

Can Muscle Twitching Be Caused by Chronic Fatigue Syndrome?

A doctor answers the question, Can chronic fatigue syndrome cause twitching muscles.
“Chronic fatigue might cause muscle twitching in some people, but the mechanism is not clear,” says Dr. Moshe Lewis, MD, board certified in physical medicine and rehabilitation.
“Chronic fatigue remains controversial because, while sometimes a virus can be identified such as EBV or Lyme or Parvo immediately preceding the onset of the fatigue, in many cases such a well-defined time correlation remains elusive,” continues Dr. Lewis.
“When it comes to muscle twitches themselves there are a host of causes which include benign fasciculations, low grade seizure activity, decreased mineral levels like calcium and magnesium, amongst others.”
If you suspect that muscle twitching is, indeed, being caused by your chronic fatigue syndrome, then find out what can be causing the CFS.
Dr. Lewis cites the following possible causes: allergies such as to gluten; toxicity; mismanagement of stress; prior physical trauma; hormonal imbalance; lack of exercise; slowed metabolism; aging; side effects of medication; improper medication; and irritable bowel syndrome.
Chronic fatigue syndrome is a diagnosis of exclusion, meaning, other possible causes for one’s symptoms must first be ruled out.
There is no blood test or imaging study that shows the presence of chronic fatigue syndrome.
Because the symptoms of CFS can overlap with those of many other conditions, it’s important for doctors to rule out other possible causes of the symptoms through a series of tests. These include imaging and blood tests.
As for Twitching Muscles
As for twitching muscles, anxiety over a diagnosis of chronic fatigue syndrome can bring on anxiety that leads to harmless twitching.
Muscle twitching can be triggered by anxiety, stress or nervousness.
When someone is anxious or worried about a diagnosis like CFS, the body’s “fight or flight” response can be activated, leading to a variety of physical symptoms, including fasciculations.
This kind of twitching is generally harmless and is usually temporary.
It’s also possible for a person to have (simply by chance) both chronic fatigue syndrome and benign fasciculation syndrome.
BFS is a disorder characterized by a lot of muscle twitching — but also of cramping of the muscles and fatiguing easily from exertion.
Chronic fatigue syndrome does not cause benign fasciculation syndrome, nor vice versa.
CFS can also cause sleep disturbances, muscle and joint pain, headaches and even a sore throat.
Again, CFS is a condition of exclusion. All other possible causes for one’s troubling symptoms need to be ruled out in order for a diagnosis of CFS.
Though exercise can be problematic with both CFS and benign fasciculation syndrome, exercise also may be the very thing that will help improve symptoms of both conditions!
 Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ fizkes
Why Does Inactivity Make Back Pain WORSE?
![]()
Find out why inactivity is perhaps the worst thing you can do for low back pain.
Bed rest and inactivity are bad for low back pain, you may already know, but do you know why?
“Muscles need to move, as this is their key function in life,” says Dr. Moshe Lewis, MD, board certified in physical medicine and rehabilitation.
“Inactivity thus leads to muscles contracting and shortening because they have a decreased distance to traverse.
“While this process is slow, it can be quickly exacerbated by back pain or an injury.
“While it may seem natural to rest after an injury, this should be limited to two or three days. The longer one takes to move, the harder it is to get moving again.
“This presents a challenge however, because when there is evidence of significant tissue trauma such as fracture or disc herniation, or significant bone involvement such as spinal stenosis or spondylolisthesis, people will find several movements, if not all, very, very painful.”
Suppose, however, your back pain or ache is due simply to lack of exercise, and there is no bone or nerve involvement.
The muscles have shrunk and shortened. They are not being used the way nature designed them to be used, and quite literally, the adage of, “If you don’t use it, you’ll lose it,” applies here.
I’m a former personal trainer and, I hate to admit this, but some years ago I began noticing a persistent aching in my low back.
I’d lifted weights and had done other physical things for years, yet my low back developed a daily ache.
I ramped up my low back floor exercises; no change. I’d always done exercises for the lats and rhomboids, but obviously, these failed to prevent the development of this low back pain.
It was interfering with my hanging leg lifts. I tried massage therapy; no change.
I wondered what ELSE could I do, as far as exercise. There HAD to be something that would cure this low back ache.
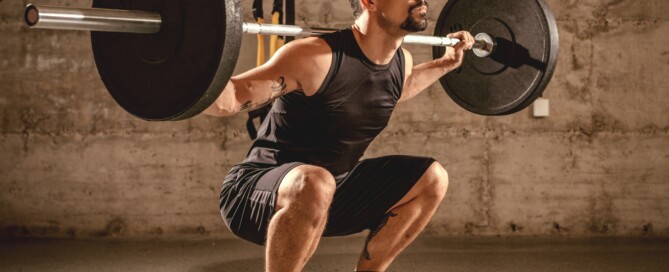
Well, there was one particular exercise that I had not considered as a solution. I gave it a try, and within eight weeks, my low back discomfort was GONE.
I’ve been doing this exercise ever since, and it’s my favorite!
It’s the deadlift — and even those who are new to strength training can do this exercise — which also helps burn excess body fat.
Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shuttertstock/Pixel-Shot

Causes of Calf Cramps in the Middle of the Night

Cramping in your calves overnight has a number of possible causes.
Many people have suffered from the sudden spasm of a calf muscle in the middle of the night, caused by tensing it a bit too much while stretching.
This pain is excruciating to high heaven, enough to make a grown man cry, but it is not a serious condition.
But what if the calf pain occurs in the absence of some careless stretching of a muscle that’s been stiffened by several hours of sleep?
This problem can occur even to physically fit people.
“Typically cramps in an athlete are caused by decreased circulation with oxygen after prolonged activity,” says Dr. Moshe Lewis, MD, board certified in physical medicine and rehabilitation.
“This phenomenon can also be seen in diabetics and smokers who also have poor circulation for different reasons.
“Classically these two groups of patients also have pain when they walk — called claudication.”
Claudication, often called intermittent claudication, is a sign of poor blood flow to the legs, causing pain or cramping during activity, typically walking, that resolves with rest.
What are some other causes of calf pain or cramps overnight?
Dr. Lewis says, “In the non-athlete or someone who has not had prolonged activity that day, night cramps are due to sciatica.
“When nerves get pinched or impinged, positional changes at night can cause muscles to go into spasm.
“This occurs because nerves send key information to muscles which lets them work correctly. When those signals are disrupted, muscles spasm.”
Sciatica is a pain that radiates down one leg, and it often begins in the lower back or buttocks.
It’s caused by irritation or compression of the sciatic nerve.
This nerve, the largest in the body, can be affected by various factors, including a herniated or bulging lumbar disc, and spinal stenosis (narrowing of the spinal canal).
There are still yet other variables that can cause calf pain or cramping in the middle of the night, though these other causes can also cause symptoms during the day as well.
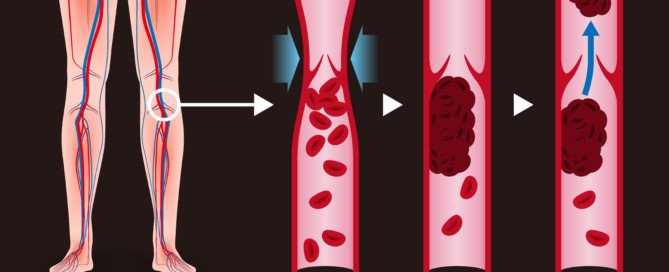
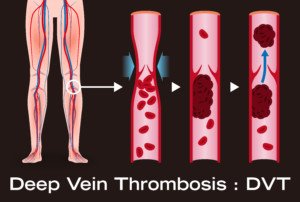
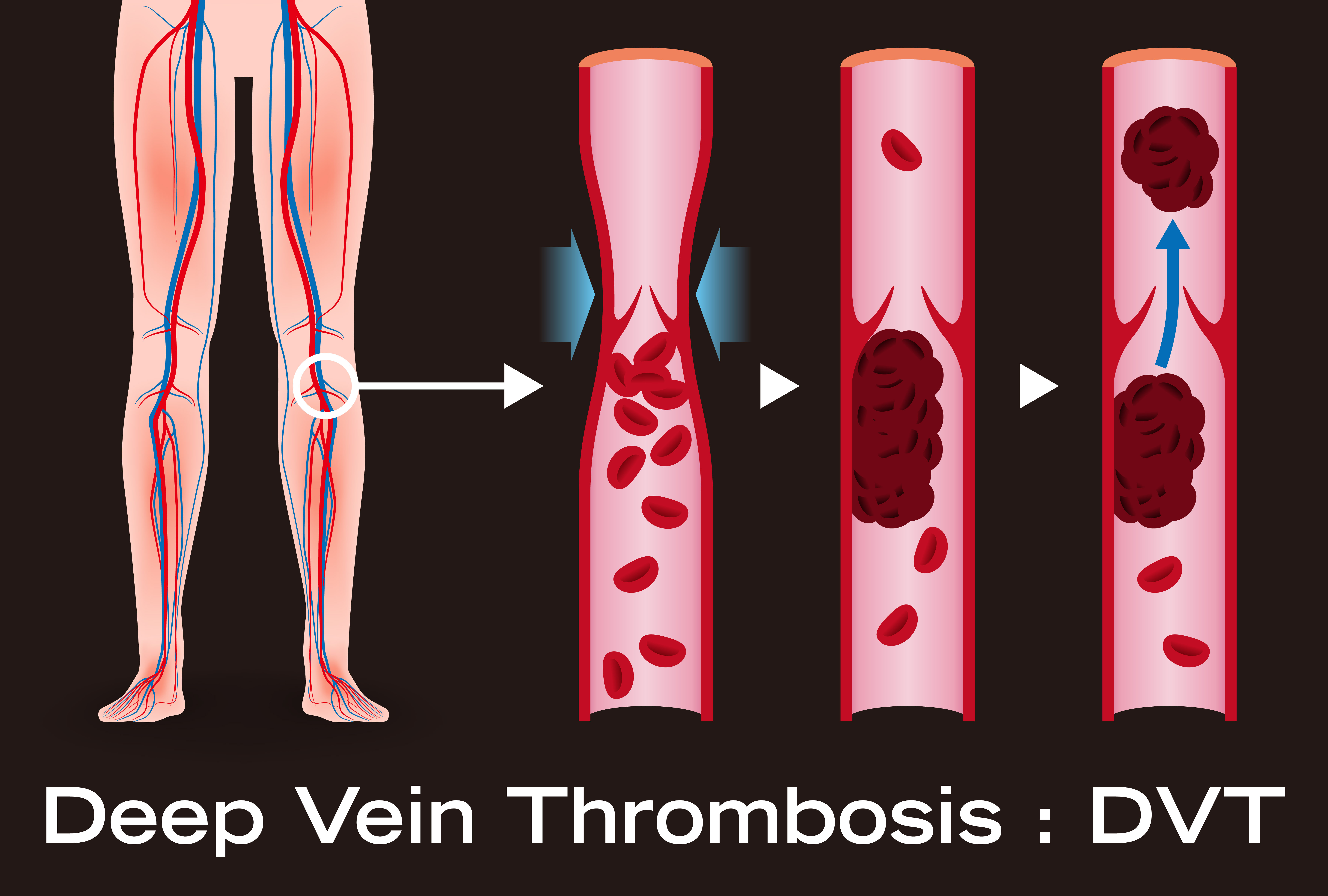
These variables are vasculitis, phlebitis, potassium deficiency and a DVT.
DVT, or deep vein thrombosis, is a blood clot that requires immediate medical attention, as it can dislodge and travel to the lungs, causing a fatal pulmonary embolism.
Risk factors for this include birth control pills, long air travel with very little movement, smoking, recent major surgery and obesity.
Another Cause of Painful Nighttime Calf Cramping
A most innocent cause, that may happen to just about anybody, is that of stretching a stiffened body upon awakening in the middle of the night.
Because one is just coming out of slumber, they’re not fully awake and hence, not alert enough to thoughtfully regulate a reflexive stretch.
The stretch is overdone, and the calf muscle gets the brunt of this, tightening up in response. The pain is excruciating.
This has happened to me, and I eventually finally came up with a solution: The moment I feel the cramp coming on, I flex my foot (moving top of foot towards shin).
This elongates the main calf muscle (gastrocnemius), opposing the tightening-up and relaxing it to its natural state: no cramp develops!
Dr. Lewis is the founder and CEO of Golden Gate Institute for Physical Medicine in CA, which provides education and clinical management of pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Prostock-studio

How Old Is Too Old for Total Knee Replacement Surgery?

Are you getting up there in years or know someone of very old age and wondering if you can be TOO OLD for total knee replacement surgery?
This surgery is invasive and comes with notorious risks such as infection and blood clots.
Age Cutoff for Total Knee Replacement Surgery
Perhaps you’ve been wondering if there’s an age cutoff for major knee procedures such as replacement or revision (of a failed replacement).
How important is old age in the consideration of surgical candidacy for knee replacements?
“Revision surgery can be done at any age if the joint has failed and the patient’s quality of life is suffering because of it,” says retired orthopedic surgeon David Fisher, MD, past Director of the Total Joint Center at the Indiana Orthopedic Hospital.

Ravedave, CC BY-SA
He continues, “Medical conditions do need to be under control and they require medical clearance, as this is a major surgery with potential complications.”
A person who’s considering joint replacement or revision surgery will need to get this clearance from the primary care physician.
Other conditions such as diabetes, kidney problems or congestive heart failure have a high potential for complicating the operation.
In other words, old age, in and of itself, is not a consideration for a total knee replacement.

Dronainfotech, CreativeCommons
Other things must be considered, such as if the patient has a weak heart, diabetes or kidney problems.
A person in his 70s, but who has congestive heart failure and obesity, can very easily be a much poorer candidate for total knee replacement surgery than a 92-year-old who’s at an ideal body weight and does not have congestive heart failure or any other serious medical problem — other than being slowed down and pained by osteoarthritis in the knees.
In short, you can’t be too old for total knee replacement surgery; the bigger patient picture needs to be considered.
 Dr. Fisher, now retired, has been involved in research and development of total hip and knee implants and has had numerous articles published in professional journals, and has participated in many research projects.
Dr. Fisher, now retired, has been involved in research and development of total hip and knee implants and has had numerous articles published in professional journals, and has participated in many research projects.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Best Ways to Prevent a DVT after Joint Replacement Surgery
The complication of DVT following joint replacement surgery can lead to a fatal pulmonary embolism.
Therefore, the best prevention tactics for a DVT must be put into place.
Other high risk surgeries for DVT are that of pelvic and intra-abdominal, says retired orthopedic surgeon David Fisher, MD, past Director of the Total Joint Center at the Indiana Orthopedic Hospital.
“There are several options available to reduce the risk of DVT/PE including a combination of pharmacologic agents (blood thinners), sequential compression devices worn on the outside of the legs or feet, and rapid mobilization postoperatively,” says Dr. Fisher.
What the Patient Should Do Preop for DVT Prevention
If you’re planning on having joint replacement surgery, the smart thing is to ask your doctor what measures will be taken to help prevent deep vein thromboses.
Don’t just assume everything will be taken care of, and don’t think for a second that you, as the patient, don’t have the right to inquire about this.
Dr. Fisher continues, “The pharmacologic agents include Coumadin (warfarin), Lovenox (low molecular weight heparin), Arixtra, Xarelto, and actually aspirin.
These agents affect the clotting cascade at different locations and act as anticoagulants.”
These drugs, but least likely aspirin, pose the potential risk of internal bleeding, since they thin the blood.
Nevertheless, in general, they definitely do reduce risk of deep vein thromboses.
Without preventive or prophylactic measures, the risk is 45 percent, says Dr. Fisher. With preventive measures, DVT risk drops to one to two percent.
One-tenth to one-half percent of joint replacement patients develop a PE, which comes from a DVT when the blood clot breaks loose and travels to the lungs.
Sudden chest pain and difficulty breathing are the two most common symptoms of a pulmonary embolus.
Is any particular preventive measure the most effective for DVT prevention?
“It is not clear which is ‘The Best,’ as they have all been proven effective,” says Dr. Fisher.
“Many surgeons like the simplicity and safety profile of aspirin and compression stockings, but there is controversy regarding the effectiveness of that combination and lack of acceptance by the American College of Chest Surgeons and the Center for Medicare Services, making it harder for surgeons to utilize this strategy,” explains Dr. Fisher.
As mentioned, the non-aspirin blood thinners are more effective than aspirin, but do come with postoperative bleeding as a possible side effect, and this can require additional surgery to correct.
“My preference is a pharmacologic agent with compression stockings and rapid mobilization (up in a chair the same day of surgery),” says Dr. Fisher.
“We have used Coumadin, Arixtra, and currently use Xarelto with the other strategies, and have maintained a DVT rate of one percent and PE rate of 0.2 percent over the past 20 years.”
Dr. Fisher, now retired, has been involved in research and development of total hip and knee implants and has had numerous articles published in professional journals, and has participated in many research projects.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/metamorworks

Failed Loosened Knee Replacement Missed by Bone Scan

Should you rely entirely on what a bone scan shows if you suspect that your total knee replacement has “loosened” or failed?
It is important to discuss this with your orthopedic surgeon.
A failed total knee replacement (TKR) can produce symptoms that are strikingly similar to those caused by other conditions such as nerve damage or spinal stenosis (narrowing of the spinal canal).
When a patient who’s had a total knee replacement presents to a doctor with complaints of knee pain, swelling, warmth and instability in walking, one consideration might be that the implants/prostheses have loosened, or have “failed.”
The doctor may then order a bone scan to see if anything suspect shows up — but how effective is this tool?
“A bone scan is a study that detects changes in bone metabolism and is nonspecific in providing results,” says retired orthopedic surgeon David Fisher, MD, past Director of the Total Joint Center at the Indiana Orthopedic Hospital.
“Increased bone activity can be caused by trauma, infection, prosthetic loosening, metabolic bone disorder.
Failed total knees may or may not stimulate a bone response depending on the cause of failure.”
Causes of Failed Knee Replacements
• Friction. The joint surfaces rub against each other, causing wear and tear over time of the implant surface.
• Infection. Bacteria can flourish on the metal and plastic components.
• Stiffness. Reduced range of motion can result in a functional deficit.
• Instability. The patient may feel that the knee might “give way” when walking. This indicates that the soft tissue that surrounds the joint is just too weak so support body weight.
• Improperly placed implants. This can cause instability.
• Fracture. A fracture around the joint can lessen stability.
Second Opinion of Bone Scan Can Be Useful
“So a bone scan is not usually necessary to determine problems with a total knee replacement and can miss many causes,” says Dr. Fisher.
Dr. Fisher, now retired, has been involved in research and development of total hip and knee implants and has had numerous articles published in professional journals, and has participated in many research projects.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/kazoka

Five Causes of Loosened Total Knee Replacement Hardware

“Total Knee replacements can ‘fail’ by a number of mechanisms,” says orthopedic surgeon David Fisher, MD, Director of the Total Joint Center at the Indiana Orthopedic Hospital.
There are five chief reasons for a failed TKR. Unfortunately, the first one that Dr. Fisher mentions brings to mind the concept of surgeon error.
He states, “In some cases, they were not implanted in a way that creates a well-functioning knee, and the patients are never happy with them. This is one of the more common causes of revision knee replacement.”
It’s deeply troubling that surgeon error cannot be proven, as the defense will blame the manufacturer of the hardware and/or loosening of the cement over time.
Dr. Fisher continues, “Another common reason is an infection develops postoperatively and leads to a need for revision.
“This may occur in 0.1-2% of knees and may be related to the volume of the operating surgeon and the hospital in which the surgery was performed.”
Following knee (and other joint) replacement or revision surgery, patients will get their temperature taken as often as once every four hours, and this includes overnight, to check for signs of an infection.
“Late infections can develop occasionally many years after implantation,” says Dr. Fisher.
The first signs of an infection may be warmth and redness about the knee.
“Loosening of the prosthesis rarely occurs in the first few years but can be a cause of late failure and will usually be associated with pain and swelling.”
The final mechanism behind a failed TKR: “Polyethylene (bearing surface) wear can also occur many years after implantation and cause symptoms of pain and swelling.”
What if your knee replacement (or hip) has been doing great since surgery?
Dr. Fisher says, “In general, it is recommended that someone with an artificial hip or knee have a regular checkup and X-ray of the affected joint to pick up on any changes that might be occurring.
“That interval could be every 2-5 years if the joint is working well.”
Dr. Fisher, now retired, has been involved in research and development of total hip and knee implants and has had numerous articles published in professional journals, and has participated in many research projects.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Miriam Doerr Martin Frommherz

General Anesthesia vs. Regional for Knee Replacement Surgery

Did you know that the use of regional anesthesia for total knee replacement surgery isn’t all that uncommon?
General anesthesia brings with it fear in many people that they’ll “never wake up.”
Don’t let the fear of general anesthesia stop you from pursuing total knee replacement surgery if your knee has reached a point of hopelessness with conservative treatment.
Yes, there are surgeons who use regional anesthesia to perform total knee replacements.
Now that you know that, it’s very logical to wonder why this approach isn’t utilized more often than general for knee replacement (or revision) surgery, since the risk of dangerous blood clots is less with the regional.
A blood clot that results from surgery is called a deep vein thrombosis (DVT).
A DVT can break loose and migrate to the lungs and kill a patient.
“In general, the risk of DVT is slightly higher with general anesthesia than with regional,” says retired orthopedic surgeon David Fisher, MD, past Director of the Total Joint Center at the Indiana Orthopedic Hospital. “With prophylaxis of anticoagulation, the risk is between 1-2%.”
Anticoagulation refers to the use of blood thinning drugs. “The risk with regional (with or without general combined) tends to be on the lower side.”
Thus, there is no doubt that regional anesthesia wins over general for knee replacement surgery as far as yielding a lower risk of DVT development.
But regional anesthesia’s advantage over general doesn’t end there.
“Additional benefits from the regional include better postoperative pain control, and decreased anesthesia side effects (nausea, vomiting, hangover effect),” continues Dr. Fisher.
“Regional options include peripheral nerve blocks, spinal anesthetic, and epidural anesthesia.
“Depending on the hospital and anesthesiologist’s abilities or competency at administering regional anesthesia, local physicians may have preferences.
“If a patient wanted regional anesthesia, I would think the surgeon would be agreeable to having it provided.”
Dr. Fisher, now retired, has been involved in research and development of total hip and knee implants and has had numerous articles published in professional journals, and has participated in many research projects.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Beets, Red in Toilet, in Urine and Poops

Beets are one of the best foods you can put in your body.
At the same time, few foods have caused more anxiety and fear than beets–because in some individuals, they cause urine to turn red or pink, making people think it’s blood.
Or, they give poops a reddish tinge as well as stain toilet water red.
The brilliant color of this vegetable means that it’s loaded with potent antioxidants.
Most people who eat beets or drink them as a whole-juiced product or as part of a mixture will not experience the undigested pigment coming out their opposite end.
The pigment is called betain, sometimes also referred to as betanin.
Below are articles that will help you fully understand this phenomenon of undigested pigment and how to tell that the red you see in the toilet or on the tissue paper is actually from the pigment in beets.

Freepik.com
*****
Poops red from beets or from blood? How to tell the difference
Reassurance is very important. You certainly don’t want to give up eating this health-giving vegetable out of fear of what you’ll see in the toilet bowl. There are key ways to detect the difference.
Guide to telling the difference between poops that are red from blood and those that are red from whole beets and beet juice.
*****
A gastroenterologist answers questions about beet juice in urine and stools.

You’ll feel even more confident after you read what a gastroenterologist has to say about this. When undigested beet juice appears in urine, this is called beeturia. Yes, it even has a name!
*****
Can you excrete an entire glass of beet juice?
Suppose you drink a glass of beet juice or even a mix that includes this nutrient dense vegetable.
The amount of beet pigment that a person may see in the toilet bowl can make them wonder if they just took in all those phytonutrients for nothing.
Can much of the juice come out in your urine?

Shutterstock/Oksana Mizina
After all, some people swig down beet juice or eat the vegetable in solid form more for the health benefits than for the taste.
As healthy as this popular vegetable is, it is highly unpalatable to many people.
Nevertheless, the health-conscious individual will eat beets anyways for their antioxidant power — and would hate to see it all go down the toilet.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Sea Wave
How NOT to Let Long Femurs Prevent a Perfect Back Squat

Don’t Let Long Femurs Stop You from a Perfect Back Squat
There’s a HUGE issue in the strength training world with femur length.
I’m a former personal trainer who has long femurs — great for karate kicking, running down hills, sprinting, pedaling … but not the best tools for the perfect back squat.
HOWEVER, I actually have a pretty decent back squat.
My back squat is below parallel WITH A LUMBAR ARCH and a moderate forward lean — nothing that I’d call a “fold” or “doubled over.” And there is no “GMing” up the weight.
I use a wider than conventional stance, though not true sumo.
I make sure that my knees track over my slightly turned out feet (I keep them out only slightly because I don’t want built-up adductors).
I have good hip flexibility to really sink down and sit in the squat.
Many women have this challenge, though it isn’t necessarily a long femur, in and of itself, but rather, a torso that’s shorter than their femurs — or, shins that are shorter than their thighs.
A woman with seemingly proportionate femurs still faces the same issue in the back squat if she has a short torso. All the time, I see women with “no torso.”
There’s nothing outstanding about their femurs until you put them up against the torso.

Torso seems to be on the short side. Shutterstock/Vladimir Sukhachev
Though Smith machine and dumbbell squats are easier than the back squat, many women (and men too) struggle with these; they often don’t even hit parallel.
Or, with the dumbbell version, if they DO hit parallel, they are folded over. Their torsos are shorter, sometimes a lot shorter, than their femurs.
I might add that at one of the gyms I go to, there’s a man who squats 365 pounds–and he’s folded over at parallel because he has a short torso; he’s “all legs,” though he’s of average overall height.
He needs to widen his stance so that there isn’t so much pressure on his lower spine.

Shutterstock/Photology1971
So it isn’t just a long femur thing with the back squat; it’s a short torso thing.
A wide stance (Sumo squat) goes a long way in making the back squat more doable for the long femur build.
Ever wonder why toddlers and preschoolers have the perfect back squat?
What are they doing differently than the adults who, even with decent proportions, still struggle with being upright?

An effortless upright position
Really now, if you had the proportions of a very young child, your nickname would be “melon head.”
In very young children, much of their height is between their hips and head, and this creates excellent leverage to stay upright.

ATG, feet flat on ground, spine upright. Shutterstock/Rozochka
Imagine if an adult had these proportions! I don’t know about you, but I’M seeing one stubby short femur that gets dwarfed by the long torso.
Here is why you shouldn’t compare an adult’s squatting form with a child’s.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}