

Tiny Red Bumps on Neck: Causes, Solutions

Are you flustered over all those tiny red bumps on your neck and wondering what’s been causing them?
If you have a situation on your neck that can be described as “tiny” or “small red bumps,” this has several possible causes.
“Bumps on the neck are often caused by ingrown hairs resulting from having the neck or head shaved,” says Glenn Kolansky, MD, with Advanced Dermatology Surgery & Laser Center of NJ.
Continues Dr. Kolansky, “This is especially common in patients with curly or coarse hair that grows under the skin.
“Treatment options include topical antibacterial agents and prescription cortisone to decrease the inflammation. The best treatment is to stop shaving the areas involved.”
If you must shave the affected area, make sure that it is thoroughly moisturized first with a cream or shaving gel, and make sure that it isn’t the shaving medium that’s causing an allergic reaction.
Experiment with different brands, and then shave as gently as possible with a clean new blade.
Other causes of little red bumps on your neck
Two more possibilities are bacterial or fungal. Bacteria can build up as a result of carbuncles, boils and acne.
Treatment is antibiotic creams and in more severe cases, laser, draining or surgery.
Another possible cause is a fungal infection. There will also be itching and likely discoloration. Topical anti-fungal creams are the treatment.
Let’s not forget that contact dermatitis can cause little red bumps on the neck.
This condition can be triggered by irritants or allergens like cosmetics, strong soap, chemicals and even clothes.
Treatment is corticosteroids, antihistamines and of course, removing the offending agent.
Dr. Kolansky has received the Physician of Hope Award presented by the American Cancer Society and has lectured at local and national meetings.
has received the Physician of Hope Award presented by the American Cancer Society and has lectured at local and national meetings.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com/wayhomestodio

Neck Rash: Many Causes and Many Treatments

What looks like a neck rash may not even be a rash and instead be skin cancer.
You’ve developed a neck rash and it may seem like nothing more than an annoyance, but it can have many different kinds of causes.
A true neck rash develops rather suddenly; it’s quite visible when just last week, the area looked perfectly fine.
Chances are very tiny that something that presents like this is skin cancer, since non-melanoma skin cancer grows very slowly.
What is the most likely cause of an actual neck rash?
It “can often be caused by a reaction to clothing or starch or sizing in shirts,” says Glenn Kolansky, MD, with Advanced Dermatology Surgery & Laser Center of NJ.
“It also can be an allergic reaction to type of product placed on the neck including cologne or aftershave.”
How is this type of neck rash treated?
“First is to try to figure out the agent causing the problem,” says Dr. Kolansky. “Treatment is often a topical cortisone agent, over the counter hydrocortisone. If that does not work, a prescription strength product may be required.”
What else can cause a rash appearance on the neck?
Squamous cell carcinoma, a skin cancer that kills about 3,500 Americans every year. The skin cancer can resemble a rash (when it’s not ulcerating,), but it’s not a rash.

Squamous cell carcinoma, ulcerating
Basal cell carcinoma. The same goes for this skin cancer as far as what it may resemble.
It grows extremely slowly and doesn’t metastasize, but it should be treated if you don’t want local destruction of tissues.

Basal cell carcinoma. Shutterstock/Dermatology11
Actinic keratosis. This is sun damage and only looks like a rash. It must be treated or it runs a 5-10 percent change of morphing into squamous cell carcinoma.
Treatment options for the cancer: surgery, topical prescription cream (basal cell); for the actinic keratosis, treatment is either liquid nitrogen or a prescription topical cream.
Actual rashes on the neck other than contact irritation
Eczema, candida fungus infection, viral infection, poison ivy, bug bites, acne, perfume allergy and atopic dermatitis (image above).
Careless shaving can also cause a rash on the neck. If you nick your skin, bacteria can take up residence and inflame the hair follicles (folliculitis).
Avoid shaving against the grain of the hairs to minimize this problem.
The inflammation may be treated with corticosteroids or antibiotics.
Dr. Kolansky has received the Physician of Hope Award presented by the American Cancer Society and has lectured at local and national meetings.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Beet Red Stools vs. Poop Stained with Menstrual Blood

Can a woman tell the difference between stools that have beet juice mixed in them and poop that has menstrual blood mixed in?
I’ve got this down, having ingested my share of beets, and of course, being a menstruating woman.
I am no stranger to closely inspecting my stools; I don’t get grossed out cutting them apart with a spoon and getting up close.
I began doing this when I developed microscopic colitis, and since then, I have no problem doing this.
Menstrual blood can easily get mixed in with stools, especially soft poop or diarrhea.
Red stained cervical fluid can make contact with stools as both exit a woman’s bottom at the same time.
The result is red or pinkish/brown gobs of mucus on the poop that seem part of it.
Menstrual blood is often in clot form.
Either way, it is a dark red with absolutely no hint of magenta or fuchsia, as is the case with beet juice.
Now note the fuschia color in the image above of the beet juice.
Since beet juice is pervasive and easily diffuses, it can find its way into cervical fluid that just might happen to drip out at the same time as a bowel movement.
Menstrual blood that’s mixed with stools will not easily stain a napkin or toilet tissue if you place the poop on the paper and break it apart.
However, beet juice will; it’s thin and instantly diffuses into the paper, staining it a magenta-red or fuchsia-red.
A woman may be far from her period, but upon seeing that tinged cervical fluid, might conclude there’s blood coming out of her vagina.
In reality, of course, the “blood” is beet juice that got mixed in with the cervical fluid.
Mucus also comes out with a bowel movement; this fluid helps with transit.
Beet juice doesn’t discriminate; it will find its way to intestinal mucus, so that you end up seeing tinged mucus with your stools.
Because intestinal mucus and cervical fluid look so much alike in the toilet water, one can easily mistake beet-juice-tinged intestinal mucus for blood-tinged cervical mucus. This is scary.
Keep track of when you eat beets. Don’t be afraid to get familiar with what stools and mucus look like close up.
There are telltale differences between menstrual blood and beet juice.
NOTE: Whenever in doubt, consult with a physician.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Africa Studio

Red Stools from Beets vs. from Blood: Comparison

If you had beets several days ago and are now wondering if the red in your stools is blood, there are some signs to look for that distinguish beet red from blood red in your poop.
Men are at a disadvantage here, because they don’t have the experience that women have at seeing a lot of blood in the toilet bowl (from menstruation).
But even a woman can have difficulty telling the difference between beet red from blood red in her bowel movements.
How to Tell the Difference Between Red Poop from Beets and from Actual Blood
Fresh blood on toilet paper in pure form (as would be from rectal/anal bleeding) is solid bright red. Think of how Kleenex looks when you hold it to a bloody nose.

Shutterstock/Parinya Art
From my experience with beeturia (undigested beet juice in stools, though this term usually applies to urine), the juice that appears on the tissue paper is very diffuse, creating a very light reddish-magenta or very light reddish-fuchsia.
It’s a color that menstruation just does not produce.
Again, a man can’t make the comparison unless he has a history of hemorrhoid bleeding.
In all my years of menstruating, I’ve never seen even the slightest fuchsia or magenta tinge to any amount of blood on the tissue paper.
When it’s mixed with cervical mucus, however, it’s dark pink, but a dull pink, with no hint of magenta or fuchsia, and usually, the pink has a tinge of tan.
Blood in a toilet bowl will not diffuse as much into the water as will beet juice because it’s heavier and tends to aggregate.
Have you ever had a drop from your nose or a cut fall into some water? It does not stain the entire contents, but stays rather localized, suspended in a glob.
I’ve had rectal bleeding after a colonoscopy, and trust me, pure fresh blood dripping into a toilet bowl does not disperse and dye the water; it remains suspended, aggregated, in ” liquid clumps.”
Beet juice is too thin to do this and will stain the water bowl pinkish if there’s enough of it.
Beet juice. Shutterstock/Africa Studio
However, in smaller amounts, it will remain concentrated around your stools—at least in my case it does.
Sometimes beet juice will form ribbons or rings that hover or float around poop. Actual blood in poop will be literally mixed in with it.
Beet juice tends to hover around stools like a halo, and in the water, it is crimson when it does this.
If you flush poop that’s red from beets, the juice will easily billow out into the water bowl, coloring it pink, red or reddish brown (if the poop is soft enough to mix with it).
Another test to tell the difference between beet red and blood in your stools.
Place several chunks of the colored stool on several layers of tissue paper or napkins, then roll them over to see what kind of stain they leave.
If it’s beets, the stain will be markedly magenta or fuchsia.

If you see a stain that resembles this color on your toilet paper, chances are extremely high that it’s from beet juice.
I hope this provides reassurance about beet poop vs. bloody poop.
This color will match the color the beets left behind on your cutting board or paper plates.
If it’s blood (from the lower intestinal/rectal/anal region) it will be pure red or red with a tinge of dark orange. It will retain this color when it dries.
Beet juice will quickly change to a light brown or dark gold or golden-brown.
“All stool that is black, maroon or red does not necessarily represent a gastrointestinal bleed,” says G. Shelton McMullan, MD, board certified gastroenterologist with Capital Digestive Care in MD.
“What we have recently eaten or ingested is often the culprit, and this needs to be considered before becoming alarmed.
“There are a host of foods that can make our stool red as well, including red Jell-O and beets.
“To err on the side of caution, it is recommended that you let your healthcare provider know if your stool remains discolored, however.”
 Dr. McMullan has published numerous medical abstracts and presented posters related to the management and treatment of inflammatory bowel disease and other gastroenterological conditions.
Dr. McMullan has published numerous medical abstracts and presented posters related to the management and treatment of inflammatory bowel disease and other gastroenterological conditions.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Timolina

Normal CT Scan After Hitting Head: Brain Bleed Can Still Occur
A negative CT (CAT) scan after hitting your head doesn’t guarantee that bleeding in the brain won’t eventually result.
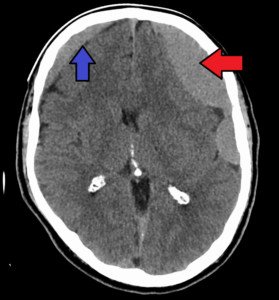
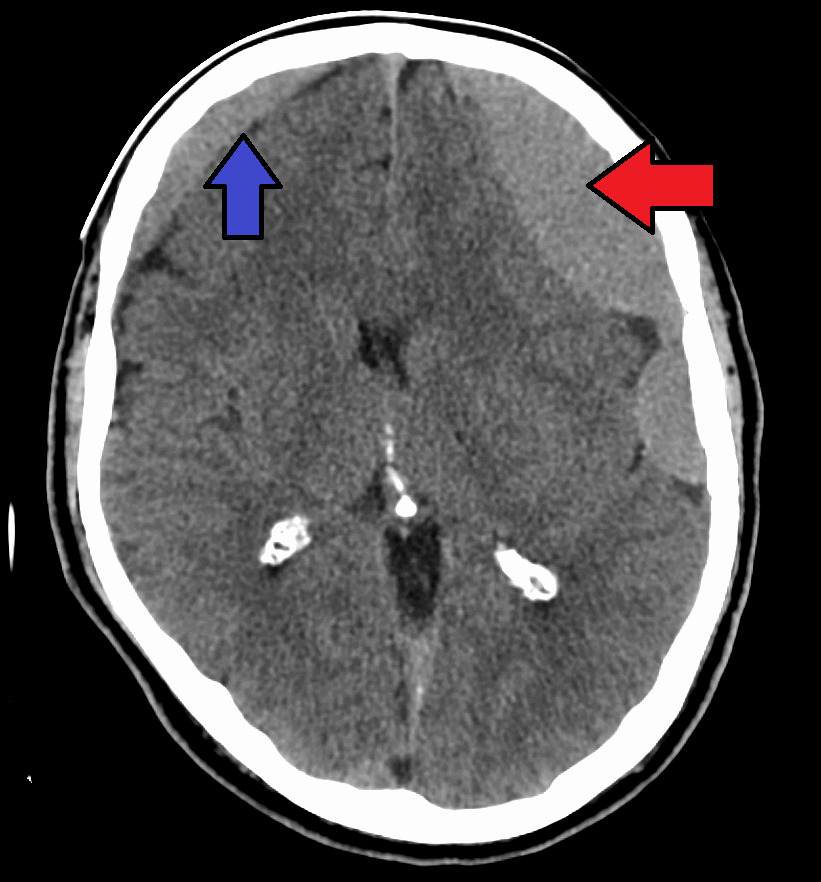
It still might, and when it does, it’s called chronic subdural hematoma (cSDH).
This happened to my mother who hit her head on a bathtub after passing out while standing.
You can imagine how hard she hit her head, since she wasn’t conscious to try to break the fall a little.
Several hours later she had a CT scan that looked perfectly normal.
She was kept for overnight observation. I was told that if her brain began bleeding, there would be neurological signs of this, that would be evident when nurses would give her neurological checks every so often.
Next morning she had another CT scan, and it was perfectly normal.
I asked the doctor about the possibility of bleeding still occurring in her brain, at some point down the road, since I had read reports in the past that getting hit in the head can cause delayed bleeding in the brain …
… up to two months later.
The doctor said there was a very tiny chance of this occurring, but that chances are, it wouldn’t, since the second CAT scan was completely normal.
My mother was discharged and I forgot about the possibility of delayed bleeding in the brain.
Six weeks later she awakened with a blazing headache and profound weakness in her legs, which I thought was a stroke.
I didn’t even think about that she had struck her head six weeks prior.
I kept thinking stroke because she had been taken off a blood thinner, Coumadin, which was prescribed for stroke prevention as a result of undergoing mitral valve replacement. The Coumadin prescription was for 90 days.
Shortly after hitting her head in the bathroom, the surgeon recommended that she cease the blood thinner because she was at risk for falling, due to unexplained orthostatic hypotensive episodes.
So she ceased the Coumadin after only 60 days. The morning she awakened with the headache and weakness was day 90 from the valve replacement surgery.
So I thought that the mitral valve replacement, in the absence of the 90-day Coumadin treatment, had resulted in a minor stroke.
The ER doctor assessed my mother and concluded that it was probably a small stroke.
Interestingly, the ER doctor never thought to ask if my mother had recently hit her head!
Because a stroke was suspected, my mother underwent a CT scan with contrast dye.
The ER doctor came back with the results and admitted being surprised at the findings: no stroke, but … bleeding in the brain.
Only then did the ER doctor ask if my mother had hit her head recently, and I was flabbergasted that all this time, I had etched the bathtub incident out of my mind.
Some of the blood in her brain was “old,” and some was “fresh.”
The diagnosis was a chronic subdural hematoma – a slow brain bleed whose primary cause is getting hit in the head.
“Elderly have weaker everything due to age,” says Danielle DonDiego, DO, a family physician with SteadyMD, an online program where patients can call, text or video chat with their doctor anytime.
“They are much more likely to have a brain bleed due to fragility from age.
“Also, many elderly are taking aspirin or a stronger blood thinner for health purposes, and this alone puts anyone at a higher risk.”
At the time my mother had hit her head, she was on the Coumadin as well as a daily aspirin.
Not Elderly?

Shutterstock/G-Stock Studio
The takeaway message here is that if you hit your head, record the date this happened, even if you’re young.
Not being elderly does not make you immune to bleeding in the brain after striking your head.
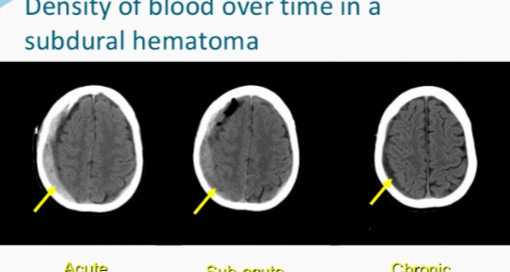
The other two types of subdural hematoma are “sub-acute” and “acute.”
Sub-acute is when the bleeding in the brain occurs three to 21 days after getting hit in, or falling on, one’s head.
The acute form has a very high mortality rate.
A normal CT scan shortly after hitting your head is always reassuring, but it doesn’t mean you’re out of the woods.
 Dr. DonDiego, who’s also a certified personal trainer, focuses on weight management, fitness, nutrition, reproductive health, preventive medicine and managing end stage disease. Learn more about SteadyMD.
Dr. DonDiego, who’s also a certified personal trainer, focuses on weight management, fitness, nutrition, reproductive health, preventive medicine and managing end stage disease. Learn more about SteadyMD.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image credit: James Heilman, MD

Burr Hole Subdural Hematoma Drain and Headaches, Neck Pain

Burr hole drainage is a standard treatment for chronic subdural hematoma, but what if the patient then complains of frequent and/or really bad headaches, or even nasty neck pain?
How common are headaches or neck pain after burr hole draining of a chronic subdural hematoma?
“Headache is a fairly common complaint after a burr hole washout of a subdural hematoma,” says Kangmin Daniel Lee, MD, a neurosurgeon with New Jersey Brain and Spine.
“Pain fibers are carried in the dura, and since the dural covering is opened to drain subdural hematomas, this can be one source of headache.
“Also, if there has been incomplete evacuation of the hematoma, this can also be a source of headache.
“Finally, there is often incisional pain which can be disguised as a headache.”
My mother had a burr hole drainage of her chronic subdural hematoma.
That day, following the surgery, and for a few days after, she complained of headaches.
But they weren’t nearly as bad as the headache (from the chronic subdural hematoma) that she suffered prior to the surgery.
I assumed it was only natural to have a headache after surgery on the head.
I’d ask my mother to place her fingers where the headache hurt the most, the “epicenter” of the headache pain, and she’d always place her fingertips smack on the incision area.
A few days after the burr hole drainage, my mother experienced sudden-onset neck pain.
The first time was in the morning, when I wasn’t there to observe it.
The second time, in the evening, I observed it. She was in agony, writhing and sounding as though she were in labor.
So how was this neck pain associated with the burr hole draining of the chronic subdural hematoma, if at all?
Dr. Lee (who was not my mother’s neurosurgeon) says, “Neck pain is not common, but would not be unusual, as headaches can be associated with neck pain frequently.”
One nurse suggested that the way my mother had been positioned on the operating table had caused a muscle to spasm in her neck.
Another nurse suggested that the neck pain was caused by my mother’s ongoing bed rest in virtually the same position.
I didn’t believe these were causes of neck pain that was agonizing enough to make a woman appear that she was in the process of giving birth.
The first nurse then suggested that the neck pain was caused by nerve endings from the brain being fired off from the burr hole draining procedure, and that these nerves extended into the neck.
The neck pain, both times, had been subdued with a hot pack and Vicodin.
Postoperative headaches, then, are to be expected, following burr hole drainage of a chronic subdural hematoma.
But beware if the headaches start becoming worse and more frequent.
This could signal a recurrence of the chronic subdural hematoma (there is a 15 percent recurrence rate).
This happened to my mother; she had a recurrence, and at some point on the headache continuum, the cause of the headaches transformed from postoperative and incisional, to a recurrence of the chronic subdural hematoma.
Ten days after the burr hole drainage, the headache pain was so unbearable that she couldn’t sleep through the night.
A few other new symptoms were present, convincing me she had a recurrence of the chronic subdural hematoma (or, to put it another way, perhaps the burr hole draining wasn’t complete, and residual fluid and leaking continued to build up).

Dr. Lee focuses on minimally invasive techniques to treat traumatic and degenerative diseases of the spine and brain tumors. He’s been invited to speak at the regional and national levels on his research areas.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Chronic Subdural Hematoma Symptoms: How Long Before They Show?
A chronic subdural hematoma is a very slow bleeding in the brain.
Just when you thought you were in the clear for having a brain injury, this kind of bleeding could rear its ugly head.
In fact, a CAT scan taken 24 hours after getting hit in the head may be perfectly normal, and then weeks go by without any problem, and then one day the patient awakens with symptoms: a chronic subdural hematoma is at work.
How Long It Takes for Symptoms of Chronic Subdural Hematoma to Start Showing
I wondered if there was a “grace period” during which the symptoms of chronic subdural hematoma would present, and then if there was a period of time following getting hit in the head, that if a patient still didn’t have symptoms, he could rule out chronic subdural hematoma.
Obviously, the hit that I took on my head two years ago, to this day, has not produced any symptoms.
So I can safely assume that I currently don’t have a chronic subdural hematoma, even though in theory, I could have developed a very small one without symptoms several weeks after the trauma, which resolved on its own.
But is there a grace period?
“There is no good answer for this question, as symptoms will be very dependent on a number of factors such as the age of the patient, variability with the amount of atrophy, the degree/severity of the trauma, history of other risk factors such as anticoagulant use, etc.,” explains Kangmin Daniel Lee, MD, a neurosurgeon with New Jersey Brain and Spine.
Old age is a major risk factor for chronic subdural hematoma, though younger people can get these as a result of blunt trauma to the head.
In fact, young children are more likely to get a chronic subdural hematoma from head trauma than young adults or middle aged adults.
Combine old age with daily use of anticoagulants such as aspirin or Coumadin, and you up the ante for the risk of developing a chronic subdural hematoma if the person hits his head as a result of a slip-and-fall, or bumps his head when getting into a car, or strikes his head on the underside of a table after being on all fours searching for a dropped coin.
“The average length of time between head trauma and presentation to the emergency room is typically one month in the case of chronic subdural hematoma.
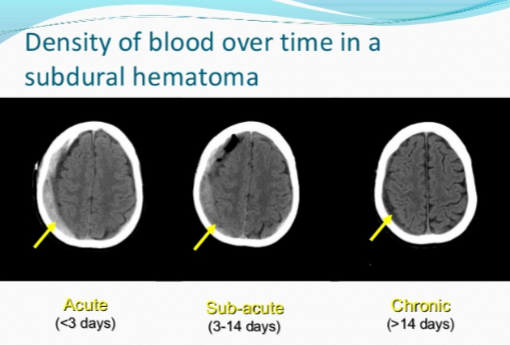
“This is likely due to the slow and progressive nature of symptom onset. The age of the hematoma is easily confirmed by observing the density of the blood on CT scan.”
If you hit your head, or get hit in the head, even if it doesn’t cause immediate symptoms like a headache or dizziness, you still should take note of the date it happened.
The reason is … you may feel fine for several weeks, then awaken one day with out-of-the-blue symptoms, like my mother did:
A headache that she described as feeling like a “crown of thorns” that wouldn’t respond much to painkillers; significant leg weakness (one leg more so than the other) that made it nearly impossible for her to stand up from a chair; and upchucking.
This occurred six weeks after she lost consciousness from a blood pressure drop while standing, and fell dead-weight against the bathtub, striking her head. The diagnosis was a chronic subdural hematoma.
Just one week before the sudden onset of the symptoms, my mother had attended an exercise class and reported that it was too easy for her!
Chronic subdural hematoma is a very stealthy condition, and if symptoms appear, you absolutely must seek medical treatment.
Dr. Lee focuses on minimally invasive techniques to treat traumatic and degenerative diseases of the spine and brain tumors. He’s been invited to speak at the regional and national levels on his research areas.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image credit: James Heilman, MD
Can Chronic Subdural Hematoma with Symptoms Go Away on Its Own?
Burr hole drainage of a chronic subdural hematoma
If a chronic subdural hematoma causes symptoms, does this mean it cannot resolve on its own, without medical treatment?
After all, many elderly people (and younger people who get hit in the head), who don’t have medical coverage, and who develop chronic subdural hematoma, won’t seek medical attention if the symptoms are mild.
Also, in an elderly person, if the symptoms are mild enough, they can be brushed off as a sign of aging, or the result of “working too hard” the day before.
In fact, when my mother awakened with a searing headache (and was later diagnosed with chronic subdural hematoma), my father actually believed that the headache was caused by eye strain from sewing too much the day before!
“It is possible for cSDH to resolve on its own,” says Kangmin Daniel Lee, MD, a neurosurgeon with New Jersey Brain and Spine. (He was not my mother’s surgeon.)
But this refers to chronic subdural hematoma without symptoms.
If a chronic subdural hematoma doesn’t produce symptoms, then how would doctors even know a patient has one in the first place?
It is discovered incidentally on a CAT scan of the head that’s taken for either an unrelated reason; or, a tiny chronic subdural hematoma is discovered in addition to the bigger one that’s causing some symptoms. This was the case with my mother.
She had a CAT scan with contrast dye of her head because the ER doctor suspected a mild stroke.
But then the ER doctor came back and stated, “You didn’t have a stroke. But what we found surprised us. You have bleeding in the brain. Did you fall recently?”
(The fall had been six weeks prior, in which she’d hit her head on the bathtub.)
There were two chronic subdural hematomas in my mother’s brain. One was “large” and the other was “small,” at just four millimeters.
Only the large one was surgically drained (via a 15 minute procedure). We were told that the small one would resolve on its own.
It never produced symptoms (after the surgery my mother didn’t exhibit the profound weakness in her legs that she had that got her the ER visit in the first place).
A follow-up CAT scan verified that the four-millimeter chronic subdural hematoma eventually vanished completely.
So yes, a chronic subdural hematoma without symptoms can resolve on its own.
Dr. Lee says, “This will take weeks to months depending on the volume of blood present.
“However, if the patient is symptomatic from the hematoma, then this usually will indicate that the volume of blood has gotten thick enough to cause mass effect on the brain.”
The term “hematoma” is derived from Latin and translates to “blood mass.”
Dr. Lee continues, “If the volume is large enough to do this, then the likelihood is greater that there will be repeat hemorrhages, causing even more mass effect, which would be dangerous for the patient.
“This is because the hematoma actually pushes the brain away from the skull, stretching the tiny bridging veins and increasing the likelihood of further hemorrhage.
“If the vein bleeds then there is often a snowballing effect making things worse and worse.”
Between the ages of 50 and 80, the brain’s weight decreases on average by 200 grams, says Dr. Lee.
Corresponding to this is an increase in the space between the brain and skull from 6 to 11 percent of the total intracranial space.
These conditions increase the likelihood of chronic subdural hematoma from a fall in the elderly.
 A chronic subdural hematoma typically shows symptoms weeks after the trauma to the head, when head trauma is the cause.
A chronic subdural hematoma typically shows symptoms weeks after the trauma to the head, when head trauma is the cause.
In fact, a CT scan taken 24 hours after getting hit in the head may be perfectly normal.
And then weeks go by without any problem, but then one day the patient awakens with symptoms: a chronic subdural hematoma is at work.
Dr. Lee focuses on minimally invasive techniques to treat traumatic and degenerative diseases of the spine and brain tumors. He’s been invited to speak at the regional and national levels on his research areas.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Chronic Subdural Hematoma Symptoms vs. Stroke

The symptoms of a stroke and a chronic subdural hematoma are strikingly similar — nearly identical — and in some cases ARE dead-on identical, even though the causes of these conditions are quite different.
For this article I consulted with Kangmin Daniel Lee, MD, a neurosurgeon with New Jersey Brain and Spine.
Distinguishing at home the difference between the symptoms of stroke and those of chronic subdural hematoma.
My mother had a chronic subdural hematoma and I thought she’d had a minor stroke. So did the ER doctor after examining her.
In fact, the ER doctor didn’t even offer the differential diagnosis of chronic subdural hematoma.
All I heard was possible stroke. Dr. Lee (who was not my mother’s neurosurgeon) explains:
“There is too much overlapping symptoms with chronic subdural hematoma vs. stroke to be able to reliably diagnose one or the other simply based on clinical presentation.
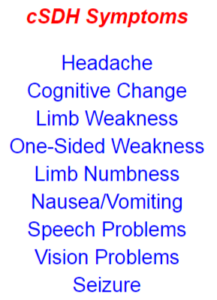
“Most often, patients with chronic subdural hematoma will complain of gait instability, headache, confusion, language difficulty or weakness. These are also common presenting complaints of stroke.”
My mother’s sudden onset of symptoms began early in the morning with a raging headache, and when she got out of bed, it was clear that there was a compromise in her ability to walk.
Though at that time, I passed it off as a side effect from the headache – who wants to march across the room while suffering the meanest headache ever?
But as the morning progressed I clearly observed something not right with my mother’s walking, and what was particularly alarming was that the left leg had a slight drag.
There was profound weakness in her lower body that made it extremely difficult for her to get out of a chair.
Her speech and cognition were normal, but normal speech and cognition don’t rule out a stroke.
Though slurred speech and/or confusion are common symptoms of stroke (and chronic subdural hematoma), the absence of one or both of these does not point more likely to stroke, or more likely to chronic subdural hematoma.
I then wondered about the symptom of sudden-onset double vision, which can occur from a mini-stroke, also known as transient ischemic attack.
Deductively, sudden-onset double vision can also be a symptom of a full-blown stroke.
But can a chronic subdural hematoma cause sudden-onset double vision?
And are there symptoms of a stroke that would never be caused by a chronic subdural hematoma?
Dr. Lee responds, “Unfortunately there really are no clinical symptoms that would necessarily distinguish between the two.
“The clinical symptoms of a stroke are dependent on the clinical function of the brain tissue that is damaged.
“Both present commonly with headache, seizure, weakness, numbness or altered mentation.
“In terms of timing, one could say that stroke is more commonly associated with an acute presentation, while cSDH will generally occur gradually and progressively.”
This is a compelling point, because my mother had two incidents of chronic subdural hematoma:
1) sudden onset of symptoms six weeks after hitting her head, and
2) 10 days after drainage of this cSDH, her left hand began losing function, and marginally altered mentation began setting in – both in a subtle way – and both caused by a recurrence of the original chronic subdural hematoma (there is a 15 percent recurrence rate).
There was nothing “acute” about this second set of symptoms.
There was a progressive component; each day the left hand got worse, and each day the headaches got worse and more prolonged.
Stroke was the fartherest thing from my mind, based on my mother’s very recent history of chronic subdural hematoma, and the progressive nature of her new symptoms.
But note that Dr. Lee says: “However, this is not a hard and fast rule, as chronic subdural hematoma can also cause acute symptoms such as altered mentation or weakness.”
The first incident of chronic subdural hematoma in my mother, as mentioned already, were acute in that in the weeks prior, she was doing great, zipping all over the place at stores, and the night prior to her awakening with a headache that was bad enough to bring her to tears, she was completely normal.
Next morning, bam! Disabling headache pain along with severe lower body weakness.
The only way to differentiate between stroke and chronic subdural hematoma, regardless of symptoms, is with a CT scan of the brain.
Don’t assume that someone’s symptoms must mean chronic subdural hematoma just because he hit his head recently, either; it can still be a stroke, unrelated to the head trauma.
Dr. Lee focuses on minimally invasive techniques to treat traumatic and degenerative diseases of the spine and brain tumors. He’s been invited to speak at the regional and national levels on his research areas.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock
Signs of Chronic Subdural Hematoma Recurrence

You may need to really be on the ball to catch the early symptoms or signs of a recurring chronic subdural hematoma.
These new-onset symptoms won’t necessarily be the same as the original ones. The recurrence rate is 5 to 33%.
My senior-aged mother developed a chronic subdural hematoma.
“A chronic subdural hematoma occurs when blood collects on the surface of the brain beneath the dura, which is the covering of the brain,” says Dr. David Beatty, MD, a retired general practitioner with 30+ years of experience and an instructor of general medicine for 20+ years.
“Rupture of cortical bridging veins occurs. These veins connect the venous system of the brain to the intra-dural venous sinus.
“Sometimes there is a history of head trauma, but this is often only a minor knock which may have happened days or weeks earlier.
“In about 50% there is no recollection of head injury.”
Six weeks prior to the first symptom of my mother’s cSDH, she had lost consciousness due to orthostatic hypotension, fell and hit her head on a bathtub. At the time she was on Coumadin, a blood thinner.
She stopped the Coumadin 12 days later due to the fall risk of orthostatic hypotension, but continued on daily aspirin for recent coronary bypass surgery.
Thus, the neurosurgeon (after cSDH diagnosis) was not able to pin down the cause of the chronic subdural hematoma.
Six Weeks After the Fall
One morning she awakened around 7 am with a splitting headache that made her weep and unable to function. It persisted for three hours until painkillers finally subdued it.
Her walking was very feeble, and she also upchucked.
With difficulty she made her way down the stairs and sat in a chair, reporting that the headache was gone. But she had extreme difficulty rising from the chair.
She was not able to walk normally; was weak and very tired. Her left leg slightly dragged behind the right.
All these symptoms suggested a mild stroke, but at the ER she was diagnosed with chronic subdural hematoma.
Ten days after a burr hole craniotomy was the first time that a definitive new symptom appeared, though at the time, I didn’t think this was a recurrence of the chronic subdural hematoma.
About nine or ten days after the burr hole procedure, I noticed that my mother seemed marginally foggy, but chalked it up to just overall general recovery, and a very recent adverse reaction to an anti-seizure drug, Keppra, that was prescribed for the chronic subdural hematoma.
She had been regaining her strength after the adverse drug reaction, but then seemed to be regressing as far as energy.
Since the surgery my mother had complained of headaches, but they weren’t bad enough to alarm me; I thought they were post-surgical, or related to the incision.
New Symptoms
But ten days after surgery I began noticing some quirky mental things.
Then she began dropping things by accident. Ultimately it was determined that the dropping was coming from her left hand.
She was not able to touch her left index finger to her nose with eyes closed. That’s when I knew there had to be a recurrence of the chronic subdural hematoma.
Also, over the past several days her headaches had increased in frequency and intensity, to the point where she’d moan and groan.
I got ahold of the neurosurgeon and reported loss of fine motor control in my mother’s left hand.
She struggled to pick up a straw, dropped cups of juice and a bowl of potato chips, dropped her glasses and accidentally stepped on them and didn’t realize it, and dropped other items like a roll of masking tape, the TV remote and some mail.
The neurosurgeon wasn’t concerned and never suggested this might be a recurrence of the chronic subdural hematoma!
One mental incident stood out. She had a few pills in her left hand, about to take them, then suddenly went to a chair and lifted a magazine off it with her right hand, then placed the magazine back down, pills still in left hand. I asked why she did that.
She said, “I’m looking for my pills.” Then she realized they were in her left hand.
Overnight she was awake most of the time, loudly groaning from headache pain.
At 7 am she was stuttering, speech mildly slurred, or, to put another way, lacking its usual crystal clarity, and her mentation was altered (e.g., kept insisting, and trying, to go upstairs to sleep despite having to get ready for an appointment with the neurosurgeon).
We were running behind schedule, yet she insisted on using her impaired left hand to lift a glass bottle of juice from the top shelf of the refrigerator. I had to remove the bottle from her flaccid hand.
She then wanted to make up her face, despite my protests that we were going to be late, and she didn’t seem to notice she was repeatedly dropping things in the bathroom.
I finally had to place my hands on her and make her walk into the garage.
Ultimately, she was diagnosed with a recurrence of the chronic subdural hematoma.
As you can see, the symptoms the second time around were different than the first time, save for the headache.
 Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for
Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for 

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}