

TIA Symptom: Body Pulling to One Side?

If your body suddenly feels like it wants to pull or veer to one side, could this mean a transient ischemic attack?
If you’ve recently experienced the sensation that your body was pulling to one side, do not blow off such a symptom.
“Sensation of body ‘wanting to go one side’ can be interpreted as veering to one side while walking, very likely might be a TIA,” says Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
Think of it this way: What else could explain such an oddball sensation?
You may be wondering, what is it about a transient ischemic attack that would cause you to feel as though your body was wanting to pull to one side?
The TIA could be cutting off blood flow to the part of the brain that controls that side of the body, making motor control and sensory perception impaired.
What you might actually be experiencing is a heaviness on one side, and if one side of your body feels or seems heavier than the other, it will seem like it’s being pulled in that direction.
“The manifestation of TIA can be protean [extremely variable], and the symptoms of TIA are as many as there are brain functions,” says Dr. Mikolaenko.
“But typically TIA symptoms will point to a specific brain region or its vascular territory.
“Veering to one side or another might be due to cerebellar dysfunction, and vertebro-basilar TIA should be thought of.”
If you’re suddenly overcome with the feeling that your body is being pulled to one side, or feels heavy or numb on one side — have someone immediately drive you to the ER, especially if you have risk factors for a TIA or stroke:
Over Age 50
Don’t Work Out; Sedentary Lifestyle
Obese
Diet High in Processed Foods
Smoker
Family History of Stroke
Diabetes
Poor Cholesterol Profile
Diagnosis of Atrial Fibrillation
TIA Is a Warning a Stroke May Be Coming
You have to wonder how many people who’ve suffered from a massive stroke — in the few months prior to it — had had a TIA but didn’t inform anyone about it.
Perhaps they didn’t even know they were having a TIA and attributed the odd sensation of being pulled to one side as anxiety related or maybe due to lack of sleep or having had too much to drink the day before.
Or maybe they wanted to mention the symptom, but at the time, nobody was around, and they simply forgot about it.
A TIA is a significant risk factor for a future stroke, and it serves as an alert that the individual’s vascular health needs immediate attention.
Awareness campaigns for stroke (symptoms are the same as a TIA) focus on only a handful of sudden signs: sudden weakness or paralysis on one side; clumsiness; facial drooping; speech difficulty; trouble with vision; mental confusion.
We often don’t hear about the more unusual symptoms such as the feeling that your body is being pulled to one side, feeling that one side of your body is suddenly heavy or difficulty swallowing.
Any sudden changes as described above warrant prompt medical attention.

Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Depositphotos

Can a Recent Transient Ischemic Attack Be Detected on Exam?

Is there a special test that can tell if you just had a transient ischemic attack?
A TIA (transient ischemic attack) is a mini stroke — and even though the symptoms may vanish after only 30 seconds, a TIA is a medical emergency because it shows that the patient is at very high risk for a massive stroke.
And in case you don’t already know, stroke is the leading cause of disability in the U.S. And it doesn’t just strike senior citizens.
Smoking and high blood pressure are key risk factors for a mini stroke or TIA. So are obesity and lack of exercise.
Out of these four risk factors for a transient ischemic attack, only one involves body weight. So don’t think you’re in the clear just because you’re thin.
Certainly, there exists a test that can tell if someone had a TIA, right?
Well, unfortunately, no such test exists.
“All of the tests that a patient with suspected transient ischemic attack will have ordered have two main goals: substantiate the diagnosis of brain ischemia and establish the cause of brain ischemia,” says Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
What is ischemia?
Ischemia refers to interrupted oxygen supply due to impaired blood flow.
In the case of a mini stroke (or stroke), the cause would be a blood clot.
The clot may originate in the brain, or it may come from the carotid artery in the neck, which carries blood to the brain.
The clot can also originate in the heart. It travels up the aorta and into the carotid artery and to the brain where it lodges in a tiny vessel, obstructing oxygen to the area of the brain that the vessel feeds.
Clues to a Transient Ischemic Attack
“General chemistry labs might detect metabolic abnormalities leading to stroke imitation,” says Dr. Mikolaenko.
“Abnormal blood count and specific blood antibodies may provide useful clues to blood rheology [pertaining to the flow of blood matter] or increased blood-clot forming.”
In short, it may be many years before a single test can identify a TIA with 100 percent accuracy.
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Roman Zaiets

Single Symptom TIA vs. Multi-Symptom

If you think a TIA that causes only one symptom isn’t as serious as a multi-symptom transient ischemic attack, you’re in for a shock.
Suppose you have sudden-onset blurry vision but no other symptoms, and you suppose this was a transient ischemic attack, but then you figure, “Oh, can’t be serious; it was only one symptom.”
“Single TIA symptom might be as serious as multi-symptoms,” says Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
“We, vascular neurologists, sometimes rate the clinical picture into ‘hard’ and ‘soft’ symptoms of TIA.
“The hard ones usually are problems with language (aphasia), one-sided weakness (hemiparesis) or loss of vision in one eye (monocular blindness).
“But many patients might have mild headache (cephalgia), dizziness (vertigo or lightheadedness), confusion, blurry vision, which very often will be ignored or pointed as not feeling well.”
These sensations may also be brushed off as side effects of medication.
Dr. Mikolaenko refers to the mild headache, dizziness, confusion and blurry vision as soft signs of a TIA, “and such transient symptoms require careful neurologic evaluation, particularly if they occur in the right context.
“It is believed that TIAs are warning signs of stroke, especially those associated with weakness and speech impairment.
“Patients who experience only isolated sensory symptoms [such as dizziness, slight headache, double vision] that resolve within 10 minutes are at risk of recurrent TIAs but rarely for the full-blown stroke.”
This doesn’t get you off the hook. If you have a “soft” TIA sign while driving, you’ll likely lose control of the car.
A soft symptom even while standing could result in a hard fall to the floor, causing a serious injury such as a brain bleed.
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/LightField Studios

Can a Doctor Tell if You Had a TIA By Looking into the Eyes?

A transient ischemic attack (mini-stroke) is a scary thing, and a doctor will use a special instrument to peer into the patient’s eyes.
This will help the physician, giving information or clues to see if there are any possible signs of a recent TIA.
How well can a physician spot evidence of a TIA by checking the eyes?
The doctor uses an instrument called an ophthalmoscope.
“So-called funduscopic exam of the deep structures of the eye, particularly the retina and its vessels, might pinpoint towards signs of a TIA, especially if retinal vasculature abnormalities are detected,” explains Ivan Mikolaenko, MD, a board certified neurologist of 20+ years based in New York with subspecialty certification in neurocritical care.
However, if this exam turns up nothing, this does not rule out a TIA!
It’s impossible for a doctor to know that you did NOT have a transient ischemic attack if the view of the deep structures of the eyes turned up normal.
In other words, this exam is very meaningful if something does indeed turn up, but it means nothing if the result is negative. Many transient ischemic attacks will not appear on the funduscopic exam.
What to Do if You suspect a TIA and the Eye Exam Is Normal
Ask your doctor what the next step should be, even if he says everything looks fine.
By definition, a TIA is temporary. So just because you feel normal sitting there in the doctor’s office, and whatever odd symptoms you had are long gone, doesn’t mean that you did not have a blood clot in your brain.
Your doctor should have your complete medical history and use that, along with other tests, to determine your risk factors for a miniature stroke.
Certainly, the index for suspicion of a transient ischemic attack will be a lot higher in a 50-year-old smoker who has borderline hypertension, than in a 25-year-old nonsmoker with low-range blood pressure.
Conditions treated by Dr. Mikolaenko in the intensive care setting include strokes, ruptured aneurysms, trauma-related brain and spinal cord injuries, seizures and brain swelling, infections and tumors.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Miriam Doerr Martin Frommherz
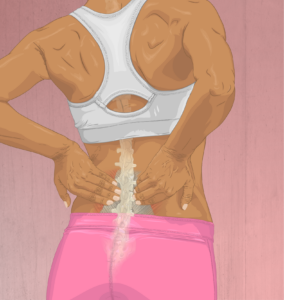
When Is Surgery Needed for a Lumbar Herniated Disc?
What is the point at which it’s time to seriously consider surgery to remedy a herniated disc in the low back?
“Learning to live with the pain” is the mantra heard by many people who have a herniated (bulging) disc.
This is also sometimes referred to as a pinched nerve by laypeople.
But it’s all the same deal, regardless of name: a compression of a nerve at the lumbar spinal column.
The resulting pain may be local or radiate out somewhat, sometimes extending down the leg.
Though the leg is affected in these cases, it’s not because of a muscle problem. It’s because of the nerve in the leg that originates in the spinal cord — where the site of compression is.
For a while patients will try to manage the low back (or leg) pain via conservative means, wondering for how long they can hold off on surgery before the pain becomes impossible to live with.
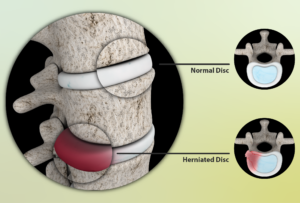
Source: myupchar. com
When Is Surgery Needed for a Herniated Disc?
“Surgery would be indicated for lumbar herniated disc when a patient is noticing a progressive loss of strength in the leg; we term that partial paralysis,” says Dr. P. Justin Tortolani, an orthopedic surgeon and spine specialist with University of Maryland St. Joseph Medical Center.
“Another indication is when there is pain that is not retractable; when nothing tried is helping,” continues Dr. Tortolani.
This would include a failure of “steroid injection, acupuncture and just the tincture of time.”
A herniated disc can cause shooting, stabbing but brief episodes of pain that can literally stop a person in their tracks.
There may be numbness and tingling. Sitting in the same position for long periods, with pressure on the hamstring (back of the upper leg) can bring on numbness and tingling.
This may often occur as a result of sitting on a toilet seat for an extended period.
 Dr. Tortolani’s vast experience includes treating all disorders of the spine including herniated discs, spinal stenosis, and adult and adolescent scoliosis.
Dr. Tortolani’s vast experience includes treating all disorders of the spine including herniated discs, spinal stenosis, and adult and adolescent scoliosis.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Can a Bulging Disc Be Untreatable?

Find out from a doctor if a low back herniated (bulging) disc can be untreatable.
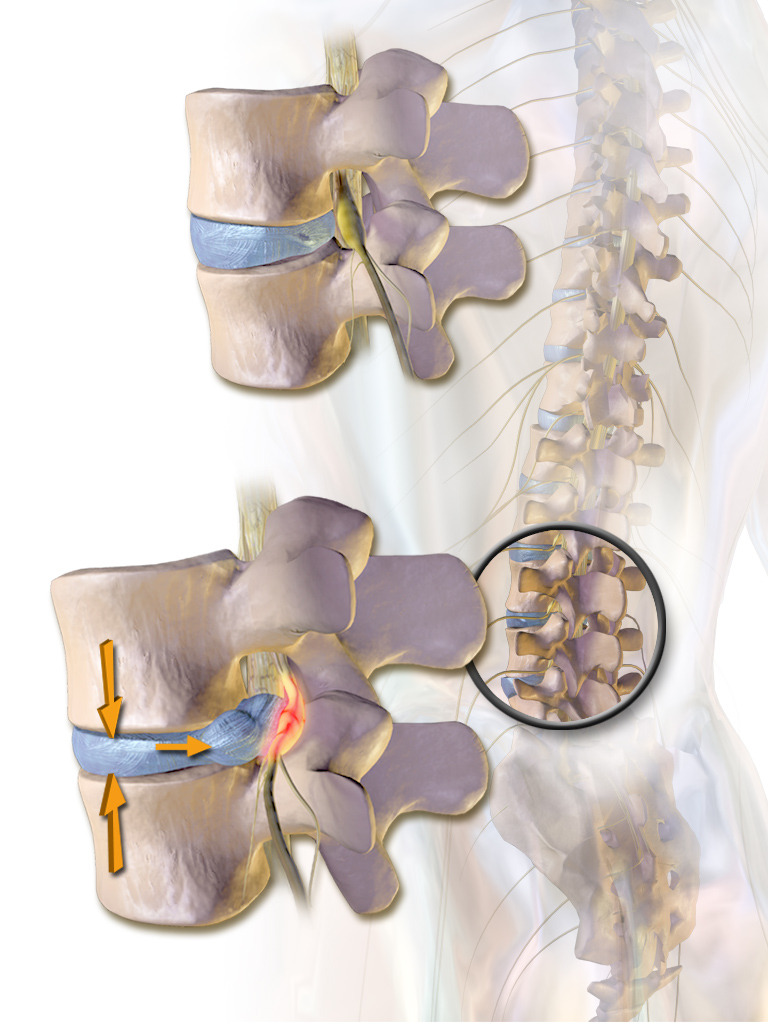
A bulging disc puts pressure on nerves that come out of the spinal cord.
A bulging disc occurs when the soft, gel-like center of a spinal disc pushes through its outer layer, potentially compressing nearby nerves.
This pressure on the nerves can cause symptoms such as pain, numbness or weakness in the affected area, often radiating to the arms or legs depending on the location of the disc.
Even a foot can be affected by pain, numbness and/or tingling.
Typically, conservative (nonsurgical) treatments are tried first.
These include physical therapy, hot packs, ice packs, massage and painkilling drugs.
But some people also undergo surgery when all else has failed for their bulging disc.
The very vast majority of herniated disc cases are treatable.
Treatments for a Bulging Disc
This is a condition in which the conservative approach (e.g., physical therapy, back supports for chairs, NSAIDs) wins hands-down over surgery.
Just because you have an issue with your spine, doesn’t mean you automatically need surgery.
Surgery in the case of a bulging disc should always be a last resort, when all else has failed.
When is a herniated disc untreatable?
“Very rarely would it be untreatable unless the patient had some medical factors in which surgery couldn’t be performed like severe heart disease,” says Dr. P. Justin Tortolani, an orthopedic surgeon and spine specialist with University of Maryland St. Joseph Medical Center.
“I’ve never had a patient come in with a herniated disc that couldn’t be treated, but I had one with nerve compression in the lower back, where their heart was so sick their doctors wouldn’t let them go through general anesthesia.”
When a patient feels that they have tried every conservative option yet the pain is still disruptive to their life, they have to ask themselves if they truly, faithfully have given physical therapy a fair chance.
It’s not unheard of for patients to prematurely give up on physical therapy due to either some degree of pain during the movements or assuming ahead of time that PT just won’t work — and hence, not trying it or skipping sessions. They then create a self-fulfilling prophecy.
The person with a herniated or bulging disc needs to give all nonsurgical treatments a fair shake before deciding that the case is hopeless without surgery.
Dr. Tortolani’s vast experience includes treating all disorders of the spine including herniated discs, spinal stenosis, and adult and adolescent scoliosis.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: BruceBlaus/CreativeCommons

Herniated Disc Surgery: What’s Involved

Find out what’s involved in surgery to treat a herniated (bulging) disc.
A herniated disc is common in the general population, but not all cases produce symptoms.
When symptoms do develop, they include the following:
- Pain in the lower back
- Pain that radiates down the butt and may extend down the leg
- Tingling or numbness in any of these areas
- Weakness in the leg and even the foot
There are numerous non-surgical treatments for a herniated disc. These are tried first before it becomes clear that surgery is the only option left.
These include physical therapy, stretching exercises, warm packs, cold packs, chiropractic, acupuncture, muscle relaxants, pain relievers and epidural steroid injections.
Surgery is often an anxiety-driving prospect, but when conservative treatments fail after being given a fair time trial, then a microdiscectomy is the only recourse.
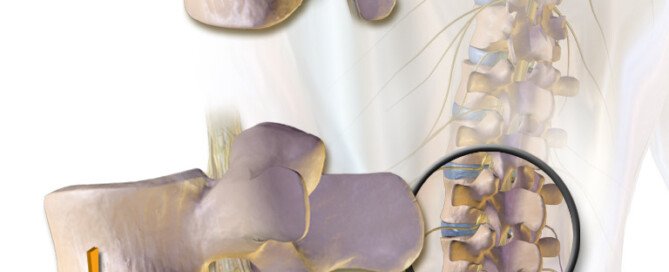
Surgical Repair of a Herniated Disc
“What we’re doing is called a microdiscectomy and it takes about 45 minutes to an hour to perform,” says Dr. P. Justin Tortolani, an orthopedic surgeon and spine specialist with University of Maryland St. Joseph Medical Center.
General anesthesia is used to guarantee that the patient will not make even the slightest movement during the procedure.
“It’s accomplished through a small incision and generally, patients are discharged the same day with a two to three week recovery period. Their daily activities are restricted somewhat,” says Dr. Tortolani.
“Specifically, what is done is to create a small window opening in the spinal column and that’s called foraminotomy, and then after that the portion that is herniated is removed or excised.
“Usually we’re not touching the remainder of the disc itself and just removing the portion that is herniated.”
Dr. Tortolani’s vast experience includes treating all disorders of the spine including herniated discs, spinal stenosis, and adult and adolescent scoliosis.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Monkey Business Images

Causes of Chest Pain, Jaw Pressure in Middle of the Night

A cardiologist names some likely causes for chest pain and jaw pressure in the middle of the night.
The cause of pain in your chest or pressure in your jaw that awakens you in the middle of the night isn’t necessarily a heart attack.
“There are many possible causes,” says Dr. Sameer Sayeed, a cardiologist at ColumbiaDoctors of Somers, NY.
Angina As a Cause
“Cardiac causes can include coronary artery disease with rest angina, especially in those with lower heart rates at night,” says Dr. Sayeed.
Coronary artery disease means plaque buildup in the arteries. This so-called sludge reduces blood flow through the heart.
Angina is a condition in which clogged coronary arteries lead to this reduced blood flow in the cardiac muscle, causing chest pain and/or shortness of breath.
When this occurs only upon physical exertion, exercise or highly charged emotions such as during a heated argument, it’s called stable angina. Jaw pressure may occur.
When it occurs during rest, such as during sleep or napping, it is called unstable angina. Here too, pressure in the jaw may occur.
Leaky Heart Valve As a Cause
Another cause of chest pain overnight that’s accompanied by jaw pressure is leaky valves in the heart.
An echocardiogram will detect if this is the case. Leaky valves as well can decrease cardiac blood flow.
Inflammation As a Cause
“Another cause can be pericarditis and inflammation of the sac around the heart, and pericardial effusion or fluid around the heart, which can be worse with lying down and flat, and can wake people up at night with chest pain,” explains Dr. Sayeed.
“This kind of pain can also occur in the setting of pulmonary embolus or blood clot in the lung. But the most common cause would be coronary disease with low flow as above.”

Dr. Sayeed performs echocardiograms and stress tests at the Midtown Manhattan and Westchester offices at Columbia Doctors. He is also trained in cardiac CT imaging.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/airdone

Best Exercises for a Low Back Herniated Disc

Here is what a pain specialist doctor recommends as best exercises for a herniated disc in the low back (lumbar region).
A herniated disc in the low back (lumbar spine) is very common, and also goes by the name of bulging disc.
The first line of treatment involves exercises. They are really quite simple; nothing complicated or difficult to do, no matter how “lazy” or “out of shape” you think you are.
What are the best exercises for treatment of a herniated disc in the low back?
Source: myupchar. com
The two types of exercises are Pilates and walking, says Neil B. Kirschen, MD, chief of pain management, Department of Anesthesiology at South Nassau Communities Hospital in Oceanside, New York.
If you use a treadmill do not hold on other than for momentary steadiness such as when drinking some water.
Holding on as part of your walking will disrupt natural gait patterns and will often cause poor posture.
These are the last things you need when you have a back problem.
Walking sessions done consistently strengthen the muscles that support the spine, which can alleviate pressure on the back and improve posture.
Walking encourages the release of endorphins, which are natural pain relievers.
It can also help maintain a healthy weight, reducing the strain on the back caused by excess body weight.
Unlike high-impact exercises, walking is gentle on the joints and minimizes the risk of exacerbating back pain.
Beginning with short, manageable walks and gradually increasing duration can be beneficial for those with back pain from disc herniation.
Pilates focuses on core strength, flexibility and overall body alignment.
By emphasizing controlled movements and proper breathing, Pilates helps strengthen the muscles that support the spine, including the abdominal, back and pelvic muscles.
This core strengthening enhances spinal stability and can reduce the strain on the back.
Pilates exercises promote flexibility and improve posture, which can help relieve pressure on the spine and reduce discomfort.
The emphasis on precise movements and proper alignment helps correct muscle imbalances and misalignments that may contribute to back pain.
What about yoga and stretching?
You do not need to be able to bend like a pretzel to do yoga.
There are basic poses, and even the difficult poses have beginner’s variations.


Shutterstock/Maridav
Dr. Kirschen also says, “Lying on back with legs elevated on a stack of shelves, gradually lowering the legs on each shelf until flat on the ground.”
He really stresses stretching, however, as a major component in pain relief.
He also emphasizes “Including pelvic tilts [below] and basic calisthenics we used to practice in gym class — the more you do this movement, the better it will feel.

Shutterstock/Mangostar
All in all, what is the most effective treatment for lower back disc herniation?
Dr. Kirschen also recommends the “application of moist or dry heat along the lumbar spine.”
Dr. Kirschen says that the “best treatments for acute and sub-acute pain from disc herniation are the epidural steroid injections and performance of acupuncture.”
 Dr. Kirschen is board certified in anesthesiology, pain medicine, acupuncture and massage therapy, and has extensive postgraduate training in osteopathic and manual medicine.
Dr. Kirschen is board certified in anesthesiology, pain medicine, acupuncture and massage therapy, and has extensive postgraduate training in osteopathic and manual medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/tommaso79

About this Site
Knowledge Is Power

Founded in 2012, Scarysymptoms.com has established itself as a leader for providing visitors in-depth information about their symptoms — not the template information of most other medical sites, but information straight from interviewed doctors that digs very deep into the issue.
What sets Scarysymptoms.com apart from the rest?
Most of the information here comes straight from interviewed physicians and other medical professionals who give detailed explanations that go beyond the generic, recycled symptom information found on other medical sites.
The expert sources for Scarysymptoms.com are respected and credible leaders in their medical field.
Furthermore, there is considerable content based on the firsthand caregiving experience of Scarysymptom.com’s founder, Lorra Garrick, regarding the following medical conditions that have affected her parents:
• Quintuple bypass surgery
• Mitral valve replacement
• Pacemaker implant
• Congestive/chronic heart failure
• Two total knee replacements
• One knee revision surgery
• Two total hip replacements
• Chronic subdural hematoma
• Two brain surgeries
• Three back surgeries
• Three shoulder surgeries
• Knee arthroscopy
• Herniated disc/sciatica
• Double carpal tunnel syndrome/surgery
• Pneumonia
• Low thyroid
• Clinical depression
• Peripheral neuropathy
• Diverticulitis
• Side effects from medications
• Mobility issues
In addition, Lorra writes about her own experiences with the following:
• Changing moles and mole removal
• Seborrheic keratosis
• Seborrheic dermatitis
• Finger pain/cramp (annular flexor pulley injury)
• Shoulder pain (rotator cuff injury)
• Biceps tendonitis
• Low backache
• Heel pain/burning heels (plantar fasciitis)
• Chondromalacia patella
• Quadriceps tendonitis
• Sudden-onset diarrhea (microscopic colitis)
• Change in stool caliber/color (microscopic colitis)
• Missed periods
• Headaches
• Sudden-onset dry mouth
• Continuous coughing (acid reflux)
• Beeturia
• Medial epichondylitis (golfer’s elbow)
• Hamstring injury
• Clicking jaw
• Blocked ears upon awakening
• Ganglion cyst
• Sprained ankle
• Sprained wrist
• PVCs
• Twitching muscles
• Panic attacks
• Actinic keratosis
• Benign paroxysmal positional vertigo
• Prophylactic double mastectomy (sister diagnosed with breast cancer)
• Broken collarbone
• ASD-1
Scarysymptoms.com, then, provides content that burrows deep into all facets of symptoms, from both the professional perspectives of esteemed physicians and also from a prolific writer who has been passionate since high school about health, fitness and strength.
Let’s put it this way: If you want to know the symptoms of colon cancer, any medical site will list these.
But if you want to know just what exactly “constipation alternating with diarrhea” actually means (and this symptom is definitely open to subjective interpretation), Scarysymptom.com covers it.
And if all the melanoma pamphlets and online guidelines say to look out for moles that are at least the size of a pencil eraser…does this mean that a one-millimeter spot can’t be melanoma?
And just why do ALS sites appear on the first page of a search for “cause of muscle twitching”?
Scarysymptoms.com picks up where all the pamphlet-type information of other medical sites leaves off.
The Autistic Advantage

In spring of 2022, Lorra received a clinical diagnosis that for some time, she’d been strongly suspecting she had. It was Autism Spectrum Disorder.
Having an Autistic brain enables Lorra to take deep dives into many medical topics of interest and dig hard right down to the bottom to present all the details, all the possibilities and variations, every single hypothetical and every potential aspect of a condition, symptom or set of symptoms to readers.
And she never tires of this venture, since Autism brings with it the capacity for sustained, deep, complex thinking and concentration on highly specific topics, and the ability to creatively and analogously present explanations in a way that’s easily understandable — yet brimming with all the details that readers seek.
Being on the Spectrum means that thinking outside the box comes easily to Lorra when developing content ideas and presenting subject matter.
Physical Fitness Aspect
Scarysymptoms.com also covers all aspects of fitness, exercise and weight loss.
After all, struggling to burn stubborn fat is a worrisome symptom for many men and women. So is failure to build muscle or gain more strength.
Lorra’s background as an ACE certified personal trainer, plus her own experience with strength training, powerlifting, interval training and injury recovery, have been converted to electrifying content that will empower anyone, be they a 90 pound weakling, someone who is very self-conscious due to obesity, a middle-ager with an expanding waistline or a senior-age person who has never exercised before.
Targeted Audience
• Men and women of all backgrounds, ages and lifestyle habits who want to know more about their symptoms or those of a loved-one without getting confused by conflicting, generic or vague information.
• Those who are simply annoyed by a symptom.
• Those who are worried sick over a symptom.
• People who have developed a fear of having a potentially fatal condition after googling what seems to be a minor symptom.
• Anyone who wants to lose fat, build muscle, sculpt their physique, run faster, lift heavier and live longer, plus improve their self-esteem and mental health.
The purpose of this site is to provide answers—from doctors with whom Lorra has personally corresponded with as a medical writer—to all the possible questions you may have about:
• Symptoms: alarming ones that mean nothing or that may mean danger
• Symptoms: minor ones that may mean a life threatening illness
• Differential diagnoses
• Misdiagnoses
• When to see a doctor and what kind of doctor
In addition, Scarysymptoms.com includes articles written by medical doctors and other medical professionals, plus articles by people who’ve experienced firsthand the condition they’ve written about.
*****
Lorra’s feature articles have appeared in the following print publications (below):
Abilities Magazine
ACE Certified News
American Institute for Cancer Research newsletter
Anchor Magazine
Blackbelt
Exercise for Men Only
Fitness & Physique Magazine
MAMM
Ms. Fitness
Natural Bodybuilding
OnFitness Magazine
Personal Fitness Professional
Taekwon Do Times
Today’s Latino Magazine
Vibrant Life
Images of Some Print Publications


Online publications include:
- Blackdoctor.org
- Howtobefit.com
- Verywellfit.com
Amazon Kindle Publications
- Crucify Fat with HIIT Workouts!
- Fitness Walking the Right Way for Fat Loss
- Maximum Fat Burn with Hormonal Walking
- Top 10 Worst Weight Exercises for the Rotator Cuff
- Shed Belly Fat and Get Ripped Abs
Lorra Garrick


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}