more on clinical exam. Another mammogram was ordered. It showed nothing.
Due to miscommunication about this between patient and doctor, the patient was never again seen by this doctor, and shortly after, went to a new radiology center for another mammogram.
This time, the result was positive for breast cancer.
Ultrasound
All of this may be confusing to some women, but it really DOES make a difference when an ultrasound is immediately ordered. Women should push for this, even if a mammogram is negative.
Secondly, she should insist on a 3D mammogram, also known as tomosynthesis. The 3D is more sensitive to picking up suspicious radiographic findings.
Finally, the only way to know what a breast lump really is made of is with a biopsy.
 Dr. Langdon, who is now retired from clinical practice, has delivered over 2,000 babies. Besides obstetrics, she specialized in gynecologic situations such as menstrual disorders, vaginitis, menopause, contraception, pelvic pain and minimally-invasive surgeries.
Dr. Langdon, who is now retired from clinical practice, has delivered over 2,000 babies. Besides obstetrics, she specialized in gynecologic situations such as menstrual disorders, vaginitis, menopause, contraception, pelvic pain and minimally-invasive surgeries.

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}