

Why There’s Pain Under Your Kneecap During or After Running

So you had a good run, but the second you stop, here comes that gnawing pain beneath your kneecap.
Or maybe it came on during your run.
What IS this and what can be done about it?
Or maybe you awaken the day after running to feel unbearable pain in the knee upon standing?
Or perhaps after sitting a while and then standing, your knee pain is hollering at you?
Causes of Running Related Pain Under Your Kneecap
I asked Dr. Kevin D. Plancher, MD, MS, FACS, FAAOS, a leading NY orthopaedic surgeon and sports medicine expert, questions about what causes knee pain in runners, and solutions to the aggravating knee pain and aching behind the kneecap, that runners often experience.
This kind of knee discomfort is called patellofemoral pain, and is also known as patellofemoral pain syndrome.
It’s also commonly referred to as chondromalacia, but you’ll soon see why these two terms are not interchangeable.
How can a person self-diagnose chondromalacia/patellar-femoral syndrome? (Some people have a large medical insurance deductible!)
Dr. Plancher explains, “Patellofemoral pain syndrome and chondromalacia patella are two separate entities, and should not be confused with one another.
“Patellofemoral pain syndrome is pain from behind the patella, and chondromalacia patella is fraying and/or damage to the articular cartilage of the patella. Chondromalacia is a surgical finding and not a diagnosis.
“Patellofemoral pain is commonly found in adolescents, especially young females, and has been estimated to account for up to 30% of all injuries seen in sports medicine clinics.
“Patellofemoral pain syndrome is a multifactorial condition, and mechanisms which cause this condition can be overuse or overloading, abnormal patellar tracking, or direct trauma.
“Other factors which may predispose an individual include muscle dysfunction, pes planus foot type, malalignment, muscle and soft-tissue tightness, congenital abnormalities of the patella or patellar groove, etc.”
Symptoms
Dr. Plancher explains, “Symptoms individuals commonly report are pain during and/or after activity, pain after prolonged sitting, crepitus (grinding), stiffness, and a sensation of giving way while ascending/descending or walking on an incline.
“The pain is usually described as a dull or achy sensation and arises from behind the kneecap.”
(This particular knee discomfort syndrome has also been described as a “fullness” sensation in the knee, or a tightness.)
Will a person with this knee problem necessarily have every single symptom?
“Individuals with patellofemoral pain syndrome may experience one or all of the previously listed symptoms,” says Dr. Plancher.
Can a person have knee pain just from running but be free of knee discomfort when climbing stairs or using the gym’s revolving staircase?
Dr. Plancher says, “Patellofemoral pain syndrome is the most common injury in runners, and running on a crowned road (repetitively in the same direction) increases the risk due to the altered biomechanics placed on the foot and ankle.
“Descending stairs typically causes more pain than ascending. This is because when descending, the contact area between the patella and femoral articulation is small, placing a great deal of stress over that small area.
“When ascending, the contact area is larger, therefore distributing the forces over a greater area.
“Patellofemoral joint reaction forces have been calculated at 3-4 times the individual’s body weight while ascending or descending.
“Patellofemoral pain syndrome is also different from jumper’s knee. Jumper’s knee is a layman’s term for patellar tendonitis.
“Patellar tendonitis is an overuse injury to the patellar tendon, which is frequently seen in jumping athletes such as basketball and volleyball players.
“The location of the pain in patellar tendonitis is typically located along the patellar tendon and not from beneath the patella.
“However, patellofemoral pain syndrome can occur in individuals who perform a great deal of jumping.”
Why is it that a person with patellar-femoral syndrome can feel minimal knee pain while running, and barely any knee pain the rest of the day after the running, but then next morning awaken with searing knee pain?
“Increased amounts of endorphins are released during moderate to strenuous continuous exercise, which may mask the symptoms during such activities,” says Dr. Plancher.
“This phenomenon can cause more harm than good, as an individual may exceed their physical limit.
“Once the effects of the endorphins wear off, the individual may start to experience pain that they did not during their run.”
Why is it that someone with chondromalacia/patellar-femoral syndrome suffers notably more knee pain after sitting for long periods, but then the knee pain dissipates somewhat after walking around?
“Individuals with patellofemoral pain have an increase in symptoms during prolonged sitting due to the increased pressure from the articulating surfaces over a period of time,” explains Dr. Plancher.
“This often dissipates somewhat after walking a short period, due to the varying forces across the knee during gait.”
The motion of squatting is strongly advised against in someone with chondromalacia/patellar-femoral syndrome, yet the very act of squatting with the thighs parallel to the floor may alleviate the knee pain in some individuals.

Freepik/master1305
In fact, for some this alleviates the discomfort after an entire leg workout session at the gym consisting of squats and leg presses. Why?
“Squatting is strongly advised against in individuals with patellofemoral pain syndrome due to the increased stress being placed through the articulation of the patella and patellar groove with active knee flexion,” says Dr. Plancher.
“However, as flexion increases, the surface area of the patella articulating with the patellar groove increases, thus decreasing the overall force placed on the joint, which may be the cause for the decrease in symptoms.”
What would cause the patella to “float” or be wobbly or loose upon lightly pressing on it, while the leg is outstretched on the floor?
“Although joint effusion is not commonly associated with isolated patellofemoral pain syndrome, an effusion may occur.
“The increased fluid in the joint may cause the patella to appear to ‘float’ compared to the uninvolved side.
“If a large effusion is present you should seek out care from a qualified sports medicine professional to evaluate if there are other pathologies present.”
At what point can a patient know he’s good to go for all-out exercise, if after the knee is feeling great for a week, he has a relapse? Is this a timeline thing?
“It’s not recommended that an individual return to their normal exercise routine immediately after their pain has resolved,” notes Dr. Plancher.
“It is recommended that the individual gradually progress their training back up to their normal exercise regimen, typically increasing their time and/or distance by 10% each week.”
This may help decrease the chance of recurrence as well as become more confident with her knee.
Gradual increases in training will also help build endurance and may help decrease other musculoskeletal injuries.
 Dr. Plancher is founder of Plancher Orthopaedics & Sports Medicine, and lectures globally on issues related to orthopedic procedures and sports injury management.
Dr. Plancher is founder of Plancher Orthopaedics & Sports Medicine, and lectures globally on issues related to orthopedic procedures and sports injury management.
 Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, health and cybersecurity topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Lopolo

Forearm Pain Doing Biceps Curls: Cause and Solution

I solved my forearm pain that occurred during biceps curls.
If you’ve been suffering forearm pain from biceps curls, you might be experiencing exactly what I experienced.
I’m a former certified personal trainer, but even personal trainers can get muscle tweaks every now and then.
I had to stop doing biceps curls because of the discomfort in my right forearm.
But the forearm pain was not caused by the biceps curls.
It was caused by neutral grip pull-ups, using the “V” bar slung atop a standard pull-up bar.

When you do pull-ups with the “V” attachment, it creates a unique stress on the lower arms.
The problem didn’t all come at once, however. After a pull-up session one day, I noticed a little discomfort in my right forearm that I connected to the pull-ups, but didn’t think too much of it.
The following week, I repeated the pull-up routine, and afterwards, felt more of the “pain” in my forearm.
In fact, while doing the pull-ups, I felt it, but didn’t think it was a big deal.
I also had been feeling the forearm “pain” while doing biceps curls.
The discomfort was located at the brachioradialis muscle, right up to the part where the arm bends.

Anatomist90, CreativeCommons
The next week, again I did the pull-ups, and afterwards, realized that whatever was going on in my brachioradialis wasn’t going away too soon.
My chest-biceps workout came three days after my pull-up workout, and I noticed that my forearm really bugged me when doing biceps curls.
The next week, I was able to do pull-ups, while still detecting the annoying tweak. But from that point, biceps curls were a problem.
For some reason, I never had to give up pull-ups; the discomfort was marginal and doable.
But during biceps curls, my forearm felt injured, and I had to finally admit it:
I had to stop doing biceps curls in order for my forearm to heal.
My elbow joint was not affected. This was a self-diagnosed muscle problem with no tendon involvement.
If a tendon were indeed involved, it should have made pull-ups painful.
On the other hand, this was the slowest-healing muscle-only injury I’ve ever had.
It kept me from doing heavy biceps curls, and in my case, I either do them heavy, or I don’t do them at all.
I hate working biceps, and doing them heavy (4-10 rep max) gets the job over more quickly.
I also couldn’t do heavy hammer curls without forearm pain.
And this forearm pain carried over to dumbbell shoulder presses, in that upon bringing the weights down to my lap after completing a set, caused pain in my brachioradialis (a forearm muscle).
To bring the weights down requires the same muscle action as the negative of a reverse biceps curl or hammer curl.
And thus, bringing the dumbbells down incited forearm pain; I use only heavy dumbbells for military press, and thus, had to replace this exercise with machine military press.
Solution to Forearm Pain During Biceps Curls
Do hammer curls with 5-pound weights, 20 reps, three sets, one minute in between sets.
It’s best that you do these standing or seated, rather than with a preacher curl machine.
If this causes annoying discomfort, stop at fewer reps, maybe 12 or even 8. If the forearm pain is really nasty, use even lighter weights.
The goal is to reintroduce the injured muscle to the concept of weightlifting, but in a baby-steps way.
Do this every time you’re at the gym if you can remember. I’d remember to do it 2-3 times per week.
The 5-pound weights actually bought out a subtle pain in my forearm, but it was very doable.
Ironically, throughout all this, I was able to keep doing the pull-ups. Strange, I know.
When 20 reps of the 5-pound weights no longer brought out forearm discomfort, I moved up to 8-pound dumbbells, and repeated the protocol: three sets of 20 reps of hammer curls.
I felt mild tweaking in the forearm, but it was very tolerable. When it disappeared, I switched to 10-pound dumbbells. You get the picture.
It took a few months before 20 reps of 15-pound dumbbell hammer curls no longer brought out the forearm pain.
At this point, I considered myself completely rid of whatever happened to my brachioradialis, and deemed myself ready to return to heavy biceps curls and dumbbell military presses.
Oddly, despite a two-month absence from biceps curls, I hadn’t lost much strength; I was at about 95 percent.
There was also no forearm pain upon bringing dumbbells down to my lap after finishing a shoulder press set, though there was some loss of strength.
Forearm pain while doing dumbbell curls?
Avoid that which really brings out the forearm pain, and commit yourself to a “baby-steps” type of rehabilitation. BE PATIENT.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer who helped her clients achieve fat loss, muscle growth, strength and improved fitness.
.
Top image: Shutterstock/staras

Ankle Pain After Running: Causes and Solutions

Do you suffer from ankle pain after running but can’t figure out what could be causing this?
There can be a number of causes — and each cause has a unique solution.
Ligament Strain or Sprain
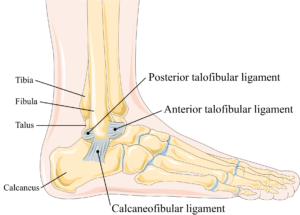
Ankle ligaments. Laboratoires Servier, CC BY-SA 3.0 creativecommons.org
Most runners have “rolled” an ankle at some point, and this can result in the overstretching or the micro-tearing of a ligament.
“The most common cause of ankle pain after running is an ankle sprain,” says Dr. Dave Candy, a board certified specialist in orthopedic physical therapy.
“This would happen after ‘twisting’ your ankle from stepping off a curb wrong or stepping on some other uneven terrain.
“This stretches or tears ligaments, usually on the outside of the ankle.”
Tarsal Tunnel Syndrome
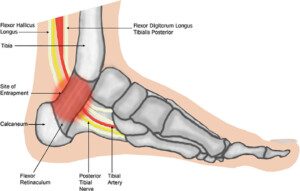
Tarsal tunnel. Nicole Williams, Jake Willet, Damian Clark, David Ketteridge/creativecommons.org
Another cause of ankle discomfort following a running session would be tarsal tunnel syndrome.
“Tarsal tunnel syndrome is an irritation or compression of the tibial nerve at the ‘tarsal tunnel’ — which is behind the bump on the inside of the ankle (medial malleolus),” says Dr. Candy.
“Most commonly, symptoms of tarsal tunnel syndrome are pain, numbness or tingling in the feet.
“This can sometimes be mistaken as plantar fasciitis. However, it is possible to have pain locally on the inside of the ankle as well.”
Osteochondral Defect or Arthritis
“Occasionally, if you run a lot of excessive mileage over a long period of time, you can develop an injury to the cartilage in the ankle joint,” says Dr. Candy.
“An osteochondral defect is an acute injury to the cartilage in the ankle joint, whereas arthritis is a gradual wearing down of the cartilage over time.”
Lack of Structured Motion
Another cause of ankle pain after some running may be simply due to lack of structured motion in the foot.
You may think you’re getting plenty of this when jogging all over the place, but jogging or running takes place in a linear path.
Unresolved Past Injury
When running causes ankle pain, this may also signal a past, unresolved injury to the foot, such as an ankle sprain that you only thought had resolved.
Sure, everything feels fine when you’re on the job, for instance, but once the feet get pounding on the pavement or treadmill, pain sets in from a not fully healed sprained ankle or strained tendon from the past.
Solutions to Ankle Pain After Your Run
Dr. Candy explains, “Adjusting mileage and frequency of running are always the first-line treatments for any of these problems. You should not run through pain.
“Ankle braces can help in the short-term for ankle sprains.
“Orthotics and/or shoes with good arch support can be helpful for tarsal tunnel syndrome and/or arthritis.”
You’ll want to try Birkenstock arch supports — these are durable, very long-lasting, comfortable and effective.

Birkenstock arch supports
“Additionally, stretching your calves and improving ankle stability through doing heel raises and balance exercises can be helpful for any of the above ankle problems.
“Outside of that, consider seeing a physical therapist to get recommendations that are more specific to your particular problem so that you can get back to running pain-free as quickly as possible.”
A great ankle ligament strengthening exercise is to walk backwards on the balls of your feet: with feet facing foward, facing outward and then facing inward.
Don’t delay if the discomfort in your ankle doesn’t seem to be diminishing once you’ve begun taking corrective measures such as new footwear, arch supports, jogging on softer terrain, stretching, cross-training, etc.
 Dr. Dave Candy, PT, DPT, is a specialist in orthopedic physical therapy and owner of More 4 Life. He’s the author of Chronic Pain: You’re Not Just Getting Older, You’re Not Crazy, And It’s Not All In Your Head, available on Amazon.
Dr. Dave Candy, PT, DPT, is a specialist in orthopedic physical therapy and owner of More 4 Life. He’s the author of Chronic Pain: You’re Not Just Getting Older, You’re Not Crazy, And It’s Not All In Your Head, available on Amazon.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.

Aching Bad Calf Cramps: Causes, Treatment, Prevention

The most agonizing pain in the calf comes at some point during your sleep, but calf cramps can also strike you during athletic training.
They can instantly halt whatever it was you were doing.
Calf cramps can be exceedingly painful, and everyone has experienced this pain at least once in their life.
What really goes on when a calf cramp comes on, which can take only a few seconds from painless to horribly painful?
There are actually several causes of calf cramps.
Dehydration is one of them. This doesn’t mean gasping for water as though you’ve been wandering in a 100-degree desert for days. You can be dehydrated and not even feel thirsty.
To prevent this, make a point of drinking six to eight glasses of water every day, whether or not you are thirsty for it.

Shutterstock/The Faces
You don’t have to drink a whole glass at once. You can sip throughout your waking moments. Lack of hydration can speed up the calf (and stomach) cramping process.
Not getting enough rest, and/or overexercising, is the next cause.
Calf cramping can occur if you’re pedaling hard on a bicycle for a prolonged period, exceeding the time that you normally spend pedaling.
Or an extra-long hiking bout up steep grades can cramp the calves up.
The cramping can come on suddenly, and if you’re a few miles from the trail head, you have no choice but to continue hiking for that distance, making the cramping worse.
Vitamin deficiency is the third possible culprit. It’s believed that the depleted levels involve phosphorus, magnesium, calcium, sodium and potassium.
Insufficient warming up also can lead to calf pain. Stiff calves are more vulnerable to cramping up.
Another cause of calves cramping up is magnesium deficiency.
“When your muscles are engaged in the rapid-fire contraction and relaxation of physical exercise, if there is too much calcium (the initiator of contractions) and too little magnesium (the initiator of relaxation), muscle cramps and a buildup of lactic acid can result,” explains Carolyn Dean, MD, ND – Medical Advisory Board Member, Nutritional Magnesium Association at nutritionalmagnesium.org.
“Eighty percent of the population has magnesium deficiency, which means that as you stretch your legs, which requires calcium to initiate that contraction in the muscle, if you don’t have magnesium to relax that muscle, the contraction continues into a cramp/charley horse or muscle spasm or twitch.”
Lastly, poor circulation, as a result of tight socks, can cramp calves.
Solutions to the Pain of Calf Cramps
An obvious solution is to cease the activity, or take a rest if you’re out in the wilderness, and massage the affected area.
Taking a magnesium supplement will also help, and Dr. Dean says it should be in powder form because this is the most absorbable.
Also do some stretching, and drink water. But to prevent calf cramps, it’s important to warm up before exercising.
I always see people jumping on the treadmill and going straight into a six or seven mph run; no slower jog preceding it, not even a walk.
It’s also not smart to exit fast running and enter straight into a seated position.
Transition out of fast running to slow running, and then a few minutes of walking, if you are vulnerable to calf cramping.
Slip in calf stretching throughout your workout, even if it’s an upper body day.
While you’re waiting for someone to finish up on the seated chest press equipment, for instance, do some calf stretching.
Drink water before, during and after exercise, whether or not you are thirsty.

Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ANN PATCHANAN
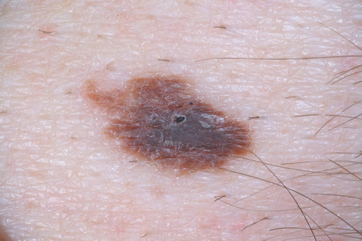
What Does Precancerous or Atypical Mole Mean?

Atypical Mole
Have you been told you have a precancerous or atypical mole?
Or maybe you were not satisfied with your doctor’s response to “What is a precancerous mole? What does atypical mean?”
Maria M. Tsoukas, MD, PhD, Assistant Professor, Dermatology Section, University of Chicago, will explain in detail just what a precancerous (atypical) mole means.
First of all, if you’re concerned about a precancerous or “atypical” mole, make sure that you consult with a dermatologist as opposed to your primary care physician.
Dr. Tsoukas explains, “Moles are common skin growths. They are correctly called melanocytic naevi (American spelling ‘nevi’), as they are due to a proliferation of the pigment cells, melanocytes.
“If they are brown or black in color, they may also be called pigmented nevi. Moles are benign in nature (harmless), but malignant melanoma (cancerous) may arise within a mole.”
About 30 percent of melanomas arise in a pre-existing lesion.
Dr. Tsoukas continues, “Some of the nevi appear since birth. There can be nevi that normally appear till around the 35th year of age.
“In pigmented and non-pigmented melanocytic nevi, we may identify clinically and histologically [with a microscope] certain atypical features.”
Atypia means the cells show some unusual features.
“In clinical examination by an expert, even when atypia is detected, malignancy cannot be excluded,” says Dr. Tsoukas.
“In those cases we obtain a specimen for histologic examination under the microscope or biopsy.”
Even if you’re planning on having a normal looking spot removed for cosmetic reasons, request a biopsy just in case.
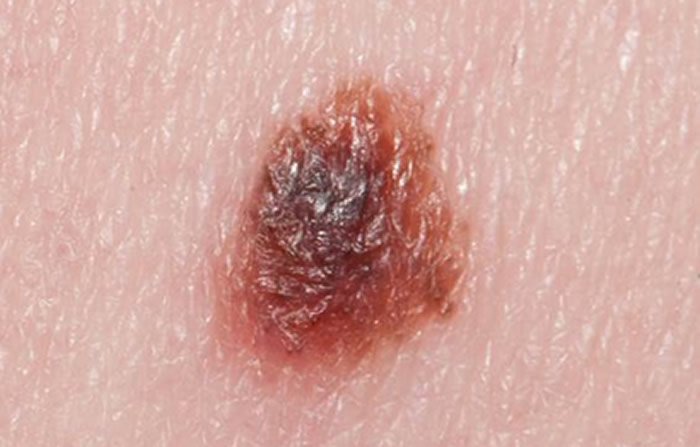
Dr. Tsoukas says that in clinical examination, dysplastic (atypical) nevi are often bigger than other moles, and tend to be abnormally shaped and colored.
They can be anywhere including non-sun exposed skin.

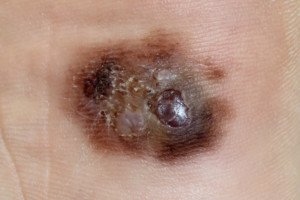
Atypical moles (dysplastic nevi). Shutterstock/Mikel Ugarte Gil

Atypical mole. Source: cancer.gov
When nevi are present with a lot of clinically defined atypical features, a biopsy is indicated to evaluate for melanoma — which kills one American every hour.
“In microscopic evaluation there are certain features that are met so as a tumor is defined as malignant,” explains Dr. Tsoukas.
“Dysplastic (atypical) nevi may present with some of those abnormal features under a microscopic evaluation.
“However, they do not meet all criteria to be diagnosed as melanomas under the microscope.”
Think of a continuum: At one end is benign, and at the other end is melanoma.
An atypical (dysplastic) mole sits somewhere between both ends of the continuum.
“This means that atypical nevi have some features that we see in melanoma, in clinical exam and under the microscope, but not all of them.”
So, in theory, any nevus that looks pathologically atypical can evolve into melanoma.
However, if the microscope shows mild atypia, this isn’t nearly as concerning as severe atypia. Moderate atypia falls somewhere in between.
Now, what percentage of melanomas actually arise from an atypical mole?
Dr. Tsoukas says those who have dysplastic nevi without family history of melanoma face a 7 to 27 times higher risk for developing melanoma.
However, this doesn’t mean that an atypical mole will necessarily transform into melanoma, although a severely atypical mole — as just mentioned — has the highest chance for melanoma transformation.
“We carefully examine and thereafter remove atypical moles (entire lesion) via biopsy or surgical excision techniques in the office.”
Having many dysplastic nevi is one of the risk factors for melanoma.
“Someone with many dysplastic nevi and personal history or with 1st-degree relatives who have had melanoma has an extremely higher lifetime risk of developing melanoma, than general population” says Dr. Tsoukas.
Melanoma under magnification. Shutterstock/Nasekomoe
Additional risk factors include: fair skin, sunburn history, indoor tanning, advancing age (though teens and children can get melanoma) and immunosuppression.
Remember the mnemonics for mole assessment: ABCDE
A – Asymmetry; one half of the mole does not match the other.
B – Border; ragged, notched or blurred.
C – Color; non-uniform and changing; mottled appearance; may include areas of red, white and blue; beware of new blackness in a mole.
D – Diameter; though melanoma is usually bigger than 6 mm (larger than pencil eraser) upon diagnosis, they can be smaller.
E – Evolving; beware of a changing mole and don’t hesitate to seek medical advice.
Dr. Tsoukas’ clinical interests include diagnosis and management of patients at high risk for skin cancer, cutaneous oncology, laser surgery and aesthetic dermatology.
clinical interests include diagnosis and management of patients at high risk for skin cancer, cutaneous oncology, laser surgery and aesthetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Sources: American Cancer Society National Cancer Institute

Are Purple Moles Normal or Possible Cancer?

Do you have a purple mole? If so, are you worried that your mole has cancer because it’s purple?
“The color of a mole may vary within normal ranges, and purple color may not necessarily mean harmful or harmless mole,” says Maria M. Tsoukas, MD, PhD, Assistant Professor, Dermatology Section, University of Chicago.
Thus, a normal mole may indeed appear to be purple. So if the question is, “Does a purple mole mean cancer?” then the bigger question should be:
Has your mole always been purple?
If it’s been this color for years, then you can assume that this is the normal nature of the skin spot.
On the other hand, if the mole has recently taken on a purple color — get it examined by a dermatologist.

Shutterstock/Albina Glisic
When a mole changes color, this can signal melanoma skin cancer, the deadliest skin cancer, with a very low five-year survival rate once this skin cancer has spread to other sites in the body.
Dr. Tsoukas explains, “The colors that we see are based on optics in human skin with regards to structures existing under our skin.
“As a general rule, red hue is due to vascular network lying in the top layers of our skin. Pigmented cells located deep in our skin may cause a bluish appearance.
“In examination of moles we are also using, along with clinical observation, dermoscopy where we have now established certain patterns of moles.
“However, confirmation is obtained by biopsy of mole and examination under microscope.”
Normal moles can come in the following colors: tan to dark brown and any shade in between; flesh colored; pink; blue; and black.
The color of a mole should be uniform.
If there is change in color, that’s when to be concerned and make an appointment with a dermatologist.
Melanoma can present in the following colors: flesh toned, white, red, blue, pink, purple, tan to dark brown, black and grey.
“Therefore, color of mole cannot confirm with regards to benign or malignant growth.”
A melanoma can be comprised of several of these colors. The key again is if the pigmented spot has been changing in color.
If you’re not sure if that purple spot on your skin has always been there, or whether or not the skin lesion has always been purple as opposed to another color, then play on the safe side and have a dermatologist look at it.
Also, what you think is a purple mole might actually be another type of skin lesion, such as a seborrheic keratosis, a benign skin lesion or barnacle that’s completely harmless.
“That’s why you need to seek medical advice to confirm,” says Dr. Tsoukas.
Dr. Tsoukas’ clinical interests include diagnosis and management of patients at high risk for skin cancer, cutaneous oncology, laser surgery and aesthetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

New Moles in Middle Age People: Melanoma or Benign?

New moles in older age are cause for concern, according to many dermatologists.
What if a newly discovered mole after age 40 looks normal?
Should you have a new mole examined anyways?
Dr. Monica Halem, MD, a dermatologic surgeon who specializes in skin cancer surgery, laser and cosmetic surgery, answers some important questions you may have.
Dr. Halem: Yes, if someone develops a new mole they should have it looked at at any age even if they think it looks benign.
Dermatologists have a special instrument called a dermatoscope where they can look closer at the pigment network than with the naked eye.
We are trained to spot certain features that can tell us if the lesion might be malignant.
The only way to definitively know is to do a biopsy if we are suspicious. Almost 100% of melanoma is curable if caught early enough.
Should you keep an extra close watch even if the doctor says it looks benign?
I would recommend that everyone watch their moles carefully.
There is the ABCDE’s of melanoma. When they check their moles they should look for the following:
A = Asymmetry. If you cut your mole if half, you want to make sure both sides are symmetric
B = Border. You want to make sure the border is regular
C = Color. You want to look for moles that are “black” or multicolored.
D = Diameter. Anything bigger than 6mm or a pencil head eraser.
E = Evolution. Anything that is changing over time, increasing in size or bleeding.

Is there a time span that, after which the new mole still appears normal, one can cease worrying that it might one day become melanoma?
Or will it always be at higher risk of becoming melanoma since it appeared during middle age?
No, there is no amount of time that can pass for a person to not be concerned.
I would not recommend that patients be anxious about their moles, but I would recommend monthly skin exams with the guidelines above.
Monthly exams followed by a yearly dermatologic exam and sooner if patients are concerned about certain spots, is adequate for surveillance.

Shutterstock/Image Point Fr
Should every new mole over age 40 be removed no matter what?
There is no need for anxiety. Follow the recommendations above as a guideline.
What percentage of new moles in men and women age 40-50 eventually become melanoma?
There are no statistical data on this. There are many different factors that cause a mole to turn into melanoma.
Most of these are still be studied. What we know now, is that it is multifactorial, including but not limited to genetics and sun exposure.
One American dies of melanoma every hour. That to me is not hype. If patients follow the recommendations above that should be more then adequate.
Is there data on what percentage a new mole will become melanoma?
There is no data on this.
As for the new moles that turn into melanoma, is there a time passage that this usually occurs?
If the spot is destined to become melanoma in middle age, does this change usually occur within a certain time frame from the “birth” of the spot?
No data on this at all. There is no way to tell in terms of timeline when a mole turns into melanoma.
Say an individual decides to just “watch” a benign-looking new spot.
If he waits for it to start changing, is it possible that the day he first notices it changing (assume he checks every month), it might have gone from normal to stage 2 melanoma?
Or is it usually the case that if one diligently monitors it, he will be able to perceive normal-to-stage 0 (very early melanoma) changes?
The latter.
If a new mole is destined to become melanoma, can its size be an indicator?
Can one assume, “Well, I don’t have to worry about it because it’s half a millimeter?”
No, there are other guidelines besides size. See above.
If a new tiny speck is a mole, how fast is it expected to increase in diameter if it stays benign?
There is no data on rate of growth.
 Dr. Halem, Founder and Medical Director of The New York Dermatologic Surgery Cosmetic Laser Center, has devoted a decade to clinical research, conducting trials that have advanced cosmetic and surgical dermatology.
Dr. Halem, Founder and Medical Director of The New York Dermatologic Surgery Cosmetic Laser Center, has devoted a decade to clinical research, conducting trials that have advanced cosmetic and surgical dermatology.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.

Fading Moles: Melanoma, or Could this Be Something Else Besides Skin Cancer?

Is a fading mole, one that’s getting lighter, worrying you about melanoma?
Have you noticed a mole on your body has been fading or getting lighter?
You’ve heard that melanoma skin cancer that develops in a pre-existing mole often manifests as a mole that gets darker, even black.
But how often does melanoma present as a mole that’s suddenly starting to fade or get lighter?
Melanoma can come in the colors of brown, black, blue, grey, red and white. A melanoma mole can start changing colors.
But what if you notice a mole that’s always been dark brown, and suddenly, it just starts getting lighter or fading?
It doesn’t necessarily change size, however. The mole only fades or gets lighter.
I’ve been conducting monthly skin checks for quite a while and was always aware of a dark mole on my back, about 3 millimeters in diameter.
It was clearly what you’d consider a “dark” mole. Every month my eyes would sweep my back for anything out of the ordinary.
To get the best view, I’d sit on my sink, and with a hand mirror, look at my back through a wall mirror to the side.
The first phase consisted of standing at the sink and viewing my back with the hand mirror while my back was angled towards the side wall mirror.
Next, I’d sit on the sink for a closer view.
Finally, I’d sit back on the sink as far in as possible, twist my back and lean in funny, maneuvering the mirror awkwardly to get the closest-possible view.
One day I was viewing my hair behind my neck, not even thinking about the spot because it wasn’t time for my skin exam.
But I caught it in my peripheral vision; it was strikingly lighter.
My eyes shifted directly to it; I couldn’t believe what I was seeing:
The mole was so much lighter all of a sudden! It had always been dark!
The mole was now significantly lighter and quite faded.
“What the f—!” I thought melanoma. Melanoma.
My last skin exam had been only 25 days previous, and it had looked the way it always had.
But now, what the f—, this mole was so much lighter, completely faded! I got in closer to examine it.
The distribution pattern of the shading was changed.
However, the size and outer shape were the same as always.
I also speculated that this was another case of follicular irritation, as I had experienced this 14 months previously with another mole; the top layer suddenly began flaking off.
The dermatologist back then had told me it wasn’t melanoma, but most likely follicular irritation.
I had told her to remove the whole thing. A biopsy came back negative.
But THIS spot now?
It didn’t look like the top layer was flaking off. I wasn’t even sure if it was even elevated, because I could never get a linear, up-close-and-personal viewing due to its location, and I had to use two mirrors.
I was not able to reassure myself that it was follicular irritation. Within minutes of the discovery of this fading mole, I made an appointment with a dermatologist.
Then I did an extensive Internet search on melanoma, which I had done before on melanoma, but this time, I discovered something I never knew about: the halo nevus.

Halo nevus (mole)
I checked my mole again; there was no halo! The Internet pictures showed very striking halos, almost neon white in some cases.
So if this wasn’t follicular irritation, and since it obviously wasn’t a halo nevus, then what else could be causing the mole to get lighter and fade?
I kept thinking melanoma. Melanoma. It’s melanoma.
A halo nevus is a mole with a very light halo of skin around it; surrounding skin starts getting much lighter than the rest of the skin; the mole starts fading, getting lighter, until eventually, it completely disappears. Halo nevus is benign.
Eight days later in the dermatologist’s office, she examined the spot; her first words were, “It doesn’t look worrisome.”
I asked, “What could cause a mole to change so quickly like this?” She replied, “I don’t think it’s a mole. It looks like a seborrheic keratosis.”

Seborrheic Keratosis
SK‘s are benign growths on the skin (see above image). I had the doctor completely remove mine just in case it might be melanoma.
Three business days later, the biopsy results were in: It was a seborrheic keratosis.
In retrospect, I realize that the spot could have easily passed for an SK while I was viewing it.
But it never dawned on me that it was an SK, because the distortion created by the two mirrors, plus the fact I could not get up-close-and-personal to view it, made it look more like a mole.
So if you ever notice a mole fading or getting lighter, don’t panic; it might be an SK.
However, see a dermatologist immediately to rule out melanoma.

These are examples of melanoma.
A mole with non-uniform fading, or disappearing sections, is highly suspicious for melanoma.
These moles have regressed areas of milky white or light grey.
Kara Shah, MD and a dermatologist, discusses dangerous regressing moles.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
.
Top. image: Shutterstock/IanRedding
mayoclinic.com/health/melanoma/DS00439; emedicine.medscape.com/article/1057446-overview

Melanoma Skin Cancer: When Changing Moles Are Benign

Melanoma: What can cause a mole to change besides skin cancer?
We’ve been alarmed by the media when it comes to changing moles — to See your doctor immediately if you have a changing mole to rule out skin cancer.
The words changing mole can dredge up the deepest fear in many people: skin cancer.
“Moles, just like the rest of our bodies, can change over time,” says Adarsh Vijay Mudgil, MD, double board certified in dermatology and dermatopathology, and founder of Mudgil Dermatology in NY.
“Subtle change over the course of years is not a melanoma,” continues Dr. Mudgil.
“Drastic change (multiple colors within a pre-existing monochromatic lesion, rapid growth, etc.) can indicate trouble, and any such lesion should be biopsied.”

Melanoma
However, melanoma usually will not cause changes in a mole that you can detect from one day to the next.
Melanoma skin cancer kills about 9,000 Americans yearly. Skin cancer can also disfigure.
- So what can cause a mole to change besides skin cancer?
- If 1,000 people have a changing mole, nobody knows how many of those will be melanoma.
If you have a changing mole, you should immediately make an appointment with a dermatologist.
But what can cause a mole to change besides skin cancer?
Follicular irritation. Some moles have a hair growing out of them. If the follicle, from which the hair grows, becomes irritated, this can cause the top layer of the mole to flake off.
This is what my dermatologist told me after she examined a changing mole on my face (biopsy was normal).
The entire layer could be gone in under two weeks: a rapidly changing mole that can scare the pants off of anyone conscious of skin cancer.
Lighting and shadows. It’s amazing how lighting-changes can create the illusion of a changing mole.
Make sure that you always check your moles in the exact same location of the house, and always under the same lighting conditions.
This means the same number of lights are used that shine above the sink mirror, for instance, or the dimmer switch is always on all the way.
Same time of day is best, and make sure light from a window is the same (i.e., curtains always drawn, or shade always up, etc.).
Variations in lighting can make a mole look like it’s changing, in that it will appear lighter or darker than usual, due to lighting fluctuations.
A light source above can also create an illusion that the top-half of the mole’s border has developed a white outline.
This is something you may have never noticed before, and because of that, the mole is “changing” and you fear skin cancer.
Skin cancer can turn parts of a mole white. When examining, examine from the same angles.
A change in angle can result in the appearance of a partially white border, created by a bright light source above.
More Causes that Aren’t Skin Cancer
Body position. Some moles, due to location, require some body contortion to get the best view. Or do they? Be aware of body contortions.

Shutterstock/Albina Glisic
One day a mole on my back appeared to be smaller and rounder: changing.
It took a few days for me to figure out that it “became” smaller and rounder when both shoulders were relaxed.
Historically, I had viewed it (during monthly skin exams) with one shoulder jutted up and forward, my back slightly twisted.
The mole is on my back and thus, I somewhat contorted myself, while sitting on the sink, to get the best, head-on view.
But this twisting and uneven shoulders stretched the skin, thereby “expanding” the mole and lessening its naturally round shape. I was used to seeing it this way.
So on the day I just happened to view it with a straight back and no jutting shoulder, it was actually its normal shape.
But because I wasn’t used to viewing it this way, I thought the mole was changing.
Always use the same body position when examining in hard-to-view locations.
Hair. I noticed that the top of a mole on my back was white, but not the same kind of white as mentioned prior. I had never noticed this before.
After a number of examinations at different angles, I discovered that the white was actually the bright light glinting off a hair just above the mole! I then began spotting other “white” hairs nearby.
If I angled my back a certain way, the white part morphed into a full-fledged hair.
The human back is full of hairs if you look closely. My back looks completely void of hair until I look closely, and then I see a ton of very short, very light hairs. This mole just happened to be smack under a hair.
Soap. One day I noticed a mole on my thigh looked a little different and had a whitish tinge to it.
It had a line down the middle I’d never seen before. The mole isn’t that big, but I could discern a line or divider down its center.
I placed my finger on it and felt texture. I’d never been able to feel it before. A mole can change by becoming elevated and changing color.
I then rubbed my finger across it and it instantly changed, appearing more like it always had.
I rubbed several times, and the white kind of flaked off it, and voila, it appeared the way it always had.
I then realized that earlier that day, soap suds had cascaded down my legs, and the mole was smack in the path. The whitish tinge and divider line had been caused by dried soap.
“It’s easy to lose the forest for the trees,” says Dr. Mudgil. “As a dermatopathologist, the majority of pigmented lesions I read are 100% benign.
“The key when examining a patient is looking for the outlier — a mole that is significantly different in appearance than what a patient naturally makes.”
 Dr. Mudgil treats infant to geriatric patients, and is versed in all aspects of medical, surgical and cosmetic dermatology. He has published extensively in the medical literature plus has lectured at numerous national meetings.
Dr. Mudgil treats infant to geriatric patients, and is versed in all aspects of medical, surgical and cosmetic dermatology. He has published extensively in the medical literature plus has lectured at numerous national meetings.
Lorra Garrick has been covering medical, health and personal security topics for many years, having written thousands of feature articles for a variety of print magazines and websites. She is also a former ACE-certified personal trainer.
.
Top image: Shutterstock/goodluz

When Brown Mole Turns Red: Melanoma or Nothing to Worry About?

Does a brown mole changing to red necessarily mean melanoma?
How many times have you read that when a mole changes color, this can be a sign of melanoma and to immediately see a doctor?
In fact, for skin cancer screening, we are told to check our ABCDE’s, and the “C” stands for color:
If a mole changes color, not only is this suspicious and should be examined by a doctor, but melanoma can cause a mole to “turn red.”
The year prior I had drawn a mole map of my lower leg so that I could then know what has apparently always been there, as far as moles.
But I never referred back to the map until a year later.
And that’s when I discovered a little dark brown spot that was not on the mole map!
It was on my shin, nearby a prominent mole, so how could I have possibly missed it when I was drawing the map?
The only explanation: It was a new mole!
Normally, moles do not appear in people over 30, though new moles can appear throughout life.
However, dermatologists are leery about new moles later in life.
New moles are common in people up to age 30. But past 30, these are to be regarded as suspicious and should be examined by a doctor.
Because I thought the spot on my shin was new, I scheduled an appointment with a doctor. She said it looked benign and I decided to just “watch” it.
I had already lined up an appointment with her prior anyways, which was two months away, for my annual routine skin exam.
I looked at this new spot three times per week for a while, then once every three days.
On a Thursday, it appeared as it always had since I discovered it: a 1-millimeter brown mole.
On Sunday, about 48 days after the doctor had examined it, it appeared a fraction larger, and had a red tinge to it.
I knew I wasn’t imagining the vague increase in size because all along, I had been measuring it up against a file card on which I had drawn two spots with a pencil: one the same size as the mole, and one just a fraction larger.
On Sunday, with the index card against my leg for a side-by-side comparison, I saw that the speck was a hair bigger than the spot that it was supposed to be the same size as, and the SAME size as the penciled spot that it was supposed to be a fraction smaller than!
Now, you might be thinking I’m a hypochondriac, but just weeks before, I had a rapidly changing “mole” removed from my back!
So I was still uptight. The changing mole on my back turned out to be a benign skin barnacle.
I was also positive I was not imagining that the spot on my leg had a new reddish tinge to it.
I had other small spots just like this one on my leg, all the same shade of brown, and when I compared this particular spot to the others, I could clearly see that it just didn’t match anymore in color.
On Monday I made an appointment to have it removed for the following Friday.
So, for five days, I suspected melanoma.
Why ELSE would this mole have developed the reddish cast and gotten a tiny bit larger?

Melanoma can be red. Source: Laurence Meyer, MD, cancer.gov
You read about how a changing mole can mean melanoma, and how when it changes colors (remember that “C”?) it can mean melanoma, and how the color red can mean melanoma in a previously brown or tan mole.
Over the next five days the mole reverted back to its original size, which provided me relief, but it remained reddish brown, though I was positive that come Friday morning, it was less red and more brown; closer to its original brown, but still tinged reddish.
Though the doctor (dermatologist) informed me that the mole was the same size as it was about 53 days prior, when she had first examined it, she then alarmed me by stating, “It looks red.”
So now I knew for sure I wasn’t imagining that the brown mole had turned a bit red.
She removed it with a “shave” procedure, taking with it a small margin of surrounding skin.
When the nurse called with the biopsy results, she said: “It’s a lentigo simplex. That means it’s benign.” She added, “A benign sun spot.”

Lentigo. Shutterstock/Dermatology11
So what had turned this brown “mole” red?
The nurse said that “simplex” is a term used to describe something that had been irritated from being scratched or rubbed.
I had no recollection of scratching or rubbing this area, but then again, it’s not impossible to be unaware of reaching down to scratch one’s leg. It can happen in your sleep.
Nevertheless, the pathology report does not lie: a lentigo simplex.
A lentigo is not a mole, even though the terms are often used interchangeably. A lentigo can look just like a mole, however.

Lentigos can be irregular in shape. Shutterstock/Roblan
And because I had thought the spot was a mole, I referred to it as a “mole” throughout this article.
But a lentigo can look just like a mole (nevus), and a lentigo can also turn into melanoma, said my doctor.
In conclusion, a brown “mole” that changes to red isn’t always melanoma, but if you notice a brown “mole” turning reddish or red, see a dermatologist, because only a biopsy can rule out melanoma. Melanoma kills around 9,500 Americans yearly.
Emily de Golian, MD
“If a previously stable mole develops a red color, blue color or new black/brown color, this may be a sign that some of the cells have become atypical, and your dermatologist will most likely perform a biopsy to examine the mole and determine if any atypia is present,” explains Emily de Golian, MD, a board certified dermatologist with Forefront Dermatology in Atlanta, GA.
“If a person is uncertain whether a mole has changed or not, the safest option is to have the mole evaluated.”


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}