

Prediction of Chronic Subdural Hematoma: Symptoms After Fall?

Find out if neurological symptoms at time of head trauma that soon vanish are predictive of chronic subdural hematoma even with normal CT.
Is a person more likely to develop a chronic subdural hematoma if, at the time of getting hit in the head, they have neurological symptoms, even if the symptoms dissipate soon after?
“Some patients strike their head and do not remember the fall, so it is hard to obtain a history in those patients,” begins John M. Abrahams, MD, chief of neurosurgery at Northern Westchester Hospital, and founder of the Westchester Neuroscience Research Foundation which is studying the genomic profile of malignant brain tumors.
“The stronger the ‘hit,’ the greater the chance of developing a chronic subdural hematoma,” he continues.
“Another predisposing factor is the use of blood thinners.
“Some patients are on these medications for other medical conditions and each has an increased risk for brain bleeding with general use.
“The symptoms can be helpful in terms of predictive value, but not every mild-to-moderate concussion patient does not develop a hemorrhage.”
 Dr. Abrahams is a highly regarded, board certified neurosurgeon who specializes in the treatment of complex disorders of the brain and spine.
Dr. Abrahams is a highly regarded, board certified neurosurgeon who specializes in the treatment of complex disorders of the brain and spine.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ michaelheim

Elderly on Coumadin, Hits Head: Subdural Hematoma Risk?

Learn more about the odds of an elderly patient on Coumadin developing chronic subdural hematoma after hitting their head.
It’s not a pretty trio:
1) Coumadin therapy
2) Getting hit in the head
3) Elderly age. After all, this is a significant threesome in terms of risk of chronic subdural hematoma.
Suppose you have an elderly relative who’s on Coumadin (an anticoagulant), and this individual falls and hits their head.
A CT scan soon after would be a smart idea, even if the patient is lucid.
Most elderly people in this situation will not develop a chronic subdural hematoma, but the number who will carries statistical significance.
“Anticoagulation to conventional intensities increases the risk of intracranial hemorrhage 7- to 10-fold, to an absolute rate of nearly 1%/year for many patients,” says John M. Abrahams, MD, chief of neurosurgery at Northern Westchester Hospital, and founder of the Westchester Neuroscience Research Foundation which is studying the genomic profile of malignant brain tumors.
“Most (70%) anticoagulant-related intracranial hemorrhages are intracerebral hematomas (approximately 60% are fatal),” says Dr. Abrahams. This is bleeding inside the brain.
“The bulk of the remainder are subdural hematomas,” says Dr. Abrahams.
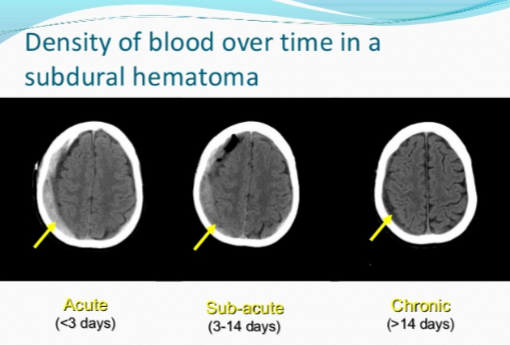
The bleeding of a subdural hematoma, including chronic, occurs between the brain and the tissue that’s one layer above it, called the dura (“sub” means beneath). The tissue between the brain and dura is called arachnoid.
“Predictors of anticoagulant-related intracerebral hematoma are advanced patient age, prior ischemic stroke, hypertension and intensity of anticoagulation,” he continues.
“In approximately half of anticoagulated elderly] patients with intracerebral hematoma, the bleeding evolves slowly over 12 to 24 hours, and emergency reversal of anticoagulation is crucial.”
If the elderly patient has symptoms immediately following the head trauma, is this predictive of a chronic subdural hematoma?
“If the patient has symptoms right after the fall, then they have a greater than a 50% chance of developing a real intracranial hemorrhage of some sort,” says Dr. Abrahams.
What if the symptoms go away fairly quickly?
“If the symptoms dissipate in an hour, then they are probably fine.”
Even two hours means they’ll likely not develop complications down the road.
Is location of the “bump” on the head predictive of a cSDH?
“Location can indicate where the headache may arise, but only in some patients, and is not a clear indicator.”
Dr. Abrahams is a highly regarded, board certified neurosurgeon who specializes in the treatment of complex disorders of the brain and spine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Photographee.eu

Percent of People with Normal Head CT Who Develop Brain Bleed

A neurosurgeon answers the question of what percent of people with a normal CT scan after hitting their head develop a chronic subdural hematoma.
Out of all the people who have a normal CT scan of their brain after experiencing a hit to their head or a fall, a certain percentage will go on to develop a chronic subdural hematoma.
A subdural hematoma of the chronic type means that the bleeding is occurring at a slow rate over time.
The symptoms begin anywhere from three weeks to three months out from the initial head trauma.
The blood leaks from tears in the tiny veins underneath the dura mater of the brain.
How many with a chronic subdural hematoma initially had a normal head CT?
“The number of people who strike their heads is difficult to quantify,” says John M. Abrahams, MD, chief of neurosurgery at Northern Westchester Hospital, and founder of the Westchester Neuroscience Research Foundation which is studying the genomic profile of malignant brain tumors.
“Overall, most patients who develop chronic subdural hematoma did not have an incidental CT scan at the time of the fall.
“In general, the number of patients who fall and develop chronic subdural hematoma is quite small, probably on the order of less than 1%.”
This percent figure will differ if specific age brackets are explored.
For instance, more people over age 70 with an initial normal head CT will go on to be diagnosed with a chronic subdural hematoma, when compared to those age 40 to 50.
Being over the age of 65 is a risk factor for one of these brain bleeds.
That’s because of age-related brain atrophy (shrinkage), which stretches the bridging veins, making them more prone to tearing.
Even minor head trauma can lead to bleeding in this population.
Additionally, older adults are more likely to use anticoagulant or antiplatelet medications (blood thinners), which impair blood clotting and increase the likelihood and severity of bleeding within the subdural space.
Some cases of cSDH in the elderly have no known associated head trauma or fall, and may arise simply from a combination of age-related brain shrinkage and anticoagulation therapy (like a daily aspirin or Coumadin).
Dr. Abrahams is a highly regarded, board certified neurosurgeon who specializes in the treatment of complex disorders of the brain and spine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/uzhursky
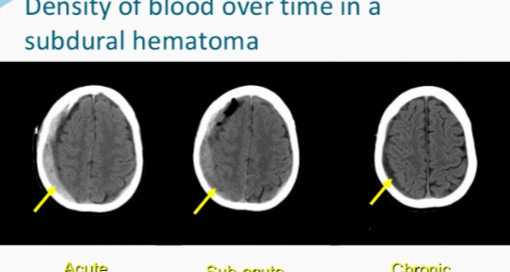
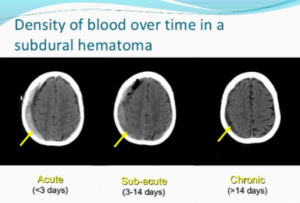
Time of Day Chronic Subdural Hematoma Symptoms Usually Start?
Is there a time of day that symptoms of chronic subdural hematoma typically begin?
You may be wondering if there’s a particular time of day that a person, who’s destined to develop a chronic subdural hematoma, will begin experiencing the neurological symptoms caused by this condition.
A subdural hematoma literally means collection of blood beneath the dura mater of the brain.
In the acute type, the hemorrhaging occurs soon after the blow to the head and is life threatening.
In the chronic type, symptoms from the bleeding (e.g., headache, nausea, change in mental status, weakness) begin occurring three weeks to 90 days out.
Do symptoms of a chronic subdural hematoma usually arise in the morning soon after the patient awakens? Or can they strike at any time?
“The symptoms usually do not depend on sleep-wake cycle,” says John M. Abrahams, MD, chief of neurosurgery at Northern Westchester Hospital, and founder of the Westchester Neuroscience Research Foundation which is studying the genomic profile of malignant brain tumors.
“Rather, they depend on severity and can affect someone all day.
“If the patient has difficulty walking or standing, symptoms would be worse upright rather than lying or sitting.
“If the patient has a headache, it can be better when lying flat rather than standing upright.”
If the patient has pre-existing medical conditions, it can be difficult to determine when the onset of the cSDH symptoms begin.
For example, the patient may already have some level of mobility impairment from a past accident or stroke.
The mobility symptoms of a cSDH can mimic that of a stroke.
They may also be in the midst of recovering from, say, knee replacement surgery, and are already physically compromised.
Nevertheless, symptoms of chronic subdural hematoma can begin kicking in at any time during the day, night or middle of the night.
Chronic subdural hematoma generally has a favorable prognosis, especially with surgical treatment.
Studies report survival rates ranging from 80% to 95% post-surgery, depending on patient age, comorbidities and neurological status at presentation.
Note: Survival doesn’t equate to permanent neurological damage following treatment.
Permanent neurological damage after treatment can result from prolonged brain compression before intervention, leading to irreversible injury.
Additional factors include delayed treatment, recurrent bleeding, brain atrophy in elderly patients, or complications such as seizures, infections or stroke.
Damage may also stem from preexisting conditions or impaired cerebral blood flow during the hematoma’s development, all of which can hinder full neurological recovery.
A recurrence of a cSDH occurs in about 10-20% of cases.
Dr. Abrahams is a highly regarded, board certified neurosurgeon who specializes in the treatment of complex disorders of the brain and spine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Can Collagen Injections Cause Misshapen Lips?

Ever wonder if those horrid lip jobs are the result of botched collagen injections?
You’ve probably seen photos of women with grossly enlarged lips that go beyond the infamous “trout pout.”
Can collagen injections ruin a woman’s lips to this extent?
Certainly, many women want a fuller, sexier pout and have been considering collagen injections.
“Misshapen lips that cannot be improved usually happen from procedures where permanent fillers/implants were utilized,” says Allen Gabriel, MD, board certified plastic surgeon with PeaceHealth Medical Group Plastic Surgery in Vancouver, WA.
Collagen injections last three to nine months, and are certainly a practical alternative to something that’s more permanent and has more potential to cause a misshapen appearance.
If lips have become misshapen from a permanent filler or implant, Dr. Gabriel says, “This is when additional surgical procedures are needed to remove the product and can further misshapen the lip.”
This is probably what has happened in most of those hideous photos of “botched jobs” you’ve seen.
Is there an alternative to collagen injections?

Shutterstock/Olena Chukhil
“The nice thing about getting injected with hyaluronic acid products is that this can be immediately reversed if one is not happy with the results.
“There is a solution that can be injected and will immediately dissolve it, and after the swelling goes down, one is back to the original lip shape and size.”
In addition, fat transfer for lip augmentation involves harvesting fat from one part of the patient’s body, processing it and then injecting it into the lips.
This procedure enhances lip volume and contour using your own fat, offering a natural alternative to synthetic fillers.
Results can be long-lasting but may require multiple sessions.
 Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Best & Safest Way to Plump Lips Medically & Look Great

A plastic surgeon explains what works best to medically make lips plumper and fuller.
There’s more than one way to make lips plumper and fuller medically, but is one particular way the best?
Let’s face it: Plump, full lips are a draw. Name one female movie star who didn’t have a good set of lips.
Okay, there might be a very tiny few. But let’s see how easily you can come up with the names of those few.
In the ’70s and ’80s, quite a few TV stars did not have plump lips, such as Farrah Fawcett, Kate Jackson and Cheryl Ladd. By today’s standards, they had thin lips.
But these days, or perhaps beginning in the early ’90s, a trend began kicking in: Want to make it big on TV? You’d better have a killer pout.
Women who star in TV shows that involve a lot of close-up shots while they speak almost always have very well-endowed lips (Jennifer Garner in “Alias,” anyone? How about Leah Remini in “King of Queens”? And let’s not leave out Jeri Ryan in “Star Trek: Voyager”).
Best Way to Get Plumper Lips Medically
Shutterstock/ Sergey Golenko
“Medically ‘plumping’ up lips includes creating a fuller and plumper lip (upper and lower) and reducing fine lines around the mouth,” says Dr. Gabriel.
“Injections of collagen or hyaluronic acid can achieve this with varying lasting results” — three months for collagen and nine months for hyaluronic.
“Additional procedures with implantable products and fat injections can also be done, and these are longer lasting to permanent, but not necessarily the best options as it can lead to unnatural feel of the lip.”
If you want to medically plump your lips, consider the temporary method first.
“When fillers are used for lip plumping one can assess its results and decide if this is something they would like to pursue since the results are temporary,” says Dr. Gabriel.
“If happy with results, discussion of longer lasting procedures should take place with your board certified plastic surgeon or dermatologist.”
Dr. Gabriel is adept at addressing a wide range of concerns, from breast reconstruction after mastectomy and the treatment of congenital anomalies, to complex facial and breast surgeries performed solely for cosmetic improvement.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Sergey Golenko

New Mole but You’re 60-Plus: May Be Melanoma

If you’ve discovered a new mole and you’re 60-plus, don’t wait to get this checked out by a dermatologist.
If you’re over age 60 you may be noticing new spots arising on your skin on a frequent basis (age spots), but suppose you notice something that appears to be a new mole — as in birthmark or like other moles you’ve had on your body since the day you could remember.
It’s not normal for a person over age 60 to develop a new mole.
A mole is not the same as a sun spot or age spot.
What appears to be a new mole may not be an actual mole (known as a nevus to dermatologists—pronounced “nee-vus”).
That new lesion may be a benign skin barnacle, known as a seborrheic keratosis. Or, it could be melanoma.

Seborrheic keratosis. Shutterstock/
Only a biopsy can rule out melanoma. A “new mole” in someone over age 60 should be biopsied for melanoma.
Such a melanoma can progress quickly, as in the case below.

Courtesy of Dr. Gary Goldenberg
“The lesion appeared three months ago and grew rather rapidly,” says Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
Dr. Goldberg explains, “It was slightly painful and itchy. A biopsy was performed and showed a nodular melanoma.
“The patient underwent a surgical excision. Patient is a 68 year old white male who came in with a ‘new mole.’”

Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/wavebreakmedia

Melanoma in Fingernails: Blacks Not Immune to Skin Cancer

People of color are at higher risk for melanoma (skin cancer) in their fingernails.
Melanoma can arise in the fingernail, or nail bed, and is called acral lentiginous melanoma. Below is a photo of what this may look like.
“The patient is a 42 year old black male with pigmentation of the thumb nail,” says Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
“The patient thought that the lesion was caused by trauma and ignored it for over one year.
“The patient presented due to increased pigmentation and pain when using the thumb to perform simple tasks.
“A biopsy was performed and showed a deep acral lentiginous melanoma.
“The patient, unfortunately, required thumb amputation and subsequent chemotherapy.”
Acral lentiginous melanoma is so rare (even in blacks) that most dermatologists won’t encounter it in their professional career.
Melanoma in a nail (which includes toes) may be misdiagnosed as a bruise, fungus or birthmark, and black patients may think it’s benign simply because of their skin tone.
However, a birthmark would have been there since childhood. A fungus will respond to medication, and a bruise will eventually go away when the offender (such as a tight shoe or high heels that compress the toes) is removed.
Beware: Acral lentiginous melanoma can resemble a harmless bruise.
With a bruise that’s underneath the nail, the rest of the finger (or toe) will be normal.
Often, with nail melanoma, it spreads to the cuticle or skin around the nail or behind, and the initial discoloration also spreads.
Acral lentiginous melanoma may also take a straight line shape from nail bed to tip of nail.
It’s normal to develop dark brown or black “streaks” or “slivers” in the nail. In the case of ALM, it’s thick (does not look like a “sliver”) and looks more like a band.
Blacks not Immune
Do NOT avoid getting a biopsy just because you think you’ve convinced yourself that the new symptom is just a bruise or benign streaks or slivers.
Blacks (plus other dark skinned individuals and Asians) are more likely to develop melanoma in the nails than are whites.
Don’t wait; have a dermatologist take a biopsy to rule out anything serious. Chances are it’s benign, but why take chances?
Top image: Courtesy of Dr. Gary Goldenberg
Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Do ABCDEs Always Apply to Melanoma; Can Cancer Look Normal?
What if a melanoma doesn’t conform to the ABCDE guidelines?
Melanoma can pass as a normal mole simply because there’s always a beginning to this disease process.
In very early melanoma, the ABCDE guidelines don’t always apply.
“Melanoma can have many different looks — the lesions may be black, brown, bluish, red or even flesh color,” Gary Goldenberg, MD, of Goldenberg Dermatology, and assistant professor of dermatology and pathology at Mount Sinai School of Medicine.
A normal mole can be raised. Dr. Goldenberg says that melanoma “can be flat or stick out from the skin surface.
Early melanomas are usually flat, and patients are sometimes surprised that a flat lesion can be dangerous. Early melanomas often look benign (normal) to an untrained eye.”
However, a trained eye can miss a melanoma if the disease is early enough, especially if that trained eye does not know what the mole looked like a month or a few months prior.
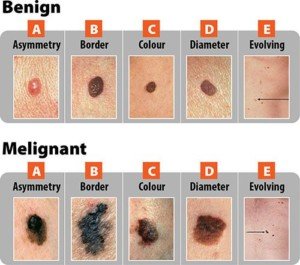
The ABCDEs for Melanoma
A = asymmetry. The spot is not equal on either side of a dividing line. However, a normal mole can be asymmetrical, especially if it’s large.

An asymmetrical mole, though this is considered an atypical mole. Source: Biophoto Associates/Science Source
B = border. The border is jagged or erratic. Again, a normal mole can have this feature.
C = color. A normal mole can be any shade of brown, even black, and may even appear purple or blue due to minute vascularity underneath.

Blue mole. Dannii Brighton, CC
D = diameter. A normal mole can be larger than a pencil eraser, and a melanoma that arises in the absence of a pre-existing mole has to start out somewhere: a tiny pinpoint.
E = evolving. This is the key. Has that black mole always been black? Has that “funny” mole always been asymmetrical or had ragged edges? Has that spot on your back always been the diameter of a dime?
“As melanomas progress, they may become more of a bump – that’s called nodular growth phase,” says Dr. Goldenberg.
“These are the most dangerous lesions, since they grow into the skin and can spread to other organs.”
A melanoma is as deep as it is high.
If it’s 2 mm above the skin, it’s 2 mm beneath the skin.
“There is a misconception that a mole with hair growing through it is more likely to become melanoma; it’s simply not true.
“This is why I tell my patients to have their moles checked once per year and to see me if there is a new or changing lesion.”
Dr. Goldenberg of Goldenberg Dermatology provides comprehensive care in medical and cosmetic dermatology, including melanoma and other skin cancer, moles, psoriasis, eczema and acne. He is the medical director of the Dermatology Faculty Practice, NY.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Is Blonde Hair a Melanoma Risk in a Biracial Person?

Blonde hair (which usually goes with fair skin) is a melanoma risk factor, but what about for biracial people with olive or caramel skin?
How often have you read that “blonde hair and blue eyes” are a risk factor for melanoma, along with “fair,” “pale” or “light” skin?
Certainly you’ve read that dark skinned people have a lower risk for melanoma when compared to light skinned people.
So here’s an interesting question that I posed to Dr. Rebecca Baxt, a board certified dermatologist with Baxt CosMedical:
Is blonde hair relevant as an added risk factor for melanoma in biracial individual?
After all, some biracial people have varying shades of blonde hair as well as skin tones.

“These are questions that we really don’t know exact answers to,” says Dr. Baxter, “as there are no good prospective studies looking at eye color and hair color and parentage and how much skin cancer these populations develop.
“From clinical experience, darker skinned people have lower risks of all skin cancers, but not zero risk.”
An even more interesting question is if blonde hair means an increased risk of melanoma in a very dark skinned individual.
Below are natives of the Solomon Islands who have a gene called TYRP1, which causes blonde hair.
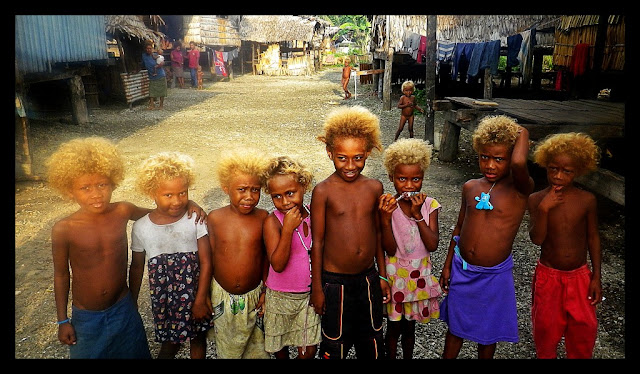
As Dr. Baxt has stated, there is no data on this. Nevertheless, no human is immune to melanoma.
In fact, melanoma can appear in areas that get very little sun exposure, which means that in those cases, the amount of natural melanin (skin pigment) would not play a role.
Plus, biracial people and those with a deeper olive complexion, have been known to get the sun-related skin cancers of basal cell carcinoma and squamous cell carcinoma.
And don’t forget that sun exposure and light skin are not the only risk factors for melanoma, especially the type of tumor that develops inside the mouth, nose or eye.
Genetics do play a role, even in those with dark skin. Researchers also believe there are risk factors not yet discovered.
Dr. Baxt is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
is an assistant clinical professor of dermatology at NYU and a member of the Skin Cancer Foundation. She also specializes in laser treatments, skin rejuvenation procedures, acne treatment and rosacea treatment.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}