

Trouble Breathing During or After Exercise, No Chest Pain

Find out a most unlikely cause of difficulty breathing IN during or after exercise in the absence of chest pain in an otherwise healthy person.
Suppose you just had your heart checked and everything’s normal, but you have sudden-onset difficulty breathing IN during or right after exercise (or any other time of the day, for that matter), and there’s no chest pain.
What might this be?
You may want to pay a visit to an otolaryngologist (ear, nose and throat doctor), because a condition called laryngopharyngeal reflux can obstruct breathing, says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
“Sudden or gradual voice changes, choking symptoms, coughing and shortness of breath are usually symptoms of laryngopharyngeal reflux or LPR,” says Dr. Silvers.
This condition can be misdiagnosed as exercise-induced asthma, even though, as Dr. Silvers explains, difficulty inhaling is not a symptom of asthma. In asthma, the breathing difficulty pertains to exhaling.
This condition can be misdiagnosed as exercise-induced asthma, even though, as Dr. Silvers explains, difficulty inhaling is not a symptom of asthma. In asthma, the breathing difficulty pertains to exhaling.
“LPR happens when acid reflux gets up to the level of the larynx,” she continues.
“The result of this acid is swelling at the back of the vocal cords. This swelling keeps the vocal cords from coming together properly and leads to hoarseness.
“The swelling creates a structural blockage and can make is hard to take a deep breath.”
When LPR comes on, you may have only one of its symptoms, such as difficulty breathing in, which can be quite alarming if this occurs right as you’re catching your breath after wind sprints across a gymnasium.
If trouble breathing strikes while catching your breath after a burst of exercise, you won’t be very motivated to speak to check if your voice is hoarse; you’ll be too busy struggling to inhale.
By the time the episode (which may be very brief) is over, your voice may sound normal.
“The swelling can tickle the vocal cords and cause a dry cough,” continues Dr. Silvers.
“And this swelling can give you the sensation of a lump in the throat and occasionally difficulty with swallowing.”
Diagnosis of Laryngopharyngeal Reflux
“All of these mentioned symptoms do not have to be present to make a diagnosis of LPR.
“A physical exam by an otolaryngologist can confirm this diagnosis with an examination of the larynx.
“This is a common problem with people of all ages. Even young healthy people can develop LPR during stressful periods, eating a poor diet, even during exercise. The symptoms of LPR can be constant or come and go.”
If you experience trouble breathing during or after exercise, especially if there’s chest pain, consult with a physician to rule out a more dangerous cause.
LPR is benign (though if left untreated, it can lead to esophageal cancer).
Keep in mind that trouble breathing from a heart problem isn’t always accompanied by chest pain.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Realstock

Sudden Difficulty Breathing Right After Cardio Exercise

Sudden difficulty taking breaths immediately after a cardio stint isn’t always exercise-induced asthma.
Symptoms of vocal cord dysfunction and exercise-induced asthma are nearly identical.
Symptoms between these two are so alike, in fact, that many athletes or workout enthusiasts are misdiagnosed with exercise-induced asthma, when in fact, they’ve been having bouts of vocal cord disorder.
However, this doesn’t mean you can’t, by coincidence, have BOTH conditions—which makes proper diagnosis even more tricky.
The misdiagnosis leads to inappropriate, and therefore ineffective, treatment, say researchers from Ohio State University Wexner Medical Center.
Vocal cord dysfunction goes by several different names, including paradoxical vocal cord fold motion disorder (PVFMD).
Asthma inhalers are useless for this condition, which is managed by several approaches such as Botox injections, biofeedback and vocal cord retraining therapy.
Vocal cord disorder can occur during or right after exercise, but can be triggered also by emotional stress.
It can be caused by environmental irritants that one gulps in during the heavy breathing of exercise.
The vocal cords constrict and obstruct the air flow to the lungs, making inhalation labored.
Another symptom of vocal cord dysfunction, besides difficulty breathing in, is coughing—not necessarily a hacking type of cough.
It can be a sudden cough, like something is suddenly deep in the throat. The cough may immediately precipitate the trouble breathing.
Thirty percent of the Wexner study group reported coughing during exercise.
However, vocal cord dysfunction that produces coughing doesn’t always produce the trouble inhaling.
Diagnosis of vocal cord dysfunction, post-exercise, can be made with a flexible fiberoptic laryngoscope.
Vocal cord disorder and exercise-induced asthma both can cause a whistling or “respiratory sound” upon inhaling, and diagnosis cannot be made based on what the “wheezing” of one condition sounds like compared to the other.
“PVFMD symptoms can often mimic asthma,” says Anna Marcinow, MD, study co-author.
She adds that up to “40 percent of people with asthma also have PVFMD — so it’s typical for an athlete to get the asthma diagnosed correctly, but not the vocal cord dysfunction.”
Though frightening, vocal cord dysfunction will not typically cause a person to pass out or suffocate.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/ nd3000
Source: sciencedaily.com/releases/2013/04/130412192400.htm

Can a Class 2 Heart Murmur Go Away on Its Own?

Have you been diagnosed with a class II heart murmur and are scared?
In June 2011 a cardiologist told me I had a class II heart murmur on inspiration (inhaling).
It was not something he brushed aside and he wanted to find out what was causing it.
The reason I was seeing a cardiologist in the first place was for a routine heart disease screening, and to also discuss results of my calcium score test (zero).
The stethoscope picked up the class II heart murmur.
A heart murmur is simply a distinct sound that the doctor hears via stethoscope.
Many are benign, but some can signal a condition. My subsequent echocardiogram was normal.
I then had a magnetic resonance angiogram because my doctor’s colleague suggested the possibility of a congenital pulmonary stenosis.
If it turned out that indeed I had this, then it would have to be “watched,” and I’d have to have periodic imaging to follow it.
I had no symptoms, but my doctor said that as one gets older, their pulmonary stenosis — if they have it — “becomes more relevant.”
The MRA took about an hour. When the MRA result came back normal, the doctor attributed the class II heart murmur to “robust cardiac flow” from my workouts.
Two years later I saw him for another routine checkup (just because you’re symptom-free and are at low risk for coronary artery disease, doesn’t mean you shouldn’t get routine checkups).
The class II heart murmur was GONE. In fact, the doctor said, “You now have the quietest heart murmur in the world.”
He didn’t know why the heart murmur went away. I had not stopped exercising in the preceding two years.
He did not rule out that “white coat syndrome” during the first visit may have caused it.
That’s when a person’s pulse changes due to the anxiety of being examined by a doctor.
Nervous about an MR angiogram?
Relax, there’s nothing to be afraid of.
An MR angiogram of the heart is like taking a detailed picture of your heart’s plumbing to check for any issues like blockages or irregularities.
It also looks at function. This amazing procedure can also detect other issues that are unrelated to the reason you’re undergoing it.
This MR angiogram is something to marvel at, not be nervous about.
Nevertheless, you will be given a squishy ball to hold in one hand that, when squeezed, signals to the technician that you want to exit the MRI machine — should you become claustrophobic.
In the procedure, you will lie down and keep as still as possible while the machine takes the images, which helps doctors see how well your heart and blood vessels are working.
Remember, there is no radiation exposure with an MRI procedure.
On a few occasions you’ll be asked to hold your breath for a brief period.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/lenetstan

Orange Urine vs. Dark Yellow: Telling the Difference

A proven way to tell the difference between orange urine, yellow-orange and dark yellow.
If you’ve read somewhere that orange urine can be a sign of disease and are wondering if what you’re seeing as orange is actually a dark yellow color, here are tips to better identify the actual color.
You’ll need a clear plastic cup (8-10 ounce) with about a 3.5 inch diameter.
This way, a woman can securely place the rim against her urethral/vaginal area to catch the stream of urine without it splattering anywhere.
While holding the cup firmly in place, relieve yourself. A man, of course, should use this same type of cup to empty his excrement.
Make sure you’ve allowed a good amount of urine to build before excreting it.
This is because only a few ounces of urine may appear darker, or even lighter, than it actually is.
The cup should be at least half full whenever you check the color of your urine; ideally, two-thirds to three-fourths.
Set cup on counter and clean yourself so that you’re not distracted by that aspect. Now, inspect the cup’s contents; here’s how:
Hold it up and look at it. If the urine is an obvious shade of yellow, then it is. You’re done with the test.
However, sometimes it’s hard to tell if what you’re viewing is orange urine, yellowish-orange, light orange, golden-dark yellow or dark yellow.
If you set the cup on the counter — at least if the counter is white, like mine — it will distort the color by making it a darker yellow.
Or, if the actual color of the urine is medium/dark to dark yellow, then the distortion will make it appear yellowish-orange or even deep orange, respectively. Do not be alarmed by this “refraction effect.”
This distortion is very evident with an aerial view of the cup when it’s on the counter.
Do NOT view the color when the cup is on a surface; you must hold it by your fingertips above the rim. Hold it up against a white wall or white door.
Orange vs. Dark Yellow Urine
Document the colors you see. In my case, I noted the following colors:
– Pale-clear
-Pale yellow
-Light yellow
-Medium yellow
-Dark yellow
-Yellow-orange
-Orange-yellow
-Light orange
-Orange

Shutterstock/gritsalak karalak
These colors were noted when I was holding the cup in the air and against a white wall. At the beginning of this experiment, I didn’t like seeing orange urine.
Perhaps you’ve read that a “dark” or “deep” yellow urine indicates dehydration.
However, dehydration, indeed, can cause urine to appear orange. So how can you tell if orange urine is benign or caused by a disease?
I’m not going to tell you that the following technique eliminates the possibility of disease.
What I WILL tell you is that it can reveal a PATTERN — a predictable pattern of varying degrees of color on the pale-clear to orange continuum of urine.
And sometimes, predictable patterns can be very reassuring.
Checking for Patterns
The technique is to track your water intake and exercise times.
If you just sweated up on the treadmill, your urine output after that may be orange from the water loss (dehydration).
A woman who’s having hot flashes especially, while doing cardio, may have orange urine due to the loss of water through perspiration.
After awakening in the morning, you’ll note that urine tends to be dark yellow or maybe even some degree of orange, due to an overnight dehydration process.
If you guzzle a lot of water and soon after urinate, the output likely will NOT reflect the rehydration.
It may take two hours after guzzling water for it to lighten the urine.
So don’t panic if, 90 minutes after drinking two giant glasses of water in 10 minutes, your urine is still orange.
Wait a short while for your bladder to become full again, and chances are, it will be yellow or pale.
![]()
For me, 20 ounces of water did the trick every single time.
What seemed like the output for that 20 ounces (not long after drinking it) was actually an output that was already building up in my bladder, from previous dehydration.
I’d simply wait for my next need to relieve myself, and sure enough, the urine was flaxen, a nice pale yellow.
Dark yellow urine is also likely to occur right before bedtime, unless you’ve been drinking up the water all evening.
Note how much water you’ve been drinking, and when you relieve yourself.
For me, one hatch mark indicated one cup of water. If I urinated right after that, I put the color down right below the hatch mark(s).
If I urinated, say, at least an hour later, I skipped a space and put down the color.
So when I reviewed the record, I knew that the skipped space meant that the urination wasn’t immediately after the water intake, but sometime after.
I quickly saw a pattern develop, and was soon able to easily predict the color of my urine.
Juicing fruits and vegetables may not do a good job of rehydrating you — or, at least —will not lighten urine much. Neither will milk.
I found that only WATER does this. Not once did I continue to yield orange urine despite drinking a lot of water. This is always very reassuring.
And by the way, the more dehydrated you are, the stronger your urine’s odor will be due to its concentration.
The concentration is what makes it a dark yellow, or orange.
Is your urine sometimes the color of the sunset below even though you’ve had plenty of water?
Do you occasionally see ssalmon-colored stains on the toilet paper after you wipe?

Here is a likely explanation if a deep amber color is scaring you.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Igor Nikushin
Source: mayoclinic.com/health/urine-color/DS01026/DSECTION=causes
Drinking a Lot of Water but Barely Peeing: Causes, Solutions

Can Angina Come and Go Every Second, Blinking On and Off ?

Do you get chest pain or what feels like angina that comes and goes, literally hurting one second then going away the next, like intervals?
“By definition, angina occurs when the oxygen supply to the myocardium is not adequate to meet the demand,” says Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“Theoretically, this can occur for a second or so, or it can last hours until ischemia (myocardial strain from oxygen deprivation) becomes infarction (myocardial cell death from prolonged oxygen deprivation),” continues Dr. Reynolds.
“Some patients are very attuned to their symptoms and can differentiate angina from non-cardiac aches. Symptoms will vary. Anything is possible.”
Non-cardiac conditions can cause a chest pain or ache that smarts or comes and goes like a light blinking on and off.
Two such conditions are esophageal spasms and muscle spasms. It’s not well-understood what triggers esophageal spasms, but muscle spasms are usually caused by fatigued muscles from a workout.
These non-cardiac and benign conditions can cause a smarting on-and-off chest pain that’s alarming, and each wave of chest pain may last only a second or so.
Another potential source of a “smarting” type of pain that seems near or in the chest is a gas bubble or fecal matter moving through the GI tract.
Transient irritation of nerves can also cause an intermittent pain in or near the chest.
“Angina usually occurs under emotional or physical stress when the heart is beating faster and harder and needs more oxygenated blood into the coronary arteries, but which cannot be provided by the partially blocked arteries,” explains Dr. Reynolds.
“Angina theoretically can also occur when there is a minor plaque rupture and blood flow is transiently disrupted.”
If you’ve been having chest pain that blinks on and off, lasting only seconds or even one second at a time, especially if you fear angina, get a complete cardiac exam by a cardiologist.
Before you see the doctor, however, it would be wise to document if anything triggers these episodes of smarting chest pain, e.g., do they tend to occur the day after heavy bench pressing?
Does it occur only upon inhalation? This suggests a musculoskeletal cause or possible inflammation of the sac around the lungs. Does the chest pain occur only upon exhalation? This suggests a musculoskeletal cause.
 Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Freepik.com

Angina During Rest but Never from Physical Exertion Possible

There’s a type of angina that can occur at rest but not during exertion.
Maybe you know that “unstable angina” can occur at rest, even during sleep and awaken the patient.
But this type of angina (caused by plaque buildup in the coronary arteries) will also strike when the patient exercises or induces physical exertion such as carrying a heavy box to the car or running up a flight of stairs.
But can angina occur only during rest and not during physical activity?
“There is a syndrome called Prinzmetal’s angina (also called variant angina or vasospasm),” says Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“It is not very common and often hard to document (requires a cardiac cath using provocative agent to induce spasm),” continues Dr. Reynolds.
“It is caused by vasospasm (contraction and narrowing) of the coronary arteries rather than atherosclerosis (plaque buildup). It occurs more in younger women.”
This doesn’t mean older women, or men, are immune to this condition.
“The treatment is slightly different than classic angina – nitrates and calcium channel blockers are usually used (as opposed to beta blockers),” says Dr. Reynolds.
Prinzmetal’s angina increases the risk of heart attack and sudden death, so don’t assume that just because there may not be much plaque buildup, doesn’t mean this condition is necessarily benign.
More About Prinzmetal’s Angina
The coronary artery may be as clear as a whistle, but the spasm reduces its diameter to that comparable to what severe coronary artery disease does.
However, this “variant” angina can also affect someone who already has diseased vessels.
Prinzmetal’s cannot be diagnosed with a treadmill stress test.
The most sensitive test is an IV administration of ergonovine at specific intervals. If a spasm results, this will show on a concurrent EKG.
When a coronary artery narrows either due to plaque buildup or a vasospasm, the body doesn’t know the difference — in that angina will result, even during rest.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/New Africa

Can an X-Ray Show a Heart Attack?
If you go to the ER complaining of chest pain or shortness of breath/difficulty breathing, the doctor will want to order a chest X-ray.
You may wonder if this type of image can show a heart attack or reveal clogged arteries.
Perhaps you were relieved when, in the emergency room, your chest X-ray came back “clear” or “normal,” and maybe this made you think you didn’t have coronary arteries full of sludge.
What does a cardiologist have to say?
I asked Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY, if a chest X-ray can show if a patient had a heart attack.
Dr. Reynolds replies, “No. CXR could show congestive heart failure or an enlarged heart or a myriad of other problems, but it CANNOT show a heart attack.”
Chest pain and shortness of breath are common symptoms and can be caused by a number of other conditions that an X-ray can pick up, such as pneumonia and an aortic aneurysm.
Chest pain and shortness of breath can also be caused by conditions that an X-ray cannot detect, such as gastroesophageal reflux disease, costochondritis and extreme anxiety.
Why an X-ray Can’t Show a Heart Attack
An X-ray cannot see the inside of the coronary arteries. It can certainly see the shape and size of the heart.
But this imaging tool cannot produce a picture of an obstruction inside a heart’s blood vessel.
Nor can it show the difference between cardiac tissue that’s normal and that which has been harmed by lack of oxygen.
When a patient presents to the ER with symptoms that a heart attack can cause, doctors always know that there are other conditions that can produce the same symptoms.
These conditions will show up on an X-ray. The test that is key to diagnosing a heart attack is a blood draw for an enzymatic protein called troponin.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Shortness of Breath, Chest Pain: What if Tests Are Negative?

Find out what you should do if ER testing finds nothing wrong with your heart despite chest pain and shortness of breath.
Chest pain is the No. 1 reason why people visit the emergency room. Shortness of breath is another leading reason for ER visits.
Typically, when a patient complains of chest pain with shortness of breath, they will be given a chest X ray, EKG and a blood test to track levels of an enzyme called troponin.
If troponin levels are increasing, this strongly suggests damage to the cardiac muscle: a heart attack, even a mild one.
The patient will be hooked up to a device that monitors heart rate, oxygen levels and blood pressure.
A doctor will listen with a stethoscope and feel the patient’s chest area. An EKG will be taken.
So imagine you have chest pain and trouble breathing, and all of these tests are normal.
What do you do next?

Shutterstock/ShotPrime Studio
“This totally depends on the patient – age, risk factors, how typical are the symptoms, physical exam, etc.,” says Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“Symptoms can be due to GI problems, anxiety, muscular strain, infection, etc.
“If cardiac disease is suspected, the patient usually gets referred for a stress test at some point.”
Warning: The above-named ER tests may come back normal, and you can still have dangerously blocked coronary arteries.
The troponin test detects if you’ve had, or are currently having, a heart attack.
It does NOT detect how much blockage is in your coronary arteries. Neither does a chest X-ray.
Though a doctor can tell a lot by listening with a stethoscope, this device cannot detect severely clogged coronary arteries.
An EKG test can be telling of heart disease, but some EKG readings can’t be read well (for possible severe heart disease) due to a “bundle branch block.”
If your ER tests are normal even though you have chest pain and shortness of breath, be very careful about what you decide to do next.
Your health history and absence or presence of risk factors for heart attack should weigh heavily into what should be done next.
Studies show that an MR angiogram, during the ER visit, is a reliable test for detecting severe heart disease in those with chest pain but with low risk factors for coronary artery disease.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Jamesboy Nuchaikong

Do Clear Carotid Arteries Mean Clear Coronary Vessels?

Just because your carotid arteries are “clean” doesn’t mean you don’t have severe blockages in your coronary vessels.
I was inspired to write this article after my father underwent an exam to see if there were blockages in his carotid arteries.
He underwent the exam twice because he had fallen at home but had no memory of the incident, nor was there a mechanical explanation for it.
The purpose of the carotid ultrasound was to see if there was enough plaque buildup in these arteries, which carry blood to the brain, to put my father at risk for a transient ischemic attack, which can cause a person to fall and sustain a concussion, which my father had.
A transient ischemic attack (TIA) is when a blood clot cuts off blood flow through a vessel in the brain.
These “mini strokes” can cause sudden-onset symptoms such as slurred speech, trouble forming words, facial paralysis or numbness (especially on one side), clumsiness, loss of balance, one-sided paralysis or weakness, severe headache and visual disturbances.
These symptoms may last only a few minutes or even less.
With my father, both vessels (located in the neck) were deemed normal; there was no concerning level of plaque buildup in his carotid arteries.
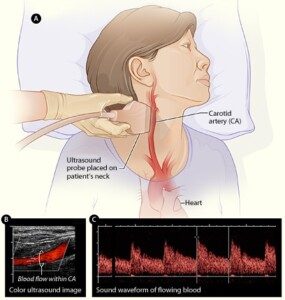
Carotid ultrasound. National Heart Lung and Blood Insitute
Can the carotids be clear in the presence of severe heart disease?
“Yes. Vascular disease tends to be system-wide — but just like most patients have more arthritis in one joint than another, most patients have an uneven distribution of vascular disease,” explains Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
If an ultrasound shows you have “clean” carotids, do NOT assume this means your coronary arteries are also clean or don’t have severe plaque buildup!
My father’s calcium score three years ago (from the initial date of this posting) came in at 1195!
A calcium score of over 450 means that a patient has a strong likelihood of severe coronary heart disease, especially if they have strong risk factors for such, which my father does.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/goodluz

Catheter Angiogram for Chest Pain but Low Heart Disease Risk?

Low risk for heart disease but chest pain? Which test is warranted: CT angiogram or catheter angiogram?
Find out what someone with low risk for heart disease should do if they have suspicious symptoms and want more than a stress test: cath angiogram or CAT scan?
Suppose you’re at low risk for heart disease (clogged arteries) in that you exercise, don’t smoke, aren’t overweight, have normal blood pressure, are not diabetic and eat mindfully, but…you’ve been having chest pains, especially upon exertion (or new-onset shortness of breath that’s out of proportion to level of activity).
Should you go straight to the cath lab? Or first undergo the non-invasive CT angiogram?
“You need to understand CT angio vs. cardiac cath angio before you throw up your hands in despair,” says Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“In summary – CT angio is really not much safer than a traditional cardiac cath.”
The CT angiogram involves significant radiation exposure, but the cath angiogram requires threading a catheter through the coronary arteries.
“And if significant disease is found, only the traditional cardiac cath allows the operator to proceed directly to stenting,” says Dr. Reynolds.
Placing a stent can be done while the catheter is already in place, if it’s determined that’s all the patient needs (i.e., bypass surgery not needed).
“CT angio for coronary arteries was the hot topic a few years ago, but has since fallen out of favor for several reasons,” continues Dr. Reynolds.
First of all, if one’s coronary calcium score is high enough, the calcified deposits will make it difficult to interpret the image from a CT angiogram.
“Patients with CAD almost always have significant calcium deposits. So CTA is really only useful in patients WITHOUT coronary disease, i.e., in healthy patients to rule out CAD.
“Here’s the downside of the CTA – CTA still requires injection of contrast dye and involves radiation,” says Dr. Reynolds.
“Therefore, the risk of an allergic reaction to the dye or risk to the kidneys from the dye in renal patients is the same whether you get a CTA or cath.
“The only advantage over a regular cardiac cath is that the test is performed using a peripheral IV rather than a central stick (usually into the femoral artery).”
Renal pertains to kidneys. The femoral artery is the main thigh artery.
“As I noted above, the other downside to CTA is that if disease is found, you can’t do anything about it. If a stent is needed, the patient then needs to have a cardiac cath to place the stent.”
When my mother was admitted to the hospital (from the ER) with chest pain, the cardiologist ordered a catheter angiogram; he bypassed the CT angiogram. Why?
Because my mother was at very high risk for severe heart disease or cardiac problems based on several factors: 1) Slightly elevated troponin level during ER visit, 2) Elderly age, 3) Abnormal echocardiogram, 4) High triglycerides.
Why waste time on a CTA with this type of patient?
It would only delay what the cardiologist probably was already anticipating: a need for a stent or even bypass surgery, plus expose her to unnecessary radiation and possible insult to kidneys from the contrast dye.
The catheter angiogram revealed “significant blockage” and about two hours later, she was undergoing quintuple bypass surgery!
“So here we go again – PRETEST PROBABLILITY OF DISEASE – if the doctor thinks a patient has normal coronaries but the patient has ongoing symptoms or is worried about coronary disease (CAD), a CTA can be done to rule out CAD,” explains Dr. Reynolds.
“This is being done more and more in the ER setting to expedite the evaluation process.” See link above in yellow highlight.
“However, if a patient is likely to have coronary disease (or the patient had a high CT calcium score), a cardiac cath is a better, more useful, more direct, and really safer approach to diagnosing and treating the disease.
“Current complication rates for cardiac cath, stent, etc., in a generally healthy patient are extremely low!
“Most complications occur in patients with unstable coronary disease and multiple medical comorbidities.”
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}