

How Long Before Effexor, Cymbalta, Paxil, Zoloft Take Effect?
When do effects of cymbalta, effexor, paxil and zoloft kick in?
What’s the time it takes for Cymbalta, Effexor, Zoloft and Paxil to start working?
Cymbalta, Effexor, Zoloft and Paxil are commonly prescribed antidepressants, and if you’re thinking of taking an antidepressant, you’ll be wondering how long before drugs such as Effexor, Cymbalta and Zoloft take to start creating some effects against your depression.
Just how long does it usually take before antidepressants such as Effexor, Cymbalta, Paxil and Zoloft to begin taking effect?
“At least 50 percent of those who will eventually respond to the above mentioned antidepressants will begin to demonstrate improvement within one week of treatment initiation,” explains Joe Wegmann, psychopharmacologist and licensed clinical social worker, author of Psychopharmacology: Straight Talk on Mental Health Medications.
“Users most often report an increase in energy and productivity, and a decrease in sensitivity (particularly to inappropriate comments from others), and a decrease in anger within the first seven days of use.”
If you are battling depression, and have tried holistic measures to relieve it, but natural treatments have failed, and the depression is debilitating, then it may be time to consider an antidepressant.
Antidepressants can do a great job in relieving symptoms of major depression, but you may not have success with the first antidepressant that you try.
You must also ask yourself if you’re truly a candidate for an antidepressant.
A person who simply feels a little down in the dumps may decide that it’s time to take an antidepressant, before trying very effective natural treatments such as rigorous (or even moderate) exercise, a change in diet, supplementation, as well as investigating possible physical causes of mental depression, such as side effects of prescription narcotics and a medical disorder like hypothyroidism.
For some people, antidepressants have been a godsend, especially for people for whom rigorous exercise (such as hormonal exercise) is not an option, or who are so depressed that they are not able to exercise, let alone attend behavior cognitive therapy sessions.
Clinical depression can literally keep a person in bed nearly 20 hours a day.
My mother had a bout with severe depression and it was a battle just to get her to SIT UP IN BED. Thus, exercise was way out of the question.
However, exercise is a great treatment modality for people with less severe forms of depression.
Though it make take a while for the effects of Cymbalta, Effexor, Zoloft and Paxil to kick in, don’t let this stop you from trying an antidepressant if all else has failed.
Wegmann continues: “Remission of mood symptoms is tougher. This may span over an 8-12 week period.
“This is due to the fact that depression is neurotoxic. Depression suppresses levels of a key neural growth hormone known as BDNF (brain-derived neurotrophic factor), leading to the eventual death of neurons in critical memory and reasoning areas of the brain, including the hippocampus and prefrontal cortex.
“Simply put, depression causes brain damage, and it takes 8-12 weeks for antidepressants, assuming they’re working for an individual, to aid in neuron re-generation and repair this neurotoxicity,” says Wegmann.
 Joseph Wegmann is a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
Joseph Wegmann is a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Getting Off Lyrica Without Problems: Minimize Side Effects

Getting off Lyrica may cause a number of discontinuation side effects. This drug is prescribed for the pain of fibromyalgia, and the nerve pain associated with diabetes and shingles.
Quitting Lyrica suddenly can result in withdrawal symptoms including insomnia, headache, nausea, diarrhea and flu-like symptoms.
“Some people withdraw from Lyrica without any ill effects,” says Joe Wegmann, psychopharmacologist and licensed clinical social worker, author of Psychopharmacology: Straight Talk on Mental Health Medications.
I didn’t know there were any serious problems in some people quitting Lyrica until I came upon this by accident on the Web.
This was several months ago, and I filed this information deep inside my mind and forgot about it.
But looking back, I realize that people on the forum reported that getting off Lyrica was producing some very nasty side effects.
But just how widespread is this? Wegmann explains, “These forum threads don’t report on alcohol consumption, illicit drug consumption, polypharmacy issues or associated physical illnesses — very important.”
All that the Web peruser sees are the complaints by the person trying to quit Lyrica. Yes, we don’t know about other variables that can make it difficult to quit this drug.
Nevertheless, it’s a wise idea to taper off this drug, because you don’t know if you’re going to be one of the unlucky ones.
Wegmann explains: “What seems to work with those experiencing a discontinuation syndrome with Lyrica is to place them on a low dose benzodiazepine regimen (diazepam or clonazepam), in conjunction with tapering the Lyrica downward at 50 mg per week.
“This is a safe, slow taper. Many taking doses of 300 mg per day are able to discontinue the drug within seven days without ill effects.”
Here’s a little irony: After I had forgotten about the Lyrica withdrawal information I had picked up on the Web, a neurologist gave my mother two bottles of 75 mg Lyrica capsules for nerve pain associated with carpal tunnel syndrome.
She was instructed to taper ON the drug, to build it up in her system: starting out with one 75 mg capsule in the morning for a few days; then one in the morning, one at night, for a few days; then two in the morning and one at night for a few days; and so on until maintaining on the full dose of two capsules, twice a day (total 300 mg per day).
The neurologist never mentioned anything about withdrawal effects of getting off Lyrica.
And interestingly, I never recognized this drug as the one that I had read about a few months’ prior in the forum, either.
So when about a week later, my mother wanted to quit this medication altogether (she had been up to 225 mg a day by then), because it wasn’t doing anything for the pain, I thought nothing of it.
She outright quit taking Lyrica, and had no withdrawal effects at all, though of course, she’d been on it for only a week as well.
If you’re on Lyrica, consult with your prescribing physician about how to taper off to minimize withdrawal effects.
Joseph Wegmannis a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Chinnapong

Cymbalta Dizziness Withdrawal: My Solution Worked

Lessening your usual daily dose of Cymbalta can cause a thick kind of dizziness.
Cutting the dose down to wean off Cymbalta (for whatever reason) can leave a side effect of dizziness.
I witnessed it when my mother’s system suddenly was 60 mg less of Cymbalta. She had no choice but to get off Cymbalta because she changed insurance plans.
The new medical plan did not cover Cymbalta, so she got a prescription for Effexor, which belongs to the same class of drugs that Cymbalta does.
She was on 90 mg (three, 30 mg capsules) of Cymbalta per day, taken all at once every evening.
To make the transition smoothly to Effexor, she was instructed to take half a 75 mg tablet of Effexor in the morning, and then another half at night, with 60 mg Cymbalta.
She was to do this till she ran out of Cymbalta, which happened about a week later.
Her body didn’t even recognize the transition; she experienced no side effects from adding in the Effexor along with subtracting 30 mg of Cymbalta per day.
However, her body really recognized something was different when it was time to take one whole Effexor tablet in the morning, and one whole one at night, which was the step to take once the Cymbalta ran out.
The next morning, my mother was dizzy as can be, and couldn’t walk on her own. I knew it had to be from the final stage of the transition.
Because my mother had already been on the Effexor for a week with no side effects, why would increasing the Effexor dose cause so much dizziness?
On the other hand, her body was suddenly 60 mg less of Cymbalta, with NONE of this drug in her system at all at this point.
Thus, the dizziness had to be from Cymbalta discontinuation syndrome.
The dizziness dissipated when my mother sat leaning back, or was lying down. She lied down for an hour soon after getting up in the morning.
She felt fine lying down, but getting up brought the dizziness on full force. She was unable to get down the staircase without assistance.
She sat in a recliner chair and the dizziness diminished. When she sat upright, it returned. She was confined to the chair. She needed a walker to get to the bathroom.
I had an idea: Maybe this Cymbalta withdrawal dizziness had to be worked out of her system, and that wasn’t going to happen if she stayed in the recliner all day.
The dizziness was the only symptom. My mother said several times, “I feel great, except that I’m so dizzy.”
I told her to sit upright while watching TV, and let the dizziness work its way out.
She had napped in the recliner for a few hours and still, the dizziness persisted once she sat upright.
But I told her to continue sitting upright and see if the symptom diminishes. And it did.
I told her to walk around the kitchen a bit; I’d assist to make sure she didn’t fall.
Within a few minutes of walking, my mother reported that the dizziness wasn’t as bad. She then sat upright at the kitchen table.
She napped again in the recliner, and then I told her to walk around the kitchen island five times, and within a minute or so, she told me to let go of her; she felt that good.
She continued walking, and over the next five minutes, the dizziness dissipated even more.
She even did a little kitchen work, and continued staying on her feet. Not long after, the dizziness was completely gone.
A person’s first instinct, when hit with severe dizziness, is to lie down or stay reclined, and not to get up if this makes the dizziness worse.
That’s good advice if the dizziness is due to a medical problem, but in this case, it clearly seemed to be from getting off Cymbalta completely, even though she was now on a similar drug.
Effexor and Cymbalta belong to the same class of drugs, but on the molecular level, they are NOT identical.
For Cymbalta withdrawal dizziness, being up and about, and walking around, was obviously the key to resolving the problem.
IMPORTANT: The patient should walk around only with someone at their side in case they lose balance until they are sure that the dizziness is gone.
I believe that had my mother stayed put in the recliner, the symptom would have plagued her straight through to bedtime.
If you have Cymbalta withdrawal dizziness, see what happens when you do the very thing that you’d never think to do: walk around and do light housework.
However, make sure someone is right at your side at all times, ready to protect you from falling, as I did with my mother.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Five Ways to Prevent Injury from a Treadmill Desk

Learn about these five key ways to help avoid injury from the use of a treadmill workstation.
Though a treadmill desk will reverse the adverse effects of sitting all day on the job, the user can actually develop various injuries, but there are ways to prevent them.
According to Andrea Avruskin, physical therapist based in Las Vegas., here are five ways to avoid injury from a treadmill desk:

1) “Don’t walk too fast too soon.” Eager beavers will get on the unit for the first time and stay on much longer than they should, believing that walking 1 mph or even .7 mph for two hours continuously is harmless, especially if they already use a treadmill for exercise or briskly walk outdoors.
I’m a certified personal trainer. What people don’t realize is that very slow walking involves biomechanics that are quite different from those of faster walking.
This means that a person who normally does faster cardio exercise on a regular treadmill is not necessarily prepared to walk extremely slowly for prolonged stints. The result can be foot injuries that cause aching and pain.
Don’t stay on for longer than 30 minutes at first. At the first hint of foot discomfort, even if you’ve been on for only 10 minutes, get off.
Take your time working up to longer sessions on the treadmill workstation to avoid injury.
2) Avruskin says, “Use the treadmill desk for breaks from your sitting desk if using the treadmill desk all day long feels like too much.”
3) “Always use well-fitted sneakers that are appropriate for your foot type and are in good shape,” says Avruskin.
Wear your heels to work, but when it’s time to use the treadmill desk, wear walking shoes.
Injuries can be in the form of a blister. Another type of injury that’s avoidable is a corn.
4) Avruskin recommends a standing desk. “This is a perfect compromise between sitting and walking. Use a work surface that is as high as your elbows when standing.
Standing burns many more calories than sitting and keeps your muscles contracting while avoiding the distraction of constant movement of the legs.”
She adds that you should use an anti-fatigue mat and wear supportive shoes even though you’re only standing.
5) Avruskin also points out that a portable pedaler can be placed under a regular desk to keep the legs in motion without the injury risk that a treadmill workstation can invite, such as repetitive stress injuries to the feet or low back discomfort.
The bottom line with preventing injuries from a treadmill desk is to avoid rushing the process; don’t feel you must walk for six hours the first day you use the unit. Give yourself several weeks to get acclimated. Listen to your body.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.

Hate Your Flabby Inner Thighs? How to Firm Inner Thighs

Do any inner thigh exercises actually tone the inner thighs?
Do you have flabby inner thighs? Loose inner thighs? Can’t anything work to firm the inner thighs? Well, yes, and here it is.
A good inner thigh routine is the hip adduction machine — but wait, before you blow the hip adduction machine off because it hasn’t helped firm your inner thighs — this machine works only if you use it a certain way.
All the time, I see women bouncing their legs back and forth on the hip adduction machine. This contraption is also known as the inner thigh machine.

It’s called hip adduction because the motion is created by your hip joint, and it’s an adduction-type of motion: To adduct means to bring together towards the midline of the body.
So when you use this machine, you are bringing your inner thighs together against resistance.
Many women have loose, flabby inner thighs. The flab is the muscle, not fat. Muscle and fat are two distinctly different body tissues.
So when inner thighs are flabby, this is because the adductor muscles are not toned.
Set the weight light enough so that you can do 20 reps.
Set the machine’s leg pads out farther than your natural range of motion, before you get into the machine. This will guarantee greatest range of motion.
Now, get in, but you’ll need to hold the leg pads in a bit so that you can get in.
If you get in BEFORE you set up the leg pads, you will shortchange yourself as far as range of motion. Maximum range of motion is key to this.
Let the leg pads slowly drift apart until your natural tightness makes them stop. Relax and take a few breaths.
Now, start closing your legs. When you close them as far as possible, hold them in this position for four seconds.
In fact, squeeze them hard towards each other so that the portions of the machine where your inner knees are against, are pressed firmly against each other, no wavering at all.
Make sure the knee supports are against each other as though stuck like that with Velcro.
After four seconds, release all the way back; not half way, but all the way.
Immediately repeat the motion you just did, squeezing the knee supports together for four seconds. Do 20 reps. Remember to always hold that squeeze for four seconds.
Your inner thighs will burn. If you cannot make it to 20 reps while following the above technique to a tee, then the weight is too heavy. You may have to go down to 40 or even 30 pounds.
The four-second squeeze, plus the wider starting point (legs further apart than what they usually are) make this routine harder.
If 20 reps, following this technique, was a breeze, increase the weight. Do three sets, 30 seconds in between each set.
Do this regimen once or twice a week. After six to eight weeks, please write in the comments box to this article about the results you’re getting.
Note: Inner thigh routines will NOT trim fat from your inner thighs. No. No. No isolated fat loss will occur.
This is strictly about firming up loose, flabby muscle. Many women with skinny legs have flabby inner thighs.
If you want to shave inches off your inner thighs, you will have to work on losing overall body fat through a comprehensive workout program and proper nutrition.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Cara-Foto

Pec Deck vs. Cable Crossover for Chest Exercise

Here is a fair comparison of pec deck to cable crossover.
Is the cable crossover better than the pec deck for building chest muscles?
Though the cable crossover and “pec deck” target the chest muscles, these two pieces of equipment have unique properties.
Cables do allow for more of a freestyle motion, and that increases the likelihood of preventing imbalances and poor lifting technique.
Cables provide you with a greater overall awareness of the muscles you’re using.
But be careful with the cable crossover; because it has more to offer than the pec deck, it also offers more potential for rotator cuff injury.
Start with light weights; don’t dive in with super heavy stacks of weight, even if you can bench press heavy.

Shutterstock/Jasminko Ibrakovic
It’s tempting with machines to shove and push, leading to other body parts getting activated without realizing that you’re cheating.
This is especially true with the pec deck.
I can’t begin to tell you how often I see men of all ages cheating like mad on this machine.
The most observed cheat move is when the man pitches his entire trunk forward in an attempt to move his arms towards each other to get that weight stack up.
He tricks himself into thinking that his chest is much stronger than it actually is, because ultimately, the weight stack gets up.
But look at how he accomplished that: leaning way forward, rather than keeping his back fixed against the back support.
And a secondary cheat move is that of bending his arms to 90 degrees (this depends on the equipment; this exaggerated bend is done on the machine that doubles as a posterior shoulder machine).
But regardless of a machine’s make and model, the big cheat move is pitching the torso way forward.
This de-isolates the chest muscles and gets other muscles involved, and hence, Mr. Strongman can move up that big stack of weights.
Sometimes the user has a weak side when performing this exercise, and is imbalanced when doing the reps.
This can cause an injury down the line, but also cause an obvious lack of symmetry.
Once a visual imbalance becomes noticeable, it can take time, patience and consistency to work it out.
You may be better off from the get-go by sticking with cables, dumbbells and other natural implements that also engage the core more, and focusing on your form and awareness of your body.
This isn’t to say that the pec deck should be avoided. It’s a good machine for novices, and it’s a good machine to take a break from the cable crossover; you don’t want your muscles adapting too much.
The pec deck is also useful when the cable systems are occupied, which they frequently are. But remember, don’t cheat on the pec deck!
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
,
Top image: Shutterstock/Dusan Petkovic

Why Your Knee Still Hurts Months After Knee Replacement

Is it normal to still suffer knee pain months after a total knee replacement surgery?
Immediate post-surgical pain is expected, but we’re talking months here.
Knee replacement patients are given powerful narcotics to numb the post-surgical pain.
However, for how long after knee replacement surgery is it still normal to feel pain?
My father had knee replacement surgery in March of 2009, and afterward, the pain in the surgical joint never disappeared.
Of course, the pre-surgical pain of osteoarthritis went away. But now, he was left with a newpain, and the joint didn’t “feel right.”
The pain wasn’t just in the knee; it was in the area above it, and was most pronounced every time he stood up from a chair or climbed stairs. Many times, he’d say, “It just doesn’t feel right. I know something is wrong.”
A few times he speculated that it was infected. Signs of infection would include swelling, redness and fever, of which my father had none.
He even wondered if the surgeon had made a mistake with the knee replacement procedure, even though the same surgeon performed the procedure on my father’s other knee about a year prior to the second operation.
My father adhered to all the prescribed post-knee replacement surgery exercises, which included physical therapy and stretching.
He regularly went to the gym to do leg presses, leg extensions and seated leg curls. He had been doing these leg exercises long before even the first surgery.
His first knee recovered great; no lingering pain, but at some point after the second surgery, not long after he was fully up and about, the walker long behind him, he began feeling the new kind of pain in the first knee that was operated on, as well as a continuation of the new pain in the most recently operated joint.
We couldn’t figure out why this was. Finally, my father had his six-month follow-up with the surgeon, and told the doctor what kind of exercises he’d been doing.
The surgeon told him he was absolutely NOT to do any leg extensions.
My father immediately omitted leg extensions from his regimen, and continued doing the permitted exercises of leg press and seated hamstring curl.
He had also been doing body-weight squats, and the surgeon encouraged him to continue with the squatting as well. But to stay away from leg extensions.
Within a few days, my father noticed a lot of improvement, and since that time, both knees have felt great and pain-free.
So if you’ve been experiencing a new kind of pain that won’t go away, months after knee replacement surgery, and you’ve been doing leg extensions, STOP the leg extensions, and then see if the pain suddenly starts disappearing.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik

Why Are 2 Knee Replacements at the Same Time Better than One?

When two replacements are done at the same time, it’s called bilateral knee replacement.
For many patients, this is the way to go. But for some patients, it’s definitely off-limits.
Have you been told that you need a total knee replacement for both joints?
If so, you’re wondering if you should have both knees replaced at the same time or if you should have the operation for each joint separately.
“Advances in surgical techniques and improvement in the prostheses we use have improved outcomes and reduced recovery time,” says Douglas Fauser, MD, of Somers Orthopaedic Surgery & Sports Medicine Group.
“In fact, among patients with two damaged knees, many are now electing simultaneous total knee replacement, avoiding a second surgery, hospital stay and rehabilitation.”
Many patients with degeneration of this hinge joint suffer from severe symptoms in both joints and need bilateral total knee replacement.
My father was such a patient, but he elected to have one knee replacement at a time, with about 12 months between the two surgeries.
For him to have had both knee replacements at once would have been disastrous.
However, Dr. Fauser explains, “The advantages of simultaneous bilateral total knee replacement are well known.
“The patient undergoes a single surgery and anesthesia, a single hospital stay and a single rehabilitation period.
“Studies have also shown that simultaneous replacement is associated with a lower risk of post-operative infection and mechanical malfunction compared to two separate procedures.”
According to one study, 95 percent of bilateral knee replacement patients said they’d have it done this way again.
When considering bilateral knee replacement surgery, the patient must consider what kind of post-operative care he’ll receive.
My father chose to go straight home after several days in the hospital. He was nearly helpless.
The house had a staircase leading to my parents’ bedroom. He’s elderly and was close to 190 pounds.
At one point he got stuck on a stool in their bathroom, unable to get to his feet.
He was not a crutches candidate, and could not transition from the stool to the walker right before him, even though only one knee had been replaced.
My mother could not lift him and she called for me (I was staying with them to help out).
Just getting from the bed to the commode next to it was a major struggle. Using the downstairs toilet was a major production.
And then there was the surgical stocking. This thing was unbelievably hard to put on every morning (my mother or I did it, as my father could not bend forward enough to do it), and pulling it up caused pain at the surgical site.
Showering was a major task even though my father did his best to maneuver into the stall with his non-surgical leg and sit on the shower seat.
More than once, we all talked about how incredibly difficult the experience would have been had he undergone two knee replacements at once.
We were flabbergasted that an overweight acquaintance of his had actually had both knees replaced at the same time.
We couldn’t understand how this woman recovered, unless she had had live-in aides or had stayed at a skilled nursing facility.
Most studies show that the rates of cardiac, neurological and pulmonary complications following bilateral total knee replacement are higher than for unilateral, especially for people over age 80.
“Advances in surgical technique, anesthesia and recovery management have made total knee replacement a safe and effective option for more elderly patients than ever before,” says Dr. Fauser.
“But those patients who are older are also likely to be sicker and at higher risk for cardiovascular and respiratory complications.
“Clearly, every patient, along with his or her doctor, must carefully weigh all the factors and risks in deciding between simultaneous and staged knee replacement.”
So will it be both knees replaced at the same time or just one knee replacement?
It’s not the easiest decision, and it depends on the patient’s individual needs, medical history and how much family support they are projected to receive.
 Dr. Fauser is a founding partner of Somers Orthopaedic Surgery and Sports Medicine Group which was formed in 1988.
Dr. Fauser is a founding partner of Somers Orthopaedic Surgery and Sports Medicine Group which was formed in 1988.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasirin pamai

Lower Back Pain When You Wake Up: Causes and Solutions

Here’s how to eliminate low back pain when you wake up in the morning.
Your low back should not hurt or ache when you get up after a night’s sleep.
To help solve the problem of low back pain or aching in the morning, you should first know the causes.
You can be the fittest person in the world and still suffer from this problem.
However, having de-conditioned back muscles will predispose you to discomfort in the morning.
“The lower back is a very complicated structure consisting of bones, joints, discs, nerves, ligaments and muscles, to name a few,” says Dr. Tom Carpenter, corrective exercise specialist, certified personal trainer and chiropractor, inventor of Stand Corrected™, a portable harness-like stretching tool that helps alleviate back, neck and shoulder pain.
“Assuming your morning back pain is not caused by anything serious, there are some other things that could be the culprit,” continues Dr. Carpenter.
Causes of Low Back Pain in the Morning
1 What You’re Sleeping On
“The first of these might be your mattress and/or pillow. I personally use a firm mattress topped with 2” memory foam and find this very comfortable and supportive,” says Dr. Carpenter.
“It’s important that your back is getting the proper support while you sleep. After all, we spend approximately one-third of our life sleeping.
“Mattresses and foam can deform over time and should be replaced as they wear out. If you notice that yours is becoming bowl shaped or indented in one area, it’s time to go shopping for a new one.
“Also, remember to turn the mattress regularly.”
If a firm mattress doesn’t help solve the problem, you may want to consider sleeping with your torso elevated to create some flexion in your lower spine.
Prolonged low back extension due to lying on your back on a “hard” surface can lead to aching muscles.
Torso elevation will prevent that little arch in your low back from forming.
Options are sleeping against a wedge pillow; in a bed with an adjustable head; or in a recliner chair.
2 Sleep Position
“In addition, use a good supportive cervical pillow that allows you to sleep in an anatomically neutral position, and never sleep on your stomach. Side or back sleeping is okay, but never on the stomach!

“When sleeping on your side, try putting a thin pillow between the knees to take the pressure off of the lower back.
“If you sit for a good portion of the day and then sleep on your side with your knees bent, then the psoas muscles (you have a right and a left) could be causing your pain.
“These muscles are powerful hip flexors which are necessary for bending and bringing the knees up when walking, running and climbing. They help to stabilizing the core as well.
“They are attached to all of the lower back vertebra and travel down to the hip area.
“When you keep them flexed for extended periods of time, such as prolonged sitting and sleeping with knees bent, they can become shortened and eventually overly tightened, pulling on the spine and causing back pain.”
Psoas Muscle Stretch in Your Bed
“There are several ways to stretch the psoas safely and effectively,” says Dr. Carpenter.
“One simple psoas stretch can be performed by lying face up near the edge of the bed.
“Bring one knee to your chest and let the other leg gently drop off the edge of the mattress.

“Let the extended leg gradually stretch for about 10-15 seconds, and then repeat with the other leg.
“If you feel any pain, stop immediately and consider discussing it with a back specialist.
“As we sleep, the discs between the vertebra in the back will tend to rehydrate, causing them to swell.
“This natural swelling can put additional pressure on areas of the back that might be susceptible to discomfort, such as from bulging discs, strain muscles or ligaments, old injuries, poorly conditioned posture muscles or a variety of other reasons.
“As we move around, this extra fluid gradually dissipates, and the back tends to loosen up, so to speak.
Two More Simple Stretches
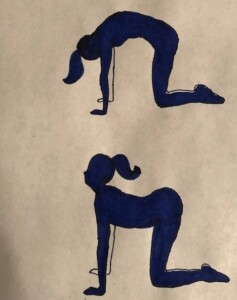
“Two simple stretches that can help with this loosening process are the sun salutation stretch and cat/dog stretch,” says Dr. Carpenter.
“Repeat this several times until the back feels looser. This motion tends to elongate the spine and traction of the discs.”
Dr. Carpenter continues: “For the cat/dog stretch, you position yourself on your hands and knees.
“First, breathe in while gently dropping the stomach down and lifting the head up. Hold for 2-3 seconds.
“Next, while exhaling, tighten the stomach muscles and arch the lower back upwards (like a cat) while letting the head drop all the way down. Repeat this several times.
“Again, this motion will help to traction the lower spine and help the back to relax.”
For best results, you should stay consistent with these two exercises.
When you practice consistency and patience, these two exercises will help your morning back pain or aches should disappear.

Photo credit: Aleesia Forni
Based upon 30+ years of experience, Dr. Carpenter’s practice approach reflects his belief that restoring optimum health and function will enable his patients to enjoy a much greater amount of vitality and wellness. Chiropractic care is true health care, not sick care!
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Stasique

Lower Back Pain Relief Naturally without Drugs
Prescription drugs only mask back pain; they do nothing to cure back pain.
If you suffer from chronic back pain, here are natural ways for back pain relief.
In most cases of chronic low back pain, the cause is bad posture. Low back treatment usually consists of painkiller drugs. But natural back pain remedies are the smart way to go.
Natural back pain relief is more applicable to the chronic lower back pain that results from incorrect biomechanics.
Say No to Drugs
It’s tempting to pop pills because they numb low back pain quickly, whereas natural treatment for back pain requires patience.
But you need to feel your back pain in order to know what movements aggravate it, and what you CAN do.
How will you know that your bad posture while sitting aggravates your back pain if you are numbed with drugs?
Set your sites on healing back pain, rather than drug-induced temporary back pain relief.
Most cases of chronic low back pain (and sometimes middle back) are caused by imposing forces on the low back muscles that they were not designed to absorb.
See your doctor for back pain resulting from acute trauma such as falling from a height or off a bike, or back pain that’s accompanied by tingling or numbness.
But again, most chronic back problems stem from mis-use of the low back muscles.
- The muscles get out of whack
- They get stiff and tight
This kind of back pain may hurt to high heaven, but does not involve slipped, bulging or ruptured discs, herniations or compressed nerves. The back pain is strictly muscular in nature; soft-tissue injury.
Back Pain Relief with Exercise
Consider hiring a fitness trainer who is knowledgeable of low back pain treatment through exercise programs.
Having been a personal trainer myself, certified through the American Council on Exercise, I know that there are personal trainers who specialize in many different areas — and rehab/injury recovery and prevention are a few of those specialties.
But even a prolific trainer with a general certification can help you naturally mitigate back pain from soft-tissue weakness and deconditioning.
Patiently executed back extension exercises will help heal low back problems. Three examples are below.

Freepik.com, yanalya

George Stepanek, CreativeCommons

Shutterstock/fizkes
So will deadlifts — but wait, before your mouth drops open at this suggestion — I do NOT mean deadlifts with a heavy barbell.
The deadlift motion can be done without any weights. Just position yourself and start moving for many reps.
Deadlifts with no weights can be challenging for the back pain sufferer. Depending on level of low back pain, the sufferer can do deadlifts while holding light dumbbells or a light barbell.

Shutterstock/Tyler Olson
There are many floor exercise routines that are great for chronic low back pain.
A fitness professional should be able to demonstrate several of these. The most popular low back pain exercise is the cat back or camel back.
Get on all fours and hunch your back like a cat does. Then reverse this position by arching it. Alternate this way for at least 15 reps.
Mattress Myths
A hard mattress might be what’s really doing your back in. It’s a myth that a soft mattress causes back pain.
A hard mattress causes the back to slightly hyperextend while the person is lying on his back.
Prolonged hyperextension will result in awakening with a lower back ache, and can cause or aggravate back pain.
A soft mattress that conforms to the curvature of your spine, while you are lying on your back, will prevent hyperextension.
The soft mattress will cause your lower back to stay in a slightly flexed position throughout sleep.
This slightly flexed position will keep the low back muscles slightly stretched, which means you will not awaken with that nagging back ache.
Lift with your legs, not back.
Finally, stop lifting with your low back. Keep low back arched whenever you lift something.
Place legs in a squat position and let your leg muscles do the lifting.
Keep torso upright as you stand up as you lift your kids, garbage, heavy potted plant, etc.
Do not lean over with your lower back to pick heavy things up.
Your back pain may just very well respond wonderfully to these natural treatments; drugs (and surgery) should be a last resort.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}