

Causes & Treatments for Irritable Bowel Back Pain

Irritable bowel syndrome (IBS) can cause back pain.
If you have back pain that has not responded to massage or other typical treatments, you may actually have IBS.
First of all, how does IBS even cause back pain in the first place?
Dr. Pejman Katiraei explains that he had a female patient in her 50s who suffered from back pain, along with other symptoms including chronic fatigue, allergies and migraines.
“Since other treatments were not working, she decided to go on a specialized water fast for three days,” says Dr. Katiraei, DO, FAAP, an integrative physician whose many areas of specialty include adult and pediatric IBS.
“Within two days, her back pain, muscle pain, allergies, and even hot flashes were gone.”
Was there a connection between the absence of food and the disappearance of the pain and other symptoms?
“To understand why this patient got better, we need to understand her IBS was tied to her back pain and all her other symptoms.
“I believe there is now ample evidence to show that people with IBS have inflammation or increased immune activity in their intestines. This inflammation is the reason for pain, diarrhea and most other symptoms.”
Think of the body as a whole unit, such that everything is connected; inflammation in one area of the body can cause a ripple effect: inflammation in another area … including the spinal area.
Eliminate inflammation in the intestines, and you will also eliminate inflammation in the back, says Dr. Katiraei.
How does the gut have anything to do with the back?
Nerves from the intestines go to the spinal cord.
“These nerves are also indirectly connected to the tissue in parts of our back. The inflammation in the intestines also irritates these nerves, which then causes irritation at the level of the tissue (skin) in the connected areas on the back.”
Massage therapists, chiropractors and osteopaths, who heal patients with their hands, can detect tissue change as a response to inflammation.
“So you may go to your chiropractor for back pain, and they may be astute enough to tell you that the pain is not from your back, but rather from your intestines,” says Dr. Katiraei.
This phenomenon also works in reverse. A problem with one’s back can cause intestinal issues.
“There are nerves that go from the spinal cord into the intestines. Some people who have back pain and some intestinal problems actually have some vertebrae that are out of place and impinging on the nerves, causing the nerves not to work perfectly, which then disrupts the signals to the intestines, causing the intestines to not work perfectly.
“The back pain may be due to these bones being out of place. So, sometimes a good adjustment by a chiropractor or osteopath can relieve a person’s back pain and subsequently the abdominal pain.”
Does this all sound confusing?
Dr. Katiraei confirms that this all, indeed, is complicated, and therein lies the problem … the problem a person with IBS has when it comes to finding a treatment that truly works.
“People are looking for a one-size-fits all solution, and it simply does not exist,” says Dr. Katiraei in reference to irritable bowel syndrome.
“When treatments for IBS are tailored to each person, it becomes very possible to effectively treat and perhaps even cure IBS!”

Dr. Katiraei created Wholistic Kids and Families for people interested in learning how to raise a healthy child (and future adult) in a world that’s becoming increasingly polluted with toxins (chemical and emotional).
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Leg Pain Caused by Irritable Bowel Syndrome

Leg pain can have a ton of causes ranging from so very benign to life threatening–and one of those possible causes is irritable bowel syndrome.
Having pain in your leg and wondering if this is related to your irritable bowel syndrome?
Your one burning question is: “Can IBS cause leg pain?”
“Yes! The underpinnings of IBS are fascinating, and this underpinning helps explain the leg pain,” says Pejman Katiraei, DO, FAAP, an integrative physician whose many areas of specialty include adult and pediatric IBS.
“To start, we must recognize that people with IBS have inflammation in their intestines. Inflammation means that there is increased immune activity in a part of the body.”
An example of this would be the redness that occurs around a cut in your skin, or the swelling of a sprained ankle.
“People with IBS have inflammation in their intestines,” continues Dr. Katiraei.
“This inflammation typically involves a specific type of immune cell called mast cells.”
A doctor may give an endoscopy to a person with IBS, but tell that patient that all is normal … because pathologists are not able to see the mast cells via standard biopsy analysis.
The problem is there, says Dr. Katiraei, but it goes unseen. This is why people with IBS are often told that nothing is wrong.
But Dr. Katiraei continues, “If doctors used very sensitive tools like electron microscopes or very specialized immune stains, they will find these changes in the intestines.
“In the bowel, sitting right next to these mast cells are nerve cells that take information from the intestines to the spinal cord.”
During an inflammatory process, the mast cells release chemicals that can irritate nerve cells.
“The irritated nerve cells then send signals to the spinal cord that there is something very wrong,” says Dr. Katiraei.
“Our brain interprets this signal as pain. It so happens that the nerves from the legs merge in the spinal cord in the same area as the intestines. The signal from the gut and the legs gets mixed up.”
This is called viscerosomatic convergence and it tricks the brain.
“The pain signal from the intestines gets mixed up as a pain signal from the legs.”
So indeed, a person with IBS can definitely experience a perception of pain in the legs. The leg pain here is actually from the intestines.
Dr. Katiraei adds, “When the inflammation in the intestines calms down, so does the inflammation in the joints, and the pain disappears.”
Dr. Katiraei created Wholistic Kids and Families for people interested in learning how to raise a healthy child (and future adult) in a world that’s becoming increasingly polluted with toxins (chemical and emotional).
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Does Colon Cancer Always Cause Abdominal Pain?

Colon cancer can cause abdominal pain, but does it always?
When I say “pain,” I don’t mean cramps.
There’s a difference between abdominal pain and abdominal cramps. Abdominal pain can result from colon cancer.
But have you wondered, however, if in every case of colon cancer that’s gone untreated long enough to produce symptoms, if abdominal pain is always one of the resulting symptoms?
“Remember, for polyps and early cancers, the hallmark symptom is the absence of symptoms — this is why getting screened at age recommendations while asymptomatic is so important,” explains gastroenterologist Whitney Jones, MD, a national expert and frequent speaker on early-age onset colon cancer prevention, and Founder, Colon Cancer Prevention Project.
A person can “feel fine” yet have colon cancer.
A colonoscopy can detect this disease early, long before it invades surrounding tissue and causes symptoms (such as abdominal pain).

Freepik.com
Dr. Jones explains, “Abdominal pain is one of the many hallmark symptoms and presents usually when there is advanced disease including obstruction, perforation or spread into adjacent organs.
“It can be the initial presenting symptom of large polyps or early cancers.”
Because symptoms of numerous benign conditions can mimic those of colon cancer, it’s important to get colonoscopy screenings beginning at age 45 if you are of average risk for this disease.
To determine if you’re at average risk or increased risk, you need to consult with a physician.
A key risk factor for this disease is having a parent or sibling who had/has the condition.
Pain in the belly is one of the most common ailments of the human body.
Thus, if you’ve been experiencing abdominal pain lately, don’t jangle your nerves by jumping to the conclusion that this must mean colon cancer, even if you are over age 45.
It’s more likely to be from any number of benign conditions.
However, does the abdominal pain from colon cancer feel different from stomach discomfort caused by benign conditions?
Dr. Jones says, “Not really. This is why any unexplained abdominal symptoms should be fully evaluated and if unresolved, colonoscopy should be a consideration once evaluated by a health care professional.
“Symptoms overlap greatly between all of the different GI problems and this includes colon cancer.
“Only a thorough exam can tell the difference and thank goodness, most of the times the cause will not be colon cancer.”
There are literally reams of causes of abdominal pain not related to colon cancer.
However, some non-malignant causes of stomach pain are of a very serious nature, such as appendicitis, a ruptured spleen and a ruptured ovarian cyst — all of which are life-threatening if not promptly treated.
In addition to abdominal pain, Dr. Jones adds the following for colon cancer symptoms:
“Change in bowel habits, rectal bleeding or blood on the tissue (paper), change in stool caliber, fatigue either from anemia or from advanced colon cancer, weight loss, nausea/vomiting from obstructions, anemia, jaundice from metastatic colon cancer to the liver or the bile duct.”
 Dr. Jones’practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Dr. Jones’practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/George Rudy

Can Diarrhea Be the Only Symptom of Colon Cancer?

Is it possible for diarrhea to be the only symptom of colon cancer?
You may be familiar with colon cancer’s classic signs such as abdominal pain, weakness, weight loss, blood in stools and ribbon-like stools — and diarrhea and/or constipation.
I wondered, however, if colon cancer can cause just the symptom of diarrhea.
I posed this question to gastroenterologist Whitney Jones, MD, a national expert and frequent speaker on early-age onset colon cancer prevention, and Founder, Colon Cancer Prevention Project.
Dr. Jones says: “Yes, diarrhea alone can be a symptom, particularly if this is a new and persistent change in habits.
“Tumors in the lower colon or rectum cause a partial obstruction of the bowel, which compensates by liquefying the stool to get stool past any narrowed portion.”
The tricky thing about this is that diarrhea is a symptom of tons of medical conditions, most of them benign.
This symptom is so common that you can’t watch prime time TV without seeing a diarrhea commercial.
Millions of people have suffered a sudden onset or gradual onset of diarrhea without knowing the cause, at least initially.
I then asked Dr. Jones if there’s a bowel obstruction, can we assume that once the obstruction starts creating enough blockage to cause diarrhea, that there will be “no going back” to formed stools?
Or can the tumor sometimes shift position and thus result in normal stools?
He responds, “The process, like irritable bowel syndrome, can wax and wane in the short-run (i.e., 1-2 weeks), but in general does not just stop and reverse to normal.
“It will usually be unremitting and eventually leads to obstruction if not diagnosed sooner.”
When having even a routine colonoscopy, if you’ve been enduring diarrhea lately, make sure your physician knows about this.
This way, the endoscopist can collect tissue samples of your colon for microscopic analysis to see if an inflammatory condition is responsible for your symptoms.
For example, ongoing diarrhea for no apparent reason can be caused by microscopic colitis.
Dr. Jones explains, “The time to be screened for colon cancer is while you are asymptomatic. Otherwise, it is not a screening test; it is a diagnostic test.
“When you do have a GI problem (as we all will ), if you had been screened, you are much less likely to have the cause of your issue be colon cancer.”
- Blood in the stools — could be red, reddish brown or even black with a tarry look
- Pencil-thin or ribbon stools
- Feeling of incomplete voiding after a bowel movement
- Constipation or diarrhea
- Alternating constipation with diarrhea
- Odd change in bowel habits
- Abdominal pain or cramps, gas
- Feeling of bloating or fullness
- Unexplained weight loss or fatigue
- Back pain
Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/daizuoxin

IBS vs. Microscopic Colitis: Similarities, Diagnosis

IBS (irritable bowel syndrome) and microscopic colitis produce symptoms that are similar enough to result in misdiagnosis.
So do you have IBS (irritable bowel syndrome) or microscopic colitis?
After all, the symptoms overlap. Furthermore, symptoms of microscopic colitis can vary greatly from patient to patient.
I should know; I had a bout with microscopic colitis, yet compared to the symptom descriptions of people posting on a microscopic colitis forum, my symptoms were quite mild.
“Microscopic colitis generates diarrhea which is for the most part continuous,” says Matthew M. Eves, MD, F.A.C.G., a gastroenterologist in Alabama.
“It is not necessarily associated with abdominal pain. Irritable bowel syndrome by the Rome criteria is defined as abdominal pain associated with a change in bowel habits.
“The diarrhea with IBS does not have the volume microscopic colitis does.
“Unfortunately, many physicians do not adhere to the strict definitions of irritable bowel syndrome and because of that, microscopic colitis has a tendency to be misdiagnosed as IBS.”
Microscopic colitis is more likely to be misdiagnosed as irritable bowel syndrome, than the other way around, and this mix-up is actually rare.
Microscopic colitis can only be properly diagnosed (and definitively at that) with random large-colon tissue biopsies via colonoscopy, which are then examined under a microscope.
“There are, however, several primary care physicians who will listen to the clinical symptoms and diagnose IBS based on that,” says Dr. Eves.
“Because many physicians see IBS as a diagnosis of exclusion, if the workup is not complete, the door is left open for missing microscopic colitis.”
Rome criteria are used to definitively diagnose irritable bowel syndrome.
“Basically you have to have a change in bowel pattern associated with abdominal pain.
“Some would argue that a diagnosis of IBS could be made if these criteria are rigidly applied.
“This is done to establish IBS as a more legitimate diagnosis even though there is no test to confirm its presence.”
Dr. Eves continues: “IBS that meets the Rome criteria is but a small part of a larger spectrum of disorders.
“So by using the criteria you would improve diagnostic accuracy of the single entity of IBS, but miss other disorders of the enteric nervous system commonly called functional disorders.”
Dr. Eves adds that most non-GI physicians view irritable bowel syndrome and functional disorders as one and the same.
And from a practical point, they are indeed synonymous, says Dr. Eves.
“The patient has abdominal pain and usually some bowel symptoms or bloating and wants relief.
“Whether it meets the definition of IBS or not, I still treat with antispasmodics, cathartics, anti-diarrhea agents and antidepressants primarily.
“I keep changing the mix until I get the patient to a point where the impact of the symptoms is minimized.
“It is frustrating because I’m not fixing the problem. In fact, we don’t even really know what the problem is.”
If this sounds like a mess to sift through, it is. To avoid it, the patient must have a colonoscopy to test for microscopic colitis.
The treatment for microscopic colitis differs from treatment for irritable bowel syndrome.
“If a patient presents with diarrhea for more than four weeks, they ought to have a colonoscopy.
“There is no getting around it. Ulcerative colitis and Crohn’s disease could be missed as well.
“Unfortunately, the physician must recognize the possibility of microscopic colitis.
“If he does not he will lump them in with IBS patients. That is why chronic diarrhea, which is a complex illness, ought to be worked up by a gastroenterologist. Unlike acute diarrhea, it will not go away on its own.”
 With more than 20 years of diverse experience, Dr. Eves cooperates with other doctors and physicians in medical groups including Imc-Gulf Coast Gastroenterology PC.
With more than 20 years of diverse experience, Dr. Eves cooperates with other doctors and physicians in medical groups including Imc-Gulf Coast Gastroenterology PC.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, nikitabuida
Source: perskyfarms.com/phpBB2/index.php
Brain Tumor Headache: What Are False Alarm Symptoms?
Does your very bad headache have you fearing you have a brain tumor? Does the pain make you think it could only be from a brain tumor?
Though the only way to rule out a tumor is with a scan of your brain, this doesn’t mean that a really bad headache is most likely cancer.
There are a number of causes for a really severe headache other than cancer or a ruptured aneurysm.
Sinus headaches have been known to trigger significant head pain.
Anyone with migraine disorder knows that this can bring on a searing headache.
But there’s yet another condition that can cause a really intense headache — plus additional symptoms that can make the sufferer become terrified that it’s a brain tumor.
The condition is called intracranial hypotension syndrome.
Intracranial Hyptension Syndrome
“Intracranial hypotension results from a cerebral spinal fluid (CSF) leak,” says Sumeer Sathi, MD, a neurosurgeon with NYU Langone Health, who treats brain tumors.
“This leak causes a decreased amount of CSF that bathes the brain and spinal cord.
“CSF leaks can be from a leak in the spinal canal (i.e., spinal tap), defects in the spinal tube, and ventricular shunt malfunctions.
“Intracranial hypotension can cause a syndrome that presents in a variety of symptoms.
“The most typical symptom is called a positional headache; the headache tends to worsen in an upright position and improves while lying flat.
“Other symptoms can include nausea, vomiting, vertigo, tinnitus, fatigue and neck pain.
“Onset of symptoms can be abrupt or gradual depending on the cause.”
Digging Deaper into IHS
A study was published in Neurology in which 11 people with incapacitating headaches were found to have enlarged pituitary glands (the gland is in the brain).
Their headache symptoms were those of intracranial hypotension syndrome.
However, intracranial hypotension, at least in the study subjects, had a variety of etiologies, such as unexplained fluid loss, spontaneous occurrence, cervical spine surgery and lumbar puncture via spinal tap.
The headaches were accompanied by nausea, neck pain, visual and hearing problems, and even facial numbness.
As you can see, IHS produces symptoms that very much mimic those of a brain tumor.
Enlarged Pituitary Gland
The researchers believe that the sinuses, that surround the gland, accommodate the low fluid pressure.
They do this by becoming engorged…with blood. This doesn’t make the diagnosis easy.
However, the study results could prevent some people from getting mistakenly thought to have a brain tumor, when they really have intracranial hypotension syndrome.
According to MRI exams, the pituitary glands were 50 percent larger, on average, than normal.
IHS Treatment
“Treatment is aimed at correcting the defect/hole in the dura mater that holds the CSF,” says Dr. Sathi.
When surgery is not required to repair the leak, treatments may consist of bed rest, hydration and corticosteroids.
 Dr. Sathi’s expertise includes spine surgery and treating brain tumors including metastasis, gliomas, meningiomas and acoustic neuromas using gamma knife radiosurgery.
Dr. Sathi’s expertise includes spine surgery and treating brain tumors including metastasis, gliomas, meningiomas and acoustic neuromas using gamma knife radiosurgery.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2000/12/001226082416.htm

Twitching Tongue: Bulbar ALS or Normal?

If your twitching tongue is driving you mad with anxiety and fear of bulbar onset ALS, then you need to know how to rule out bulbar onset ALS, which is diagnosed in only about 600 people every year in the U.S.
However, for some panicky individuals, this number is no reassurance if their tongue is twitching, and especially if they’ve been perceiving accompanying symptoms such as a heavy-feeling tongue, or a lopsided tongue.
Other Perceived Symptoms
Others that can cause alarm over bulbar onset ALS in some hyper-alert individuals include difficulty swallowing, and the inability to rapidly speak a particular selection of words without mispronouncing one.
Fear can play abominable tricks on the vulnerable mind.
People with bulbar onset fear are very capable of spending huge amounts of time every day examining their tongue in a mirror for all sorts of nuances, ranging from comparing one side to the other, to counting the number of indents in the tongue.
Other tongue tests for bulbar that can consume a fearful person’s time include rapidly moving the tongue from side to side; pressing it as hard as possible to the roof of the mouth or to the side; sticking it out to see if it twitches; rapid chewing; and chewing tough foods.
No matter how many tests such an individual subjects himself to, there’s never enough reassurance that they do not have bulbar onset ALS.
But is this endless menagerie of testing necessary?
“If a person is really worried about having bulbar onset ALS, inspecting the tongue is not the exam to perform,” says Kristina Lafaye, MD, a board certified neurologist specializing in clinical neurophysiology and neuromuscular medicine with Tulane Doctors Neurosciences.
“If they do not have any problems with swallowing, chewing, or controlling their secretions, then they do not need to bother looking at their tongues.”
Nevertheless, visual inspections of the tongue is a common, time-sinking occurrence amongst individuals suffering from bulbar onset hypochondria.
Dr. Lafaye emphasizes, “Looking at the tongue is irrelevant.”
She adds, “Bulbar onset is marked by problems swallowing, chewing, and controlling secretions.
“There is coughing and a perception of food (liquids) ‘going down the wrong way.'”
As for swallowing, chewing and controlling secretions, keep in mind that if you fixate on these elements, you’ll be prone to imagining or perceiving difficulties with these.
The more you focus on every tiny detail of your eating experience, the more you’ll imagine something’s wrong.
The time to review your chewing, swallowing and secretion control is when you weren’t thinking about it.
Look back and ask yourself how things went during that dinner with friends when you actually didn’t think about bulbar onset ALS or your tongue. Went pretty smoothly, didn’t it?
Dr. Lafaye says about the bulbar onset progression, “This is subtle and does not occur overnight.
People with ALS have a very distinct speech which is impossible to describe, but it is a combination of spasticity and weakness.
“These individuals need swallowing studies and other diagnostic studies.
“They must have electrodiagnostic studies to assess for denervation in other parts of their body, because they do not have ALS if symptoms are limited to the bulbar muscles.”

Dr. Lafaye is triple board certified: neurology, clinical neurophysiology and neuromuscular medicine from the American Board of Psychiatry and Neurology. Her expertise and leadership continue to make a significant impact on patient outcomes.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/oneinchpunch
Twitching Tongue: When to Worry About ALS
Is your twitching tongue keeping you up all night worrying you might have bulbar onset ALS?
Relax, relax. Don’t let a twitching tongue ruin your life.
Do you realize how exceedingly rare bulbar onset ALS is?
Even if your tongue is twitching all over the place, don’t forget that your tongue is a muscle.
Muscles twitch. That is a fact of nature.
Only about 600 people annually are diagnosed with bulbar onset ALS.
So the odds of your twitching tongue being a symptom of bulbar onset are over 60 times LESS than dying in a car accident!
Thus, examining your twitching tongue for every little distinction, every little groove, indent and twitching, in the name of “could this be bulbar onset ALS?” will prove nothing, really.
And don’t stick your tongue out to inspect for twitching, because the mere act of sticking out the tongue can cause this muscle to twitch!
And forget the side comparisons for size and shape.
“The tongue is a muscle, so like any other muscle one side could be a little larger,” says Kristina Lafaye, MD, a board certified neurologist specializing in clinical neurophysiology and neuromuscular medicine with Tulane Doctors Neurosciences.
Yes, one side could be bigger. Just like one calf or one foot or one bicep can be bigger than the other.
Focus on what your tongue can do, not what it looks like or whether or not it twitches.
Dr. Lafaye explains, “Basically, if the tongue moves normally as characterized by the person speaking, eating, swallowing, and breathing normally, then those are the important points.”
You need to learn how to distinguish between perceived difficulties chewing, swallowing and talking, and actual (or clinical) difficulties performing these functions.
Bulbar onset prevents carrying out these functions without true, actual difficulty.
The “rule of tongue” is this …
If you must concentrate and really focus your mind upon what you are testing for, then there’s no need to think bulbar onset ALS.
On the other hand, if you have bulbar onset ALS, you will not have to scrutinize and hunt for any noticeable problems, because they will be quite obvious.
Deliberately selecting tough-to-chew-and-swallow foods won’t prove anything.
Dr. Lafaye also says, “There can be atrophy of the tongue caused by other conditions (e.g., tumors compressing the hypoglossal nerve), but there would be other signs and symptoms as well.”
And that’s key: other signs and symptoms, and REAL signs and symptoms, not ones that you have to invent through carefully calculated examinations in order to keep your fear alive.
Dr. Lafaye is triple board certified: neurology, clinical neurophysiology and neuromuscular medicine from the American Board of Psychiatry and Neurology. Her expertise and leadership continue to make a significant impact on patient outcomes.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Twitching Calf Muscle: Should You Worry?

Have you been closely monitoring the twitching in your calf muscle?
Counting the number of “fasciculations” per minute, watching the muscle move as it twitches, and even going as far as repeatedly testing out the strength of your calf muscle?
If you’ve succumbed to this fright and obsession, it can only mean that not too long ago, you noticed an annoying twitch going on in your calf muscle.
You Googled muscle twitching calf…
…or something similar, and that’s when you learned that muscle twitching is one of several symptoms associated with an incurable, fatal disease called ALS.
And since then, you’ve become consumed with terror that your twitching calf muscle means ALS, never mind that muscle twitches in the calf rarely mean anything sinister.
Worrying over calf twitches may very well stem from:
- Frequency of the fasciculations
- How easily they’re felt
- Whether or not they’re visible to the naked eye.
Another reason a person ends up overwhelmed with worry about a twitching calf muscle is that he or she mistakenly has made a connection between quantity of ALS search results with likelihood of having this disease.
But a swarm of ALS links on the first few pages of Google’s search results, after typing into the search engine, Should I worry about a twitching calf muscle, absolutely does NOT mean that lower body fasciculations are likely a symptom of ALS!
The search results reflect who’s writing what, NOT how likely you might have a disease.
Otherwise, you may as well believe in the Loch Ness Monster, because if you type in these keywords, a bunch of links about the Loch Ness Monster will show up!
Your twitching calf muscle is by far most likely caused by:
1) fatigue
2) anxiety over relationships, money, job, etc.
3) caffeine intake
4) exercise
5) improper footwear
6) body position when seated
7) insufficient fluid intake
8) mineral imbalance such as insufficient calcium and magnesium
9) medication
10) massage
More serious conditions such as Lyme disease can cause the symptom, but again, this is rare.
Summary
“It’s common,” says Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“Most often it’s due to a ‘misfire’ of a nerve that causes a muscle to twitch,” adds Dr. Besser.
“It’s the same process that causes hiccups.
“If there is loss of ability to use the limb or weakness or loss of sensation, further evaluation is needed.”
Otherwise, a mere twitch should not mean a serious underlying disease.
24/7 Calf Muscle Twitch?
Even if fasciculations occur “all the time,” DO NOT WORRY as long as nothing else is wrong such as that same leg seems to be dragging as you go up stairs or walk across a room.
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/ANN PATCHANAN

Carpal Tunnel Syndrome Symptoms vs. Impinged Neck Nerve

Did you know that the symptoms of an impinged neck nerve can masquerade as carpal tunnel syndrome?
A doctor might get fooled by this. This happened to my mother.
The doctor who misdiagnosed my mother’s carpal tunnel syndrome for nerve entrapment or impingement in the neck, was an ER doctor whose work badge said “toxicology” on it.
The doctor asked my mother to describe her symptoms, then touched her in various places along the hand and arm, asking what she felt, if she felt it, etc.
The doctor felt around her neck and discovered an extra sensitive spot.
My mother told him she had difficulty turning her head leftward.
After gathering information from her as far as numbness, tingling, pain, etc., the doctor said he suspected a pinched or impinged nerve in the neck.
However, only an MRI would supposedly confirm that, so he ordered an MRI.
A few hours later the doctor returned with the MRI report and said, “It was what I suspected; you have nerve impingement in the neck.”
Interestingly, the doctor said he himself had the same problem.
The doctor appeared to be around 40 and explained he, too, had neck nerve impingement, and described his symptoms, which were identical to my mother’s, but not as extensive as hers, which were as follows:
1) Awakening in middle of the night with arm pain
2) Experiencing numbness in the second and third fingers, and
3) Shoulder pain.
My mother’s symptoms were more pronounced, but the doctor’s symptoms could “fit” inside my mother’s easily.
So when he said she had neck nerve impingement, we didn’t question this diagnosis, even though we were well aware of the idea of carpal tunnel syndrome.
I might add that my mother’s carpal tunnel syndrome was in both hands simultaneously.
The doctor said that a neck nerve impingement could explain why her symptoms were in both hands/arms.
The MRI report revealed narrowing of the spinal canal through which the spinal cord extends; a few bulging disks; degeneration due to age; and some arthritis.
The doctor said the next step was to make an appointment with a neurosurgeon and take it from there.
He said this didn’t necessarily mean she needed surgery; other treatment options were possible, and he himself had seen a neurosurgeon three times and had never been “cut into.”
My mother got an appointment for the following week, but in the meantime, was able to get a sooner appointment with a neurologist to have an EMG test done.
The EMG neurologist immediately suspected pronator teres syndrome after examining her.
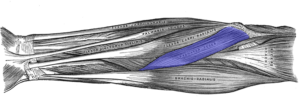
The pronator teres muscle joins the upper arm bone with the two forearm bones.
His secondary diagnosis was carpal tunnel, and he said that her symptoms were not consistent with those of neck nerve impingement!
He said the EMG test would be the only way to tell for sure if the problem was pronator teres syndrome or carpal tunnel syndrome.
Next day was the EMG test: “It’s carpal tunnel,” said the neurologist early into the testing.

The nerves affected by CTS. Source: scientificanimations.com/CreativeCommons
Not only did the EMG test confirm carpal tunnel syndrome, but the EMG test ruled out any pinched nerve in the neck, since the neurologist attached recording electrodes to my mother’s neck.
“Carpal tunnel syndrome and an impinged nerve in the neck can have similar symptoms, which can make it difficult to distinguish between the two conditions,” says Christopher R. Sforzo, MD, head surgeon and founder, Sforzo Dillingham Stewart Orthopedics + Sports Medicine.
“However, one key difference between the two conditions is the location of the symptoms.
“Carpal tunnel syndrome affects the hand and wrist, while an impinged nerve in the neck may affect the neck, shoulders, arms and hands.
“Additionally, carpal tunnel syndrome symptoms are usually more pronounced in the thumb, index and middle fingers, while an impinged nerve in the neck may affect a broader area of the arm.
“A healthcare professional can perform a physical exam, nerve conduction studies and imaging tests to help diagnose the underlying cause of symptoms and develop an appropriate treatment plan.”
If you’re having troubling symptoms (numbness, tingling, weakness, pain) in your fingers, hands, arms and even shoulder, and you’re diagnosed with nerve impingement or pinching at the neck WITHOUT an EMG test to confirm this, you should have an EMG test done.
An EMG exam may reveal that you have carpal tunnel syndrome or even pronator teres syndrome.
And here my mother was … thinking that she might need neck surgery!
 Christopher R. Sforzo, MD,
Christopher R. Sforzo, MD,

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}