

Confusion, Cognitive Impairment from Dilaudid

If someone is on Dilaudid at the hospital, and not long after shows confusion or cognitive impairment, it may very well be the drug talking, which is an opioid narcotic painkiller.
Every single time my mother has ever been given Dilaudid in the ER or hospital room, cognitive changes resulted.
When this first happened, I wasn’t sure if it was the Dilaudid or if something was truly wrong with my mother’s thinking.
It’s scary, to witness mental changes in a family member, especially when the nurse never tells you, “By the way, if you notice any cognitive changes or mental confusion, it’s probably the Dilaudid.”
But after witnessing the confusion and disorientation and irrational thinking in my mother a few times, it began getting predictable: “I’ve seen this before,” I’d comment.
Dilaudid’s Affect on Mental Status
For this article, I asked a physician if Dilaudid, a commonly dispensed painkiller in emergency rooms and hospitals, could cause cognitive impairment (temporary, of course).
“Dilaudid is a very powerful narcotic and can certainly cause confusion and altered mental status, often within 30 to 60 minutes of taking it,” says Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”

He continues, “As with any narcotic, changes in mental status would be normal, but often decrease over time as the body adapts to them.”
My first observation of Dilaudid with my mother was after her knee arthroscopy.
I convinced myself that the irrational thinking and confusion had to have been related to “something they gave her.”
Soon after was double carpal tunnel surgery, and once again, she was on Dilaudid and talking confused, thinking irrationally.
“It has to be the Dilaudid,” I reflected, though also concerned that the confusion might be psychiatrically based. The effects wore off after she returned home.
A year later she was back on Dilaudid … after coronary bypass surgery, and holy smokes, she was in La-La Land.
And maybe lingering effects of anesthesia was involved, but my mother showed numerous signs of altered mentation, such as telling the nurses that I was a doctor (I was a personal trainer).
At first my mother justified this because I was using medical jargon when I spoke to the nurses and doctors.
Then my mother began refuting my claims that I was not a doctor.
Turns out my mother thought that I was her other daughter, who is a doctor.
When my mother came home, she thought she was still in the hospital and thought that I was a nurse.
This was scary stuff, because I also speculated that the heart-lung machine might have caused permanent cognitive impairment.
But during the hospital stay, my mother was given Dilaudid. The confusion dissipated after she was home.
A few days later she was back in the ER with grueling abdominal pain and given Dilaudid, and once again, she began thinking irrationally … until the drug cleared from her system.
Some weeks later my mother was in the hospital for a chronic subdural hematoma suffered after falling and hitting her head, and was given Dilaudid after the brain surgery to drain the hematoma. Once again, she was loopy.
Of course, I couldn’t help think that maybe this time, the loopiness and irrational talking was the result of brain damage from the surgery. It disappeared when she was taken off the Dilaudid.
Not long after, she was in for a second brain surgery; the hematoma had recurred.
This time she was very irrational and disoriented … more so than before, but I kept thinking it’s just the Dilaudid, and made a comment about that to the nurse.
The nurse told me that my mother had not been on any Dilaudid at all, but she was on Seroquel due to agitation the previous night.
So I blamed the cognitive impairment on Seroquel. The cognitive impairment didn’t wear off, like it always historically had done. I was really worried.
I began thinking the neurosurgeon “nicked her brain,” or that “something happened during the surgery” that injured my mother’s brain.
Fast-forward: My mother fully recovered, and after researching chronic subdural hematoma, I have concluded that the deteriorated cognitive status resulted from her brain re-expanding to fill the space that the hematoma had taken up.
The neurosurgeon blamed the impaired mental functioning on a combination of anesthesia, surgery and painkillers.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Effexor Withdrawal How to Minimize Discontinuation Syndrome

A doctor explains how to best get off Effexor to minimize discontinuation syndrome side effects and withdrawal.
Effexor can be difficult to get off of, due to discontinuation syndrome. Ask the many people who have decided to stop taking Effexor (or other SSRI’s), only to experience troubling withdrawal symptoms.
Effexor is prescribed for clinical depression, but getting off it doesn’t have to be difficult.
First of all, if you want to get off Effexor but haven’t made any changes in that direction yet, first consult with your prescribing physician.
Never quit Effexor before discussing this with you doctor.
So, is there a way to make Effexor withdrawal easy, or, at least, not so troublesome?
What are the common withdrawal effects when quitting Effexor?
“The longer you’ve been on the medication and the higher the dose, the more likely one is to get the discontinuation syndrome,” says Dr. David Gutman, Assistant Clinical Professor in the Department of Psychiatry at Columbia University, and Director of Psychopharmacology, ColumbiaDoctors Eastside.
Dr. Gutman continues, “It can include agitation, loss of appetite, anxiety, diarrhea, dizziness, dry mouth, low mood, fatigue, flu-like symptoms, headaches, insomnia, nausea and sensory disturbances (including shock-like electrical sensations), among other symptoms. Most common is a flu-like feeling.”
Why does quitting Effexor cause these side effects?
“It is related to rapidly stopping the serotonin reuptake inhibition,” says Dr. Gutman.
“Medications with longer half lives (they take longer for your body to digest) or that work on other neurotransmitter systems are less likely to cause this condition.”
Can a person just outright quit Effexor?
“A physician should be consulted prior to making medication changes.
“They can help a person decide how quickly to reduce the medication depending on the total clinical situation.”
What is the best way a person can get off Effexor?
Dr. Gutman says, “Reducing the medication slowly is the best way to avoid or minimize the discontinuation syndrome.
“Switching to an SSRI with a longer half life and then tapering that medication is another option.
“Effexor, like other antidepressants and other classes of drugs, should be tapered off of with the guidance of the prescribing physician, to minimize discontinuation syndrome (side effects).
“Clinical or ‘major’ depression in its truest form is incapacitating and can leave people essentially bedridden.
“If depression becomes disabling and a person has difficulty functioning, medication can be very helpful.”
 Dr. Gutmanis interested in the intersection between neurobiology and psychology; his general practice consists of psychiatry, psychopharmacology and psychotherapy.
Dr. Gutmanis interested in the intersection between neurobiology and psychology; his general practice consists of psychiatry, psychopharmacology and psychotherapy.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Has My Child Been Misdiagnosed with ADHD?

If your child’s been diagnosed with ADHD, consider a misdiagnosis; so many other conditions can masquerade as attention deficit hyperactivity disorder.
“I would say that many of the kids I see come in with that diagnosis,” says Claudia B. Rutherford, PhD, a Massachusetts-based licensed psychologist specializing in the psychological and neuropsychological testing of children and adults.
Dr. Rutherford says that the diagnosis of ADHD in her patients “turns out to be incorrect” many times, “and I know that many clinicians feel it is over-diagnosed.”
ADHD Misdiagnoses
Sleep disorders. About 25 to 30 percent of children diagnosed with ADHD actually have untreated obstructive sleep apnea, explains Steven Y. Park, MD, otolaryngologist, author of Sleep, Interrupted: A Physician Reveals The #1 Reason Why So Many Of Us Are Sick And Tired.
Have your ADHD-diagnosed child or teen undergo sleep apnea testing, since this condition can replicate ADHD symptoms such as poor ability to focus on school work or pay attention in class, restlessness and being easily distracted.
Posttraumatic stress disorder. Emotional trauma from a recent crisis event can cause symptoms that mimic ADHD.
Hearing impairment. If your child doesn’t pay attention to you or to teachers, maybe it’s because they’re not hearing adequately.
Numbed hearing can result from a chronic exposure to loud sounds such as screaming and shrieking children/toddlers, wearing earbuds loud with music, being around blaring entertainment systems, motors or machines, or having a history of multiple ear infections.
Mood disorders. Feeling the blues is normal in life, but undue or relentless depression can impair one’s attentiveness.
If you suspect depression, then a medical workup is in order, since this may be caused by a medical situation such as an underactive thyroid.
At the opposite end, bipolar disorder’s “manic” phase can result in hyperactive behavior.
Generalized anxiety disorder. Could your child or teen be unsettled about things going on in their life? New school? Parents’ pending divorce? Problems with a coach or teacher?
Kids can have ongoing anxiety from stressful environments or from getting too much criticism or pressure to be perfect in a sport from a parent.
Learning disabilities. This does NOT mean a low I.Q. or that of being “slow.”
The so-called learning disability is an impairment of information processing that can affect speech, reading, listening and learning math.
Auditory processing deficits. Dr. Rutherford says, “Kids with central auditory processing disorders have trouble performing well in the classroom.”
They do better with one-on-one teaching.
“They can display symptoms that can easily mimic the inattentive type of ADHD,” says Dr. Rutherford, “such as having difficulty following directions in a series, showing comprehension problems during conversations, or poorly discriminating between similar sounding words.”
Speech-language delays. “I see numerous kids with a question of ADHD and turn out to have undiagnosed receptive speech-language delays,” continues Dr. Rutherford.
“These are kids who may have had chronic ear infections or were slow in mastering language acquisition.
“They are behind in the ability to understand spoken language; if this is not diagnosed, it is easy to assume the child is simply not paying attention.”
TBI (traumatic brain injury). Has there been any recent trauma to the head during sports or play? Even if it was months ago?
Autism spectrum disorder. ASD and ADHD share come traits, such as the ability to hyperfocus, repetitive movements (often called fidgeting or stimming) and sensory sensitivities.
However, a child can have both of these conditions, but with only the ADHD being identified during the assessment.
So though there are cases where the child eventually is given an autism diagnosis instead of the ADHD diagnosis, there are also cases in which the individual gets an ASD diagnosis added to their ADHD status. This is now commonly called AuDHD.
Only a psychologist or neuropsychologist with a specialty in evaluating the pediatric population for ADHD should conduct an ADHD assessment.
If a pediatrician or social worker has said to you, “Your child has ADHD,” this really means your child has been exhibiting a minimal number of symptoms that may fit criteria for an ADHD diagnosis.
But you should still seek a formal assessment from a psychologist or neuropsychologist with this specific experience.

Claudia B. Rutherford
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Freepik
Child Has Nightmares about Drowning, Choking: Cause, Solutions
Does your child suffer night terrors about drowning, suffocating or choking?
There may be a very definitive cause for your child’s night terrors of suffocation and drowning, and it will surprise you.
It may very well be sleep apnea. Yes, sleep apnea. Sleep apnea can occur in children, even thin kids.
Kids with sleep apnea are sometimes misdiagnosed as having ADHD, says Dr. Frank Barnhill, MD, board certified family physician practicing child and adult preventative care/ADHD-behavior medicine in upstate South Carolina.
Dr. Barnhill hence sees quite a few children who actually have sleep apnea … which causes breathing problems, including stopped breathing, during sleep, which can lead to night terrors about suffocating or drowning.
Dreams About Drowning Mean a Real-Life Airway Obstruction
Dr. Barnhill explains that night terrors centering around choking, drowning or suffocation are “caused by the child struggling for breath as his or her obstruction to airflow increases and oxygen levels drop.”
Children often describe the sensation as being choked, drowning or suffocating.
Experts think they link the actual event to something they have either seen or read or been told about (television, movies, books, word of mouth stories), as a memory, and it creates a night terror nightmare.”
Dr. Barnhill says that the typical scenario is that the child begins falling asleep.
If the child has obstructive sleep apnea, he or she will start snoring.
If it’s central sleep apnea, the child won’t snore but will develop “sighing breaths.”
As the condition progresses, the respiratory rate will get interrupted by irregular partial breaths called hypopneas, or breathing cessation (apneas).
Both types of breathing disturbances may cause either partial arousal from slumber, or complete awakening, “as the brain tries to alert the rest of the body to falling oxygen levels,” says Dr. Barnhill.
“This explains why some kids awake struggling to get a deep breath, while others are just partially awake and don’t remember it.
“The latter kids often complain of nightmares or night terrors about drowning or suffocating.”
This is easy to understand, the concept of having a dream or nightmare related to a physical problem that’s happening to you in real life.
How many times have you dreamt you were insanely thirsty and couldn’t get enough water in your dream, only to awaken thoroughly parched?
Night terrors about suffocating or drowning have other causes besides sleep apnea.
Dr. Barnhill explains, “Anything that interferes with the child’s normal sleep can cause them — gastroesophageal reflux and restless leg syndrome, for example.”
If your child has the following symptoms, don’t chalk it up to him or her being a pest; instead, consider a real, physical cause of these symptoms: bedwetting, sleepwalking, complaints of things happening to their legs like “bugs biting,” and sudden emotional problems.
The brains of sleeping children are adept at manufacturing a story about what’s really happening to their bodies, and hence, night terrors about drowning, choking or suffocating in kids with sleep apnea and other problems that affect their body.
 In practice for 30+ years, Dr. Barnhill is the author of “Mistaken for ADHD.” He has additional training in Infant, child and adolescent medicine, urgent and emergent medicine, and gerontology. Selfgrowth.com/experts/frank_barnhill
In practice for 30+ years, Dr. Barnhill is the author of “Mistaken for ADHD.” He has additional training in Infant, child and adolescent medicine, urgent and emergent medicine, and gerontology. Selfgrowth.com/experts/frank_barnhill
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can You Have Celiac Disease without Symptoms?

You can have celiac disease and not even know it; that’s because half of people with this autoimmune disorder don’t have any symptoms.
So how do they learn they have it?
Usually it’s because they get tested because an immediate family member–who has symptoms–is diagnosed with it.
The Commonality of Celiac Disease
Celiac disease is more common than most people think, and most don’t have symptoms, says Stefano Guandalini, MD, Founder and Medical Director, The University of Chicago Celiac Disease Center.
The condition is more common than many doctors believe, which is why it takes an average of nine years for this autoimmune disorder to finally be diagnosed in an ailing patient.
Can you have active celiac disease yet no symptoms?
Dr. Guandalini explains, “Yes, in fact, the majority of people with celiac disease have no symptoms at all.” So what brings these individuals to the diagnostics stage if they don’t have symptoms?
Perhaps a first-degree relative has CD and they decided to get tested.
Another way a person, without symptoms, can discover he has celiac disease is if he learns he has the gene/s for the disorder, and decides to get a blood test for CD – which turns up positive for tissue transglutaminase antibodies. The positive blood test then leads to a small-intestine biopsy.
Dr. Guandalini continues, “Even though they have no symptoms, when the disease is active it is doing the same harm internally.
“Ultimately, research has shown that celiac disease left untreated … with or without symptoms … can not only lead to serious complications, but it most definitely leads to a shorter life span.”
The University of Chicago Celiac Disease Center states: There are more than 200 signs and symptoms of celiac disease, yet a significant percentage of people with celiac disease have no symptoms at all.
It continues:
The undamaged part of their small intestine is able to absorb enough nutrients to prevent symptoms.
However, people without symptoms are still at risk for some of the complications of celiac disease.
“To help diagnose celiac disease, physicians first test blood to measure levels of certain antibodies,” explains Dr. Guandalini.
“These antibodies are: the anti-tissue transglutaminase (tTG); the anti-endomysium (EMA); and the anti-deamidated gliadin peptides (DGP).”
He continues:
“A positive antibody test suggests that a person might be celiac, but it is not a conclusive test; a biopsy will be needed to confirm the diagnosis.
“The blood test is, in other words, a quite accurate” first step. If the test is positive, your doctor should know what steps to take next.
Symptoms of celiac disease (remember, not all patients have even ONE of these)…
- Diarrhea
- Constipation
- Bloating
- Gas
- Abdominal pain
- Vomiting
- Weight loss without trying
- Grayish foul-smelling stools
- Fatigue
- Anemia
- Tingling or numbness in the legs
- Tooth discoloration
- Pale sores inside the mouth
- Unexplained infertility and miscarriages
- Brittle bones
- Skin rashes
- Brain fog
- Depression
The disorder, left untreated, raises the risk of bowel cancer, and can cause neurological problems. Treatment is eliminating gluten 100 percent, for life.
Kids and even babies can develop celiac disease.
For children and babies, it can manifest itself by stunting their growth.
The most common symptom of celiac disease in adults is iron deficiency (anemia) that does not respond to therapy.
 Dr. Guandalini is an internationally recognized expert on celiac disease, Professor Emeritus, University of Chicago, and the founder of the University of Chicago Celiac Disease Center. His clinical and research efforts have greatly influenced how celiac disease is diagnosed and treated today.
Dr. Guandalini is an internationally recognized expert on celiac disease, Professor Emeritus, University of Chicago, and the founder of the University of Chicago Celiac Disease Center. His clinical and research efforts have greatly influenced how celiac disease is diagnosed and treated today.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: celiacdisease.net/assets/documents/CDCFactSheet_Symptoms_2010.pdf

Is a Torn Rotator Cuff Always Painful?

If you had a torn rotator cuff, would you necessarily be in enough pain to suspect this?
Or might the pain–even severe–come and go, faking you out?
According to Edmond Cleeman, MD, the pain of a torn rotator cuff can actually come and go, surprisingly.
I’m a former personal trainer and wondered about whether or not pain, from a torn rotator cuff, could take breaks every so often, providing no-pain days for the patient.
“They certainly can have good days,” says Dr. Cleeman, a board certified orthopedic surgeon who specializes in sports medicine and arthroscopic surgery of the shoulder, knee and hip.
This surprised me, because when a rotator cuff is torn, the tendon (usually some of it, rather than all of it) is disconnected from the bone it’s supposed to be attached to; it’s torn away.
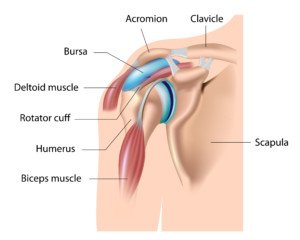
Shutterstock/Alila Medical Media
How could this sometimes be painless?
I can understand this if the patient is still. But “good days” mean that the patient is using the shoulder and arm, and feeling no pain at all, despite the torn rotator cuff.
“To make things more confusing, there are many older patients walking around with rotator cuff tendon tears and don’t even know it,” says Dr. Cleeman, founding member of TRIARQ, a community of orthopedists and physical therapists.
“There are MRI and ultrasound imaging studies that have found that a certain percentage of people have rotator cuff tears without symptoms.
“These studies took groups of people with no shoulder pain and no history of trauma and found that as people age (particularly over 60), a percentage had tears.
“Some studies followed these patients and found that a percentage eventually became symptomatic.”
Tears in the rotator cuff are not always caused by a single-event trauma, such as during a heavy weight lift at the gym, in which the person suddenly feels intense pain arise in the shoulder.
Nor do rotator cuff tears necessarily result over a short time period, in which an athlete repeatedly performs the activity that initiated a small tear, such as throwing or a particular weight-lifting routine.
Many tears happen over time in older people, a part of aging, particularly in people who are not physically fit. The tendons degenerate over time, and a tear results.
A comprehensive strength-training program, especially when initiated during young adulthood, will go a tremendous way in helping prevent tendon degeneration down the road.

Freepik.com
However, even an intense strength training program is no guarantee against an acute injury of the rotator cuff.
For example, the strongest guy in the gym one day plays beach volleyball.
He leaps for the ball and dives into the sand for it, his arm outstretched before him, palm down, as he slides into the sand.
This is a very potential recipe for a shoulder tendon injury.
Thinking he should work through the pain that continues to persist several days later, he decides to do some bench pressing, further injuring the shoulder tendons.
He doesn’t go to a doctor and continues trying to lift weights, and eventually suffers a rotator cuff tear.
 Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
Dr. Cleeman is a highly experienced orthopedic surgeon and sports medicine specialist at Manhattan Orthopedics. He is committed to performing advanced minimally invasive procedures, allowing his patients to go home the same day.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Can Running Cause Hip Bursitis (Trochanteric)?

Dr. Bright explains, “Trochanteric bursitis is very common among runners. In order to understand trochanteric bursitis, it is important to have an understanding of what a bursa is.”
If you suffer bursitis hip pain from running, here are some excellent exercise treatments that are recommended by a sports medicine doctor.
“Trochanteric bursitis is very common among runners,” says Darrin Bright, MD, who specializes in sports medicine and family medicine with OhioHealth Physician Group.
“In order to understand trochanteric bursitis, it is important to have an understanding of what a bursa is.
“A bursa represents a fluid filled sack that allows structures to glide smoothly over other structures. Bursitis occurs when the bursa becomes inflamed from repetitive movement or excessive pressure.”
Right off the bat, you see how running or jogging can easily be a cause of hip bursitis, what with all of the repetitive movement going on in the hip joint.
Dr. Bright continues, “In this case, the greater trochanteric bursa lies on top of the hip bone, allowing the iliotibial band to glide smoothly over the hip bone.
“Running results in repetitive movement of the IT band over the bursa, which may result in greater trochanteric bursitis.
“Similarly, if the IT band is tight it will exert excessive pressure on the bursa, resulting in greater trochanteric bursitis.”
What kind of exercises are therapeutic for bursitis of the hip caused by running?
Dr. Bright says, “Physical therapy (PT) is an integral part of the recovering from greater trochanteric bursitis.
“PT is directed at stretching the iliotibial band as well as strengthening the gluteus medius and other hip external rotators.”
Here are a few exercises for strengthening the gluteus medius and gluteus minimus, which are responsible for external hip rotation (the major “butt muscle,” the gluteus maximus, enables hip extension).
#1. The hip abduction machine at your gym. This isolates the hip rotator muscles.
#2. Get on all fours. Keeping one knee on the floor, lift the other leg (think of how a male dog lifts one leg to relieve itself) so that the inner thigh is parallel with floor, but lower leg bent so that there is a 90 degree angle at the knee. Thighs are perpendicular to each other. Then lower.
Do repetitions this way. You should feel the outside of your hip and upper thigh working. This exercise will fatigue the hip rotators quickly. Switch sides.
#3. Inline skating, especially up hills, will target the hip rotators. (If this aggravates hip bursitis pain, then don’t do it.)
#4. Stand with feet shoulder width apart. Lift one leg into a high-march position, but don’t extend lower leg.
Now rotate upper leg to the side so that the knee is to your side, maintaining the high-march position, then return to starting high-march position.
Repeat for reps, keeping knee high. This will tire you quickly if you’re not used to doing isolation work for hip rotators. Switch legs.
If someone has hip trochanteric bursitis, how long should they avoid running?
Dr. Bright explains, “Recommendations regarding running with greater trochanteric bursitis will vary depending on the degree of injury.
“I usually recommend using pain as your guide. If the pain is affecting your gait or you are limping, then you should not run.
“Otherwise if you aren’t limping try some easy running and see how it goes. Avoid hills and up-tempo or faster running.
“Icing after activity and again at bedtime can help with the inflammation in the bursa.”
Don’t let your hip bursitis make you lose hope with your running program.
 Dr. Bright gives special focus to comprehensive care for runners, triathletes and cyclists, overuse injuries, stress fractures and active release technique (ART).
Dr. Bright gives special focus to comprehensive care for runners, triathletes and cyclists, overuse injuries, stress fractures and active release technique (ART).
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: ©Lorra Garrick

Lamictal Rash Side Effect: Causes and Prevention

The Lamictal rash, a side effect of this drug, is well-known in the community of Lamictal users.
And this rash isn’t pretty at all.
Is there a way to prevent this side effect?
And what causes the Lamictal rash in the first place?
In fact, the Lamictal rash can be much more than nasty; the website for this prescription drug states:
LAMICTAL may cause a serious skin rash that may cause you to be hospitalized or to stop LAMICTAL; it may rarely cause death.
For this article I asked Dr. Oanh Lauring, MD, founder of Lauring Dermatology in Nottingham, MD, how it is that this serious skin rash can develop from taking Lamictal. She explained:
“The mechanism is unknown and approx 20 percent of patients can develop some type of a rash, but it is rarely life threatening. It usually presents as hives, itching or red blotchy patches all over the body.”
In other words, if you develop the Lamictal rash, there is no need to fear for your life. The drug’s Website further explains:
There is no way to tell if a mild rash will develop into a more serious reaction. These serious skin reactions are more likely to happen when you begin taking LAMICTAL, within the first 2-8 weeks of treatment.
But it can happen in people who have taken LAMICTAL for any period of time. Children between 2 to 16 years of age have a higher chance of getting this serious skin reaction while taking LAMICTAL.
Is there a way to prevent the Lamictal rash?
Dr. Lauring says no. She explains, “Other more well-known anti-epileptics such as phenytoin, phenobarbital, primodone are more likely causes of life threatening rashes like Steven-Johnsons syndrome (patients have sloughing and bleeding of their mucosa such as the mouth, gut and groin), or toxic epidermal necrolysis (patients can slough off their entire skin within hours to a few days).
“These rashes represent an autoimmune hypersensitivity response that is purely genetic-based and therefore you cannot prevent it.
“If any family members are allergic to a specific class of medications, then they should use these meds with caution.
“If someone has a clear-cut severe itchy rash to a drug (and I have excluded infection), I may treat them with oral antihistamines and topical or oral steroids depending on the severity.”
According to the Website, your risk of getting a rash from using Lamictal increases, if you are also taking Depakene or Depakote (anti-seizure drugs).
Another factor that increases risk of this situation is if you take a higher starting dose than what your physician has prescribed for you.
Finally, a third variable that raises the risk of this skin rash is if your dose of the drug is increased at a faster rate than what has been prescribed.
 Dr. Lauring is former chief of dermatology at Mercy Medical Center. Lauring Dermatology provides medical and cosmetic services including for skin cancer, acne, psoriasis, hair and nail problems, and skin rejuvenation.
Dr. Lauring is former chief of dermatology at Mercy Medical Center. Lauring Dermatology provides medical and cosmetic services including for skin cancer, acne, psoriasis, hair and nail problems, and skin rejuvenation.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

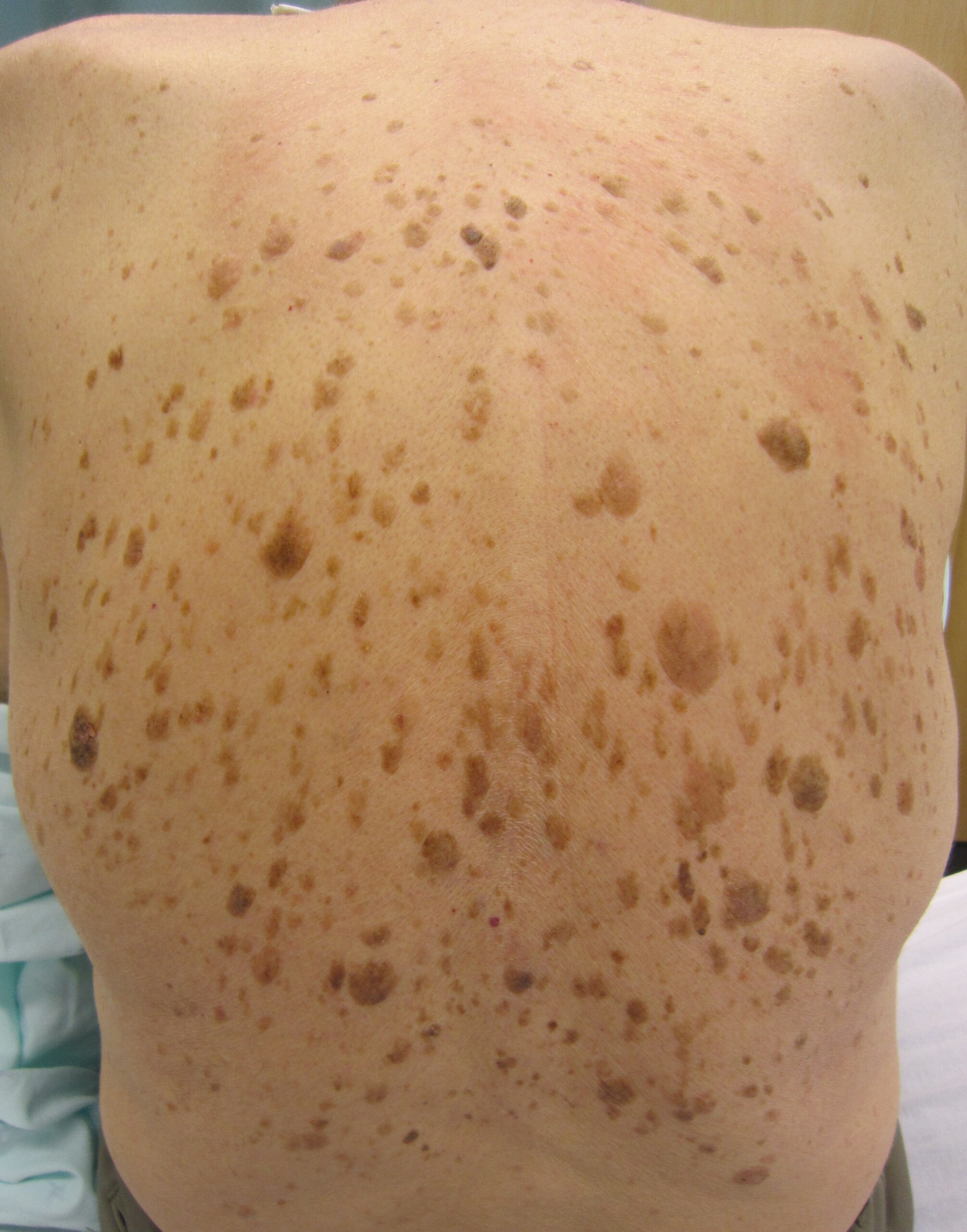
Can Seborrheic Keratosis Turn into Skin Cancer?

Seborrheic keratoses can look like melanoma, the deadly skin cancer.
These benign lesions can come in a variety of colors, sizes and shapes, and can raise concern if you just happen to discover one or a few on your skin.
Seborrheic keratoses can easily be identified by a dermatologist and have several classic features.
One such feature of seborrheic keratoses is that it can resemble skin cancer, including melanoma.
There are two questions to consider.
1 Can skin cancer or melanoma arise from the cells of a seborrheic keratosis?
2 Is a seborrheic keratosis more likely to develop into melanoma when compared to regular areas of skin?
“Seborrheic keratoses represent a normal thickening of the skin,” says Adam J. Mamelak, MD, a board certified dermatologist and founder of Sanova Dermatology in Austin, TX.
They can appear to be stuck onto the skin in the way that a little speck of dirt or clay can be stuck on. But not all appear that way.
They may resemble warts, but a seborrheic keratosis does not contain the virus that causes warts, the human papilloma virus.
A seborrheic keratosis that develops or progresses can begin to look like a wart, with a lot of unsightly texture.
On the other hand, some can appear like glossy tiny droplets, which can be flesh colored, pinkish or some shade of brown, with a smooth surface.
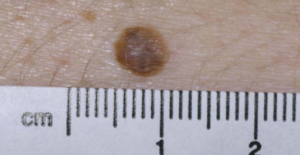
Seborrheic keratosis
These lesions may, or may not, itch. You may never know you have them unless you just happen to visually discover them upon, for example, adjusting your bra strap in the mirror, and you see a few speckles on your skin that you didn’t notice before.
They can appear just about anywhere and usually begin appearing after age 40.
“Their development is most often genetic,” says Dr. Mamelak. “If your parents have them, there’s a good chance you’ll get them as well.
“Often called age or liver spots, seborrheic keratoses are completely benign.” In short, their cells are not atypical.
But we need to dig deeper here. The cells that make up a seborrheic keratosis are perfectly normal — but can they ever become cancerous?
Dr. Mamelak explains, “The skin cells that make up a seborrheic keratosis can become malignant, just as they can in normal skin.
“That is, a skin cancer can arise within a seborrheic keratosis the same way it can arise in normal-appearing skin.”
This shouldn’t be surprising, because these benign skin barnacles are MADE UP OF SKIN.
As for their likelihood of turning cancerous when compared to surrounding skin, Dr. Mamelak says, “The risks for a skin cancer arising anywhere are the same: history of excessive sun exposure and sunburns, fair skin and complexion, personal and/or family history of a skin cancer.”
If one of these skin growths is scratched, it can bleed. Do not take this to mean a sign of melanoma or other cancer.
“And while some consider them unsightly, or they can catch or rub on clothing and become painful and irritated, there is no reason to treat them unless they become symptomatic,” says Dr. Mamelak.
“Just as you should be mindful of a non-healing or changing lesion on your skin, if a seborrheic keratosis starts to change in appearance, bleeds or changes color, it should be evaluated.”
Otherwise … you may as well just leave them be, unless the itching gets annoying; they interfere with clothes; or they become a cosmetic issue. They can be removed via liquid nitrogen by freezing.
A scar may result from the new skin, growing in after the removal, having different pigment concentrations than the original skin.
If you are not sure you have a seborrheic keratosis, and keep wondering if it might be melanoma or some other kind of skin cancer, make an appointment with a dermatologist. The peace of mind will be worth it.
 Dr. Mamelakfocuses on the full breadth of dermatologic care, from cosmetic skin solutions to advanced skin cancer removal. He’s founder of the Austin Mohs Surgery Center, which is dedicated to the treatment and management of skin cancer.
Dr. Mamelakfocuses on the full breadth of dermatologic care, from cosmetic skin solutions to advanced skin cancer removal. He’s founder of the Austin Mohs Surgery Center, which is dedicated to the treatment and management of skin cancer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: James Heilman, MD, CreativeCommons

When an Itching Mole Begins Bothering You

Here’s what a dermatologist says about itching moles.
If you’re concerned about an itching mole (could it be melanoma?), first make sure that the itching is coming from the actual spot itself, rather than nearby skin.
Sometimes it’s difficult to tell precisely where the itching is coming from.
With that said, assume that you have an itching mole. According to dermatologist Alan Rockoff, MD, a suddenly-itching mole probably means trauma to the little spot – rather than cancer or melanoma.
A woman complaining of an itching mole wrote in to medhelp.org.
She says there is a tiny darker spot on an otherwise symmetrical, brown mole, and the mole had been there “forever.”
However, it is located beneath where her bra strap normally lies.
A few days before she wrote in, the spot began feeling weird.
When she touched it, it became sensitive, as though being poked with a little needle.
She wanted to know if it was possible to have an itching mole that was not melanoma or another form of cancer.
Dr. Rockoff, with the Rockoff Dermatology Center in Brookline, MA, explains, ”When a mole starts to bother you suddenly, that invariably means not cancer, but minor trauma.
“I’m sure that when you see the doctor, the dark spot — if it’s even still there — will be diagnosed as a small scab from the mole’s rubbing on your bra.
“The needle sensation is also almost certain to be from the rubbing.
“Just keep the mole covered so it doesn’t run, and don’t freak out — just see the doctor for reassurance and you’ll be fine!”
The patient described her problem in fine detail. But had she simply said, “I have an itching mole,” and said nothing more, this likely would have altered Dr. Rockoff’s response – because melanoma can indeed cause a mole to itch.
The patient is being smart by planning on seeing a doctor. And that’s exactly what you should do if a spot on your skin becomes worrisome.
Some people are mole hypochondriacs and create needless anxiety.
On the other hand, around 8,000 U.S. people die every year from melanoma.
Many would still be alive if they, too, were hypochondriacs – or, to put it another way, hyper-vigilant about skin surveillance for suspicious changes.
Melanoma is a ruthless cancer once it spreads. However, it is one of the most curable forms of cancer when caught early.
With vigilant surveillance, the layperson can catch melanoma early.

Melanoma. Shutterstock/Krzysztof Winnik

Melanoma. CreativeCommons/Hans677

Melanoma. Cancer.gov
To help catch melanoma early, it’s important to conduct monthly skin checks.
If you have moles in difficult to inspect areas such as your back, you can have a dermatologist inspect them every six months; this will provide you peace of mind and extra surveillance.
Just because your insurance won’t cover elective screening like this doesn’t mean you shouldn’t invest in it.
If you keep scratching a mole, it is likely to continue itching, just like any other area of the skin that you keep scratching, since repeated scratching produces histamines that cause even more itching.
 Dr. Rockoff
Dr. Rockoff 

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}