
Choking Sensation in Throat: Causes, Solutions

An ear, nose and throat doctor explains the causes of a choking sensation in the throat, and what you should do.
Have you been experiencing a choking feeling or sensation in your throat?
“The most common cause of a choking sensation, without a known foreign body incident, is acid reflux, ‘silent reflux’ with our indigestion or heartburn symptoms,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
“Acid from the stomach comes up and irritates the back of the throat,” adds Dr. Silvers. This causes it to swell.
“This makes it hard to swallow and gives a feeling of a lump in the throat.
“Patients may describe shortness of breath, a choking sensation or trouble swallowing.
“Stress is a big contributing factor to acid reflux. Stress will increase the production of stomach acid and the acid can reflux up.”
Have you noticed that the choking sensation or feeling in your throat tends to subside or even disappear during times that you’re relaxed or absorbed in concentration? This is a tip-off that it’s stress-related.
Signs the Choking Sensation in Your Throat Is Serious
You may have a serious condition that warrants medical attention if the choking sensation in your throat occurs only when you’re trying to swallow food.
This is especially concerning if over a short period of time, the ability to clear food from your throat becomes increasingly difficult, such that you’ve begun switching to more soft foods in your diet.
Another worrisome sign is if the choking feeling comes with new symptoms that seem to be related.
Examples are trouble with speech, a buildup of saliva, a cough that won’t go away, and pain in an ear.
Tests that a doctor will order include an upper endoscopy, a barium swallow, a chest X-ray, pulmonary function and allergy testing.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Brain Aneurysm: Surviving a Rupture with Fast Treatment
Often, a ruptured brain aneurysm means quick death, and if not, permanent brain damage. But these burst blood vessels do not always have to be lethal.
Surviving a Ruptured Brain Aneurysm
“The sooner the presence of an aneurysm is detected, the more likely it is to be successfully treated,” says Dr. Ezriel Kornel, a neurosurgeon with Somers Orthopaedic Surgery & Sports Medicine Group in NY.
“With a ‘full’ rupture, symptoms range from sudden death to coma to impaired level of consciousness, impaired speech and impaired motor function to simply an excruciating headache that does not let up,” continues Dr. Kornel.
What is the ruptured aneurysm (hemorrhagic stroke) headache like?
Dr. Kornel explains, “Always, it starts with a ‘thunderclap’ headache. About 50 percent of individuals with a full rupture of a cerebral aneurysm die before reaching a hospital, especially in more remote areas.
“A favorable outcome is certainly more likely if the aneurysm is discovered before there is a rupture that results in neurologic deficits.
“Over 60 percent of aneurysms are now treated by coiling, a procedure by which a very fine catheter is introduced into the aneurysm via arteries from the groin, into the head, and tiny ‘coils’ are injected into the aneurysm, filling it and causing it to clot off rather than bleed.
“Those aneurysms that cannot be coiled require clipping of the aneurysm microsurgically via a craniotomy.”
 Ezriel Kornel, MD, FACS, is at the forefront of minimally invasive neurosurgery which he uses to treat brain tumors and other neurological ailments. Known for his pioneering contributions to minimally invastive surgery techniques, he has developed and patented several innovative instrumentation methods that substantially reduce surgical trauma and enhance recovery times.
Ezriel Kornel, MD, FACS, is at the forefront of minimally invasive neurosurgery which he uses to treat brain tumors and other neurological ailments. Known for his pioneering contributions to minimally invastive surgery techniques, he has developed and patented several innovative instrumentation methods that substantially reduce surgical trauma and enhance recovery times.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image credit: Vecteezy.com
How Long Can Brain Aneurysm Leak or Bleed Before Bursting?
Could a brain aneurysm slowly leak or bleed for a few weeks before rupturing?
To find out if a brain aneurysm could slowly bleed or leak over a period of up to three weeks before finally rupturing, I interviewed Dr. Ezriel Kornel, a neurosurgeon with Somers Orthopaedic Surgery & Sports Medicine Group in NY.
Devastating Misdiagnosis
I was inspired to write this article after proofreading a medical malpractice deposition transcript, in which the plaintiff’s persistent headache was diagnosed by a doctor as a sinus issue, when in actuality, it was related to an aneurysm in her brain.
More than two weeks later she had a seizure, and it turned out that she had suffered a ruptured brain aneurysm.
She survived but with a permanent disability related to her eyes plus dizziness.
Had the brain aneurysm been slowly leaking or bleeding all this time?
“Aneurysms don’t ‘slowly’ leak,” says Dr. Kornel. “What is referred to as a sentinel bleed is an initial very small rupture of an aneurysm that immediately seals itself.
“The sudden expansion of an aneurysm without bleeding may also cause a headache.
“In any case, the initial symptom is a sudden, substantial headache that may linger for hours or days but is not unbearably profound.
“The initial headache is often described as the worst headache of their life.
“The neck may feel achy and stiff as well and light may be bothersome. There may be nausea as well.
“However, speech and mentation are preserved as is movement of the face and limbs.”
The plaintiff also experienced ptosis—a drooping upper eyelid. It never dawned on her to insist upon an MRI of her head, even when she began developing visual problems.
Dr. Kornel explains, “An expanding aneurysm of the posterior communicating artery can cause pressure on the third nerve which impairs the nerve’s function.
“This results in dilatation of the pupil which can result in blurry vision and ptosis or drooping of the eyelid.
“Also, eye movements are limited in the affected eye, so the individual can develop diplopia or double vision.
“All these symptoms with exception of third nerve compression can last for days or weeks and may never be followed by a ‘full’ rupture of the aneurysm.
“However, often, when we see a patient with a ‘full’ or substantial rupture of a cerebral aneurysm, if they give us a history of a prior headache, it is generally a few days to a week or two earlier.”
A brain aneurysm is also known as a hemorrhagic stroke. There are different ways to treat this potentially life threatening condition.
Ezriel Kornel, MD, FACS, is at the forefront of minimally invasive neurosurgery which he uses to treat brain tumors and other neurological ailments. Known for his pioneering contributions to minimally invastive surgery techniques, he has developed and patented several innovative instrumentation methods that substantially reduce surgical trauma and enhance recovery times.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image credit: Vecteezy.com
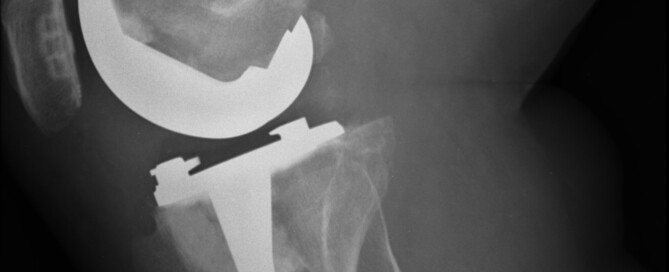
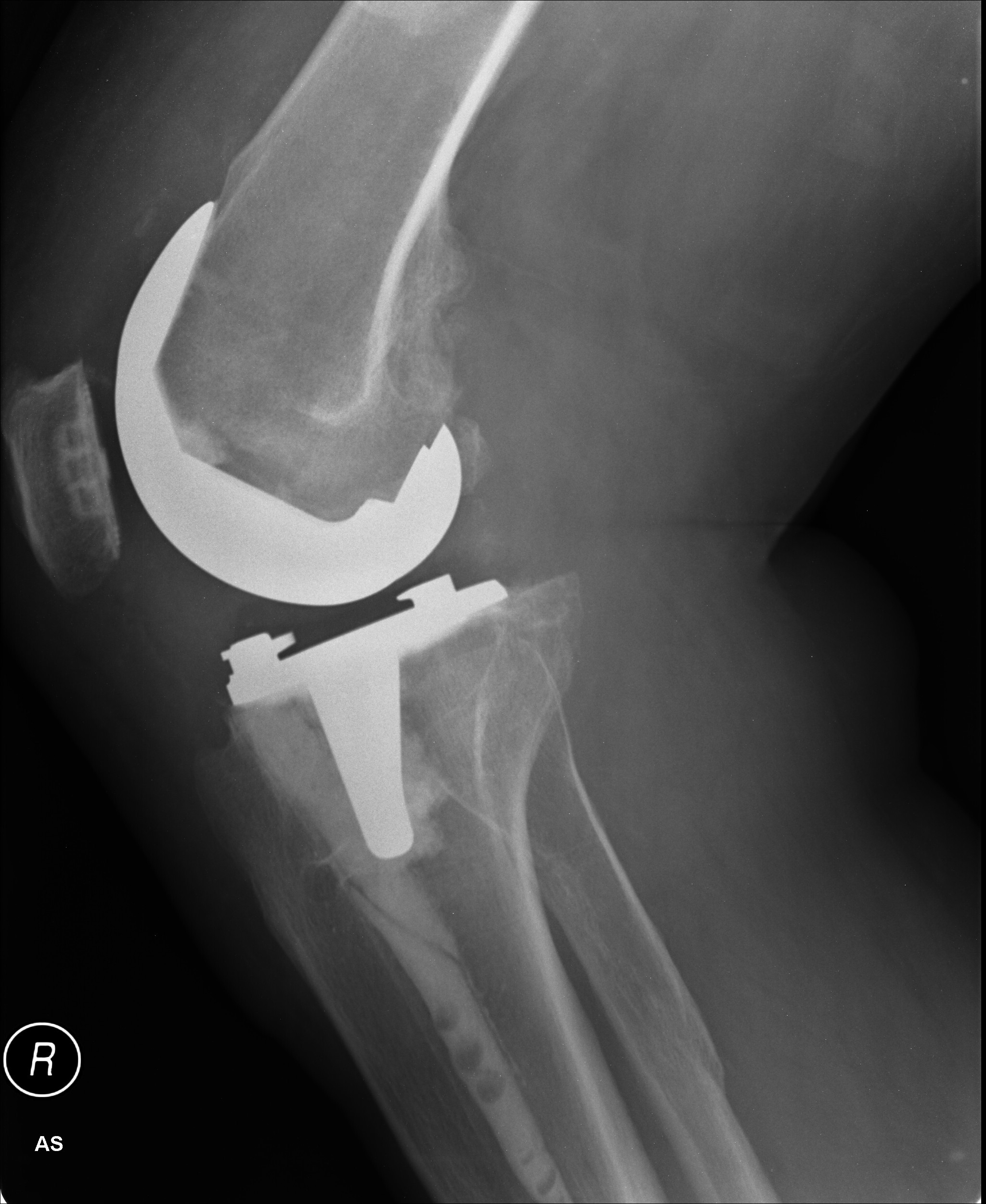
Are You At Risk for a Failed Knee Replacement Joint?

Despite how common total knee replacement is, many patients end up with failed or loosened hardware that causes pain and crashes their hopes of regaining mobility.
Approximately 50,000 people in the U.S. are diagnosed with a failed total knee replacement each year.
Revision surgeries are often required to address the malfunctioning hardware.
Risk Factors for a Failed TKR
“Oftentimes, we don’t know why they loosen,” says Jeffrey A. Geller, MD, Associate Chief, Division of Hip & Knee Reconstruction; Director, Minimally Invasive Hip & Knee Replacements, Columbia University Medical Center, NY, NY.
“It is assumed that some combination of prolonged time since surgery, and active lifestyle, leads to a process where the cement de-bonds from the bone.
“Rarely, prosthetic design may be inferior, leading to earlier loosening, but most popular designs have done well with good medium to long-term results reported in the scientific literature.”
A failed knee replacement can also result from infection or misalignment.
Symptoms of a Loosened Knee Replacement
Pain and swelling in the affected joint
Pain upon sitting and standing
Pain while walking
A sensation of warmth or heat at the knee
A feeling of instability when standing or walking
The symptoms may not occur for a while following the surgery, and thus, the patient may not make the connection, and instead blame the pain on other factors such as nerve compression in the back, which can actually cause pain in the knees.
Nerve compression in the back, particularly in the lumbar (low back) region, can certainly cause knee pain.
This occurs when nerves exiting the spine become pinched or irritated, often due to conditions like herniated discs or spinal stenosis.
The compressed nerves can radiate pain down the leg, sometimes manifesting as knee pain despite the issue originating in the back.
This referred pain is a result of the complex nerve pathways and how they interact with different parts of the body.
Since the replacement surgery may initially be successful, it can take quite some time before the patient realizes the possibility that perhaps the knee replacement has become loose or in some way is not working properly.
The pain can radiate beyond the knee and up the thigh, mimicking iliotibial band syndrome, as well as mimicking the pain in the upper legs that can result from spinal stenosis (narrowing of the spinal canal).
 Dr. Geller specializes in arthritic disorders of the hip and knee. He has extensive training in joint replacements and performs surgery using some of the latest, most advanced minimally invasive techniques.
Dr. Geller specializes in arthritic disorders of the hip and knee. He has extensive training in joint replacements and performs surgery using some of the latest, most advanced minimally invasive techniques.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can a Loose Knee Replacement Be Fixed Conservatively?

If you have a failed or loosened knee replacement, wouldn’t it be fantastic if this could be fixed without surgery — a conservative treatment that can resolve this problem?
To go through another invasive surgery, in which the failed parts are removed and a whole new artificial joint is put in its place, is just too daunting to even think about for many patients.
Knee replacement revision surgery involves replacing some or all of the prosthesis, and this doesn’t paint a pretty picture for patients who face once again going under the knife and having general anesthesia for the three hour operation.
And then there’s another several months of rehabilitation to go through all over again.
Bad News for Those with a Failed Knee Replacement
“If a patient with a loosening knee replacement absolutely cannot have surgery due to multiple medical problems, the only thing that may provide some modest degree of relief will be some type of brace and activity modification, i.e., limited walking,” says Jeffrey A. Geller, MD, Associate Chief, Division of Hip & Knee Reconstruction; Director, Minimally Invasive Hip & Knee Replacements, Columbia University Medical Center, NY, NY.
Dr. Geller explains that the brace requires a prescription. “It is usually fitted and dispensed by a brace specialist, called an orthotist.”
The brace, of course, will not repair a loosened knee replacement hardware. It may only take the edge off of the pain.
What about pain pills?
Pain medications can be limited in their ability to obstruct the pain, as well as be troublesome if the patient experiences unpleasant side effects. Dr. Geller adds that nerve or pain blocks are temporary and not effective.
About 20,000 or so knee replacement revisions are performed in the U.S. every year.
And some end up loosened or failed — and sometimes the reason is not clear why.
Unfortunately there is no way other than surgical to fix this, and the revision surgery may result in yet another failed replacement.
Dr. Geller specializes in arthritic disorders of the hip and knee. He has extensive training in joint replacements and performs surgery using some of the latest, most advanced minimally invasive techniques.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, peoplecreations
Can a Single Fasting Glucose Over 100 Mean Prediabetes?
Did you get one fasting glucose reading over 100 and under 126 and are now panicking that diabetes will soon be a part of your life?
“One individual reading of a fasting glucose over 100, does not impart a diagnosis of prediabetes,” says Richard Kelley, MD, a practicing physician in Texas for 20+ years, and author of “The Fitness Response,” “The Three-Hour Appetite” and the ebook, “The Fitness Response ‘Diet’ for Women.”
Dr. Kelley continues, “However, it is generally felt that two or more fasting glucose tests which fall above 100 and below 126 on two different days, would be reasonable to assess as prediabetes.”
Research in the field of how sleep impacts glucose metabolism is relatively young, but the research results are solid, including the report in a 2010 Journal of Clinical Endocrinology & Metabolism that just one night of sleep deprivation can cause insulin resistance, a type of prediabetes that’s a forerunner of type II diabetes.
If your fasting glucose is over 100 and under 126, don’t panic. Evaluate your sleeping habits.

Has your sleep been disrupted lately due to anxiety?
Chronic stress can also cause a higher than normal fasting glucose result.
Ongoing stress/anxiety causes blood sugar to rise, to be available as a quick energy source for muscles —the body interprets stress as a sign of an imminent fight or flight.
The fight or flight response uses up the sugar and restores normal chemical balance.
In our modern world, people don’t fight or flee; they sit and seethe.
The blood sugar (glucose) remains elevated, always on standby for a fight or flight that never occurs.

Regular gym workouts may not be enough to lower blood sugar below 100 in some of these cases.
“By the same measure, two different fasting glucose tests that are done on different days, and found to be 126 or higher, and especially if one is symptomatic (increased thirst and urination, weight loss, easy fatigue) is generally enough to assess a diagnosis of diabetes,” adds Dr. Kelley.
“Symptoms of diabetes tend to be more prominent the higher and longer blood glucose levels remain outside of the norms for a healthy blood glucose range.”
 Richard Kelley, MD, is an author, speaker, fitness expert and transformation coach.
Richard Kelley, MD, is an author, speaker, fitness expert and transformation coach.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Do Barbell Squats Hurt Your Shoulders? Pain Prevention Tips

Here are several simple things you can do to help prevent or eliminate shoulder pain from barbell squats.
“Shoulder pain while barbell squatting is a common problem in people with shoulder pathology,” says Joseph Ciccone, DPT, CSCS, a doctor of physical therapy and certified strength and conditioning coach with ColumbiaDoctors in New York, NY.
What causes pain in the shoulders while squatting with a barbell across the upper back?
“Squatting with a flat barbell causes the shoulders to assume an abducted and externally rotated position, which is a high-risk position (not to mention you are applying a large force with a bar and attached weights),” says Ciccone.
Abduction means that the shoulder joints are moved away from the midline of the body.
Those whose shoulders hurt during barbell squats, says Ciccone, will likely have at least one of the following going on:
- Instability in the joint
- Rotator cuff tears or strains
- Labral tears
- Reduced mobility in the thorax and/or glenohumeral joint
- Decreased scapular mobility.
What can you do to prevent pain from barbell squats?
Ciccone says to use a different kind of bar such as a buffalo bar, cambered squat bar or safety squat bar.

Buffalo or bison bar

Cambered bar
“These types of bars allow the shoulder to be in a much safer position while still maintaining proper form during the squat exercise.”
The next preventive approach is to perform front squats, that is, holding the barbell at your front.
This isn’t a practical approach if you normally use very heavy weight loads unless you use a Smith machine.
Nevertheless, give it a try, making sure to master this version before piling on the resistance.

Front squat. Shutterstock/Syda Productions
For those who intend on sticking to light resistance, they can use different implements such as kettlebells, dumbbells and weighted vests.
Another alternative is to do single-leg squats, which can be done with body weight only, or while holding dumbbells. These can also be performed using a Smith machine.

Shutterstock/Artsplav
Shoulder Stretch
Finally, stretching the shoulder prior to barbell squats will go a long way in helping reduce or even prevent pain, depending on what’s going on in the joint in the first place, which may simply be a case of stiffness.
A most useful stretching technique is to position yourself under the bar of a Smith machine or a bar at a squat rack (as you would to prepare for squats behind the neck).
Next, place hands lightly on the bar — but very far apart — and simultaneously externally rotate the shoulders as you maintain your position, leaning forward to get in a good stretch.
Lean forward for reps, meaning, hold this position for 1-2 seconds, then release, 20 times (take your time!), for three sets prior to lifting.
 Joseph Ciccone’s practice focuses on numerous musculoskeletal conditions, including management of chronic and acute injuries, and surgical rehabilitation. He has a strong interest in adolescents, weekend warriors and professional athletes.
Joseph Ciccone’s practice focuses on numerous musculoskeletal conditions, including management of chronic and acute injuries, and surgical rehabilitation. He has a strong interest in adolescents, weekend warriors and professional athletes.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Burning Heel Pain: Five Harmless Causes

Top 5 Causes of a Burning Type of Pain in the Heels
“Burning pain in the heel can be an array of problems,” says Joseph Ciccone DPT, CSCS, a doctor of physical therapy and certified strength and conditioning coach with ColumbiaDoctors in New York, NY.
1 Plantar Fasciitis
The first up is, not surprisingly, plantar fasciitis, a more common cause of burning in the heel, says Ciccone.

Shutterstock/Alila Medical Media
He adds that plantar fasciitis can be caused by “running on hard surfaces, not changing running path/route frequently, not changing shoe wear when it is appropriate, changing running pattern, i.e., switching to a forefoot runner without proper staged progressions, not having appropriate shoe wear or support.”
2 Obesity

Shutterstock/Motortion Films
Obesity is another cause of plantar fasciitis, along with “playing sports where you need a lot of foot push-off — example basketball, racquet sports, runners — starting an exercise program without proper guidance; example: starting too aggressively.”
3 Achilles Problems
The third possible cause of burning heel pain is Achilles tendonitis/tendonopathy.
Shutterstock/Sebastian Kaulitzki
Ciccone explains, “Many people are over-pronators and need support to correct foot abnormalities, which can cause stress on plantar fascia and/or Achilles tendon — an example of this would be someone with forefoot varus (bone alignment abnormality in the toes).”
Over-pronation refers to rolling the inside part of the foot inward as you walk or run.
4 Haglund’s Deformity
The fourth possible cause of burning pain in the heels is that of Haglund’s deformity, a protruding or enlarged area on the back of the heel bone.
This growth can cause irritation and pain where the Achilles tendon attaches to the heel.
Wearing shoes with high heels, plus foot mechanics and genetics may contribute to this condition.
5 Arch Problems
No.5 is a pes planus (flat foot) or pes cavus (high arch).
Flat feet: Instead of the usual curve in the middle of the foot, the entire sole may touch the ground. This can be a condition from birth or develop over time.
High arch: This often means that only the heel and ball of the foot make contact with the ground, while the rest of the foot is elevated.
Bonus Cause: Tight Calves

Shutterstock/Shaynepplstockphoto
The sixth likely cause of a burning sensation in the heel would be tight calf muscles — those of the gastrocnemius and soleus muscles.
Tightness in these muscles can actually lead to plantar fasciitis, which is notorious for a sensation of burning in the heel.
To perform an effective calf stretch, face a wall with your hands pressed against it for support.
Position one foot forward and extend the other leg back, keeping the heel of the back foot firmly on the ground and the toes pointing straight ahead.
Gently lean into the wall while bending your front knee and keeping the back leg straight.
You should feel a stretch along the calf of your back leg.

Freepik/katemangostar
Hold this position for 15-30 seconds, then switch legs.
This stretch helps lengthen the calf muscles and can help relieve burning in the heel.
Joseph Ciccone’s practice focuses on numerous musculoskeletal conditions, including management of chronic and acute injuries, and surgical rehabilitation.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/catinsyrup

Does a Blue Mole Mean Possible Melanoma?

A dermatologist weighs in about what a blue mole most likely means and if this can signal melanoma.
“Yes, some moles will appear blue in a clinical exam and they are called blue nevus moles,” says Ben Behnam, MD, is a board certified dermatologist from Dermatology & Hair Restoration Specialists in Santa Monica, Calif.
A nevus (pronounced knee-vus) is the medical name for a mole.
Dr. Behnam continues, “In reality its not really blue, but instead the way the light hits, combined with the person’s skin tone, makes it looks blue.
These blue moles are typically noncancerous but might be malignant.
“They can look suspicious and I would recommend getting it checked out by a board certified dermatologist, as it is possible for some melanomas to appear as dark blue.”
Ask yourself, has the mole always been blue?
If not, get it biopsied immediately.
This means that a dermatologist excises the entire blue mole, or, at least a portion of it, for analysis under a microscope by a dermapathologist.
If you’ve been aware of the blue mole for some time, and it appears not to have changed in any way, it probably isn’t melanoma, but the only way to be sure is to get a biopsy.
It’s never too early to begin examining your skin on a monthly basis to get familiar with what all the various spots, dots and lesions on your skin look like.
This way, you can monitor for any changes of pre-existing spots, or the appearance of new spots.
Be sure the examination includes more obscure areas such as the outer ear folds, behind the ears, the eyelids, the groin, the soles of your feet and between your toes.
A new spot isn’t necessarily concerning; it could be a mere blemish.
But if it doesn’t go away after a few weeks, it would be a wise decision to have a dermatologist look at it with a handheld tool called a dermatoscope.

In addition to skin cancer treatment, Dr. Behnam provides laser, cosmetic and acne treatments, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can an Age Spot Turn into Melanoma? Yes, Says Doctor

“In a small number of cases, melanoma can start out as an age spot, but typically a melanoma looks darker, is more asymmetrical, has more variation in brown color, making it look darker, and is generally more raised,” says Ben Behnam, MD, is a board certified dermatologist from Dermatology & Hair RestorationSpecialists in Santa Monica, Calif.
It’s best to keep track of your age spots, though this will be difficult if you have a lot of them.
Make a note of how your age spots look, on an individual basis, if you don’t have that many. Examine your face up close every month.
If you’re worried about an age spot turning into melanoma, you should have a dermatologist (not a primary care physician) inspect your age marks on an annual basis.

Melanoma. Omar Bari, Philip R. Cohen/CreativeCommons
In fact, for extra reassurance, have a twice a year examination — in addition to your monthly self-exams.
But don’t obsess about this. As the years continue to march on, you can expect new benign age spots to appear.
You’ll see plenty of these just on the hands of elderly people.
Just keep track of those as you do with the other ones.
In fact, you can expect them to appear over time if you’re at least 40.
Again, do not panic if you notice a new age spot. They’re called “age spots” for a reason: They come with age!
Do not jump to the conclusion that it might be melanoma just because it wasn’t there a month ago.
In addition to skin cancer treatment, Dr. Behnam provides laser, cosmetic and acne treatments, among many others.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}