

Normal Stress Test but a Massive Heart Attack the Next Day ?

A cardiologist explains why you can have a normal stress test one day and then a massive heart attack the next.
You’ve probably heard of instances in which a person had a normal stress test but then next day dropped dead of a massive heart attack. How can this be?
“We have more and more theories about how plaque develops within the coronary arteries,” says Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“We are starting to understand how soft plaque can rupture and lead to greater plaque formation.
“Sometimes these ruptures are minor and result in minor or no symptoms, but other times the rupture can be catastrophic, resulting in a totally occluded artery where before there had only been minor non-obstructive plaque.
“This catastrophic rupture often explains how a patient can have a normal stress test one day and a massive heart attack the next.”
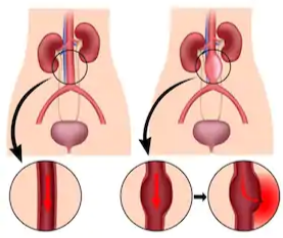
To make this easier to understand, imagine a tube. The inner wall of the tube is only lightly covered with patches of sludge.
Water flows freely through the tube; there is no narrowing or restriction of the water flow.
One day, a piece of the sludge dislodges from the inner wall and travels down the tube, getting stuck at some point—stuck in a way that it blocks the flow of water.
That’s how a heart attack occurs when soft plaque ruptures in a coronary artery that, according to a stress test, has no restricted blood flow.
What a Stress Test Looks For
A stress test measures perfusion: blood flow through the coronary arteries.
A stress test does not measure amount of soft plaque, and it’s the soft plaque that can rupture (hard or calcified plaque can’t).
To kick back any soft plaque you may have in your coronary arteries, avoid processed food as much as possible.
So if you want a chicken, rice and broccoli dinner, make it the way someone in the year 1902 would have made it, rather than buying a frozen dinner.
Though it’s nice to know that one’s stress test was normal, there’s always that small chance that a massive heart attack is around the corner.
This is why it’s so important to keep on top of your heart health even if you don’t seem to have any risk factors or suspicious symptoms.
 Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock

Is Exercise Safe if You Have PVCs 24/7?

A cardiologist addresses exercise safety in people with many PVCs, even nonstop.
Some people have premature ventricular contractions seemingly nonstop, thousands and thousands a day, and fear that exercise may not be safe for them.
“PVC’s had a bad reputation many years ago,” begins Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“When I was first in training, we were very aggressive in treating PVCs, especially in patients who had CAD, because the theory was that patients with PVCs were at high risk for cardiac arrest (V-fib or V-tach).”
CAD stands for coronary artery disease.
Dr. Reynolds continues, “In fact, we tried suppressing them with two infamous medications – Encainide and Fleciainide. Unfortunately, more patients died from the medications than from the PVCs.
“Since then, we’ve done a lot more research on PVCs and ventricular arrhythmias and risk of sudden cardiac death.
“We now use beta blockers, amiodarone, and ICDs (implantable defibrillators) in patients at high-risk for sudden death (low EF, prior cardiac arrest, etc.).”
EF stands for ejection fraction, the amount of blood that the heart beats with each pump. A low EF corresponds to weak pumping ability.
Exercise with PVCs Is Safe for Healthy Individuals
“PVCs in a healthy patient are rarely anything to worry about,” says Dr. Reynolds.
“We usually will do a holter, echo, and stress test to screen for more ominous arrhythmias.

Freepik.com
“Family history is also important to document, i.e., any family history of sudden death?
“Assuming everything checks out fine, then yes, you can exercise to your heart’s content (pun intended). Exercise actually suppresses benign PVCs.”
Exercise is safe for those with premature ventricular contractions who are healthy. This includes strength training.
Don’t let PVCs stop you from exercise if your cardiologist has given you the green light.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

How Does Exercise Suppress PVCs?

A cardiologist explains how exercise suppresses or inhibits PVCs: premature ventricular contractions.
Though some people with PVCs wonder if it’s safe to exercise, it’s a well-documented fact that exercise suppresses PVCs.
In fact, many individuals who have frequent premature ventricular contractions report that exercise is a reliable, predictable way to stop them cold.
How does exercise stop or suppress premature ventricular contractions?
“Premature beats originate during the ‘resting’ phase of the cardiac cycle, i.e., the time when the myocardial electrical activity has reset itself and is waiting for the next electrical wave coming down from the atria -> through the AV node -> through the His bundles -> and then through the ventricular myocardium,” explains Monica Reynolds, MD, a cardiologist with ColumbiaDoctors Medical Group in White Plains, NY.
“With exercise, the heart rate increases which essentially shortens the ‘resting’ time and reduces the amount of time that PVCs can originate.
“Basically, the increased electrical activity of the faster beating heart overrides the aberrant beats in the ventricles.”
So even though you may have heard that the reason exercise seems to make PVCs go away is because PVCs can’t be felt as much when your heart rate is elevated and you’re huffing and puffing during physical activity, it’s a fact that working out actually inhibits PVCs.
And this process has nothing to do with the individual’s perception.
Since 1992 Dr. Reynolds has practiced clinical cardiology at ColumbiaDoctors Medical Group, one of the largest multi-specialty practices in New York State.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

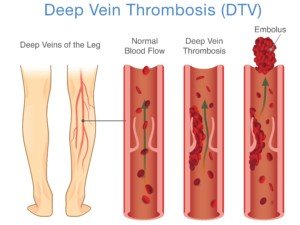
Deep Vein Thrombosis (DVT) Prevention: 7 Lifestyle Changes

Making lifestyle changes to help prevent a DVT is as easy as 1 through 7.
Deep vein thromboses are much more common than you think and are very dangerous, requiring immediate medical intervention.
“The problem isn’t the formation of the clot in the leg (although it is painful and causes significant morbidity such as swelling of the leg),” begins Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“The real risk is if the clot breaks off from its location in the leg and travels to distant parts of the body,” continues Dr. Besser.
“Once there, it can lodge in a blood vessel and cause that blood vessel to block. If there is no blood flow — that area of the body ‘starves from the lack of blood.
“The most common site for the clot to travel is the lungs (pulmonary embolus). That causes the lungs to work less efficiently — so less oxygen (a necessary substance for life) is absorbed.
“It is also possible for a small clot to pass through the lungs and lodge in a heart blood vessel which can cause a heart attack, or into the brain which can cause a stroke.”
You can now clearly see why making lifestyle changes to prevent a DVT is so crucial to one’s overall health regimen.
Even athletes can get a DVT. This disorder is not reserved just for the old and sick!
A DVT is a very preventable condition, even though a pulmonary embolism kills a person in the U.S. approximately every five minutes.
Big Steps Towards Preventing DVT
These ways to help prevent a DVT come from research that was presented at the Arteriosclerosis, Thrombosis and Vascular Biology 2013 Scientific Sessions.
- Exercise
- Don’t smoke
- Eat healthfully
- Avoid being overweight
- Control blood sugar level
- Control blood pressure
- Control cholesterol
These seven lifestyle factors go a long way in preventing DVT.
A study followed over 30,000 adults 45-plus for 4.6 years. Blood clot incidence was compared among three groups:
1) inadequate heart health
2) average heart health
3) optimal heart health.
Blood Clot Risk in the Study Subjects
- 44 percent lower in those with optimal heart health when compared to inadequate heart health.
- 38 percent lower in those with average heart health when compared to inadequate.
Out of the seven, what were the top two as far as greatest effect on lowering DVT risk? Exercise and weight control.

Shutterstock/wavebreakmedia
So now you have even more motivation than ever to lose body fat and stay on an exercise program. Exercise should include strength training.
And please, don’t assume you have an automatic built-in exercise regimen just because you do housework or have a staircase in the home.
A deep vein thrombosis is a lot more powerful than household chores!
Do your part in helping prevent the development of a DVT by following the seven lifestyle changes here.
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: sciencedaily.com/releases/2013/05/130502185419.htm
ABDOMINAL AORTIC ANEURYSM: Surgery, Drugs, Watchful Waiting
An abdominal aortic aneurysm is a very serious condition, but not all cases require treatment.
The aorta is the largest blood vessel in the body.
It comes out of the heart and travels all the way down the abdomen, where it branches off to feed blood to the lower extremities as well as organs, especially the liver and kidneys.
Usually, a bulging section of this great vessel is discovered by accident, when the patient is imaged for an unrelated cause.
For example, he might undergo an X-ray covering the abdominal region for an unrelated issue, and the ballooned portion of the aorta is picked up on the study.
Treatment for an Abdominal Aortic Aneurysm
If the vessel is only mildly dilated, the treatment will be ongoing surveillance via imaging studies to track the growth of the aneurysm.
“If you have been diagnosed with an aortic aneurysm and have been told to simply observe symptoms, know what symptoms you should be looking for,” says Walter Gaman, MD, FABFM, board certified in family medicine and the author of several award-winning books including “Age to Perfection: How to Thrive to 100, Happy, Healthy, and Wise.”
“This will allow you to recognize a serious change in your condition.”
The symptoms may be abdominal pain, back pain, a bulge in the lower abdomen and/or feeling a throbbing pulse in the lower abdomen (without actually touching the area with your fingertips).
“Also, share these symptoms with your family members so they will know how to react in case of an emergency,” says Dr. Gaman.
If the aneurysm ruptures, the pain will be sudden and agonizing, capable of bringing the person to the floor.
“Alerting medical personnel early will help your chances of survival. The most common symptom is intense pain in your abdomen, side, or back.”
The excruciating pain of a ruptured abdominal aortic aneurysm may be the person’s first symptom.
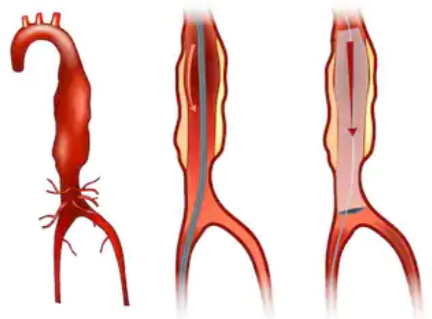
The mortality rate is very high due to the rapid internal hemorrhaging. Below is a graphic image of an actual AAA.

Hertzer NR, CC
Risk Factors
- Male gender
- Over age 70
- Smoking
- High blood pressure
- Family history of AAA
Ongoing Surveillance
“Aortic aneurysms should be monitored yearly,” says Dr. Gaman. “If they get to or above five to six cm in diameter, surgical intervention may be necessary.”
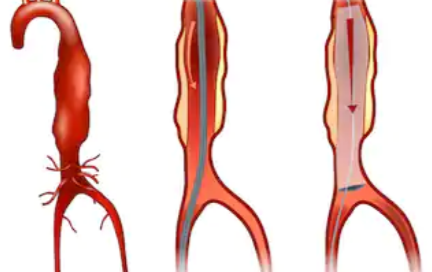
Sometimes, though, when an abdominal aortic aneurysm is discovered, it’s already at a life-threatening size, and the diseased portion must be repaired asap.
The repair may be done invasively by opening up the abdomen, or, it may be done endovascularly, which means a shorter recovery time and lower risks of complications.

Dr. Gaman is with Executive Medicine of Texas and is with the Staying Young Radio Show 2.0 podcast.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Alila Medical Media

Peripheral Neuropathy Misdiagnosis: Doctors Miss Disease

Just because doctors haven’t mentioned peripheral neuropathy as the cause of your pain, doesn’t mean you can’t have it.
“Peripheral neuropathy” means disease of the nerves of the peripheral nervous system, and I know at least one person who’s been recently diagnosed with this — after it was missed for the past four years by a steady stream of doctors: my father.
For about four years he’d been complaining of pain in his legs, and several doctors attributed this to problems with his low back, including spinal stenosis. Two endoscopic back surgeries didn’t help.
Another doctor said it was from osteoarthritis of the hip and recommended a hip replacement, which my father had; it did no good.
He’s had three knee replacement surgeries by two orthopedic surgeons who both said that the leg pain was caused by osteoarthritis in his knees.
The second surgeon, who did the third knee surgery (a revision) said that the pain could very well be from a failed knee replacement.
What seems to make it easy for doctors to miss peripheral neuropathy is when the patient actually has these other conditions, which are easily proven with X-rays and MRIs.
My father has had more than one primary care physician over this time period, who named back and knee problems, as well as old age, as probable causes of the leg pain.
Other proposed explanations for the leg pain was a knee infection, and allergic reaction to the knee replacement device.
Early on, an adverse side effect to my father’s use of a statin drug was suspected, but ruled out after he went off the statin but the leg pain continued.
Strangely, none of these many doctors came up with, “You know, this very well could be peripheral neuropathy. Let’s aggressively pursue this possibility.”
Peripheral Neuropathy Doesn’t Necessarily Work Alone
If you have degenerated knees or lumbar discs, this doesn’t mean you can’t also have peripheral neuropathy adding to your lower body pain, burning and tingling.
Peripheral neuropathy is associated with diabetes; diabetes is the most common cause.
A doctor may rule out peripheral neuropathy if you don’t have diabetes (my father doesn’t), and especially if you have other “differentials” that can explain the leg pain, such as degeneration of the lumbar spine as shown on imaging tests.
How did my father finally get diagnosed with peripheral neuropathy?
His assortment of doctors would have continued to miss this had he himself not decided one day to review his medical records over the past four years.
He’d had an EMG about three years ago and the doctor said he had “nerve damage.” However, that doctor, plus his primary care doctor at the time, didn’t further pursue this “nerve damage,” and thus, my father had thought nothing of it.
My father found the words “peripheral neuropathy” in the paper work as a diagnosis, and was floored that nothing ever came of this; no further workups or recommended drugs.
He immediately contacted his newest PCP, who in turn ordered blood tests to rule everything else out.
Within 24 hours of the blood tests, my father was prescribed Nortriptyline, a tricyclic antidepressant that’s also used to suppress the pain of peripheral neuropathy.
At the time of this writing, he has not yet gotten the prescription because it was ordered late Friday afternoon.
Why, after four years, did so many doctors not think of peripheral neuropathy?
And why didn’t the EMG neurologist pursue it? It’s because sometimes, the patient knows more than their physician.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/BEAUTY STUDIO
What’s the Death Rate of Abdominal Aortic Aneurysm Repair?
The death rate following the repair of an abdominal aortic aneurysm is something that you’d definitely want to know.
However, if your doctor is already discussing surgical treatment with you, it’s a safe bet that it would be very dangerous to decline surgery.
After all, the aneurysm in your abdominal aorta is at high risk of rupturing, and the internal bleeding from that can be fatal in minutes.
All invasive surgeries do carry risks, and surgeons always weigh the benefits of the surgery against the risks of going without it.
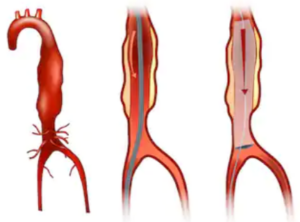
The case of an abdominal aortic aneurysm is no exception to this standard of medical practice. Below is a graphic image of an actual abdominal aortic aneurysm. This particular AAA had not been repaired, as is evident.
Hertzer NR, CC
“Most randomized control trials indicate the 30-day perioperative mortality for elective repair of abdominal aortic aneurysm is about 5%,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
“This is major surgery and presence of a AAA is a marker for other significant cardiovascular disease. As a matter of fact, beyond the 30-day, most people die from other cardiovascular causes, such as MI, CVA, etc.”
MI = myocardial infarction (heart attack).
CVA = cerebral vascular accident (stroke).
It is advised that men over the age of 70 be screened for the presence of an abdominal aortic aneurysm.
In addition to male gender and older age, high blood pressure and smoking are risk factors.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Sakurra

How Long Does It Take DVT to Get to Lungs After Breaking?

A DVT (blood clot) that’s in your leg has a chance of breaking apart or completely dislodging and then going to your lungs…and how long this takes is not what you may think it is.
I was reading in a health anxiety forum a lengthy thread that was started by a person who’d been at her computer for “three days” googling things relating to health — but not DVT.
She took breaks only to use the bathroom, catnap here and there, maybe eat a little something, but essentially it was a marathon at the computer for three days.
Upon getting up at the end of the computer stint, she felt a pain in her calf and googled this, learning that marathon sitting at a computer can cause a blood clot.
She then freaked out, convinced that there was a DVT in her calf. She kept making posts in the thread over a 45 minute period, corresponding in the then-real-time with a few other caring health anxiety sufferers.
At some point she then said the pain had moved up to her knee and was panicking that the DVT had broken off and was on the way to her lungs.
This post was maybe 10 minutes after the first one.
Then 15 minutes later she made a post that her thigh was hurting, and could the DVT then be in her thigh on the way to her lungs?
Shutterstock/solar22
What a Vascular Surgeon Says
According to the times these posts were made, 15 or so minutes had lapsed between the onset of the knee pain and the thigh pain.
She was convinced that this meant that the DVT was enroute to her lungs.
When a blood clot gets into a lung, it’s called a pulmonary embolism.
Blood Clot in a Leg: Hare or Turtoise?
So if a DVT breaks off or dislodges from its location in the leg, just how long will it take to get to the lungs and become a pulmonary embolism?
“Generally, it is immediate (do not know the exact time period), but by far the majority remain clinically silent since they can be very small,” explains Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
Imagine that you have a DVT anywhere in your leg, and suddenly, a part of it breaks off or dislodges.
This clot material then gets swept up by the venous flow that returns de-oxygenated blood to the lungs.
This is akin to tossing stuff in a river, and the flow of the river carries it downstream.
Of course, veins in the legs pump blood “upstream,” but the principle is the same:
The bits of DVT immediately get carried away with this blood circulation and, like Dr. Gashti says, the time lapse is immediate from when the clot dislodges to when it arrives in the lung (pulmonary artery).
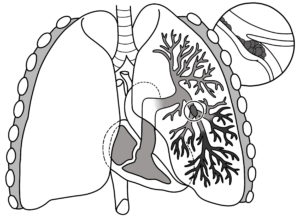
Pulmonary embolism
Think of it this way:
The time it takes for a broken DVT to get to your lungs is the time it takes for the blood in your calf vein, at any given time, to get to your lungs. That’s just seconds.
Though most pulmonary emboli don’t produce symptoms due to being very small, this doesn’t negate the estimated 300,000 U.S. deaths every year to a pulmonary embolism.
A pulmonary embolism is a common event in the U.S. population.
DVT Risks
Recent surgery
Excessive bedrest
Smoking
Obesity
Pregnancy
Extended air travel
Extended vehicular travel
Lack of exercise
Senior age
If you suspect a DVT, and knowing that if it dislodges, the occurrence of a pulmonary embolism will be literally within seconds, don’t delay getting yourself checked out in the nearest emergency room.
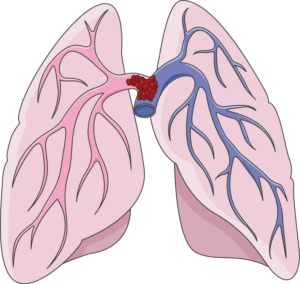
A “saddle” type pulmonary embolism, plugging up the area where the pulmonary artery splits off into each lung. This can cause death in minutes. Laboratoires Servier, CC BY-SA/creativecommons.org/Wikimedia Commons
The time between when a blood clot breaks to when it reaches the lungs is a few SECONDS.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ShotPrime Studio
Can You Get a Pulmonary Embolism without a DVT?

Find out the interesting answer to the question: Can a pulmonary embolism form in the absence of a DVT?
“By definition a PE is an ‘embolus’ that has traveled to the lungs,” says Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
An embolus is a thrombus (blood clot) that is dislodged from one place and ends up in another.
“It can be both venous and arterial. Of course a pulmonary embolus must have a venous source.”
In other words, in order for a blood clot to end up in a pulmonary artery, it has to travel there somehow, and the only way is via veins (venous pertains to veins).
“I assume that one can form a thrombus de novo [originating from] in a pulmonary artery, but that would not be considered a PE.”
Remember, embolus refers to a blood clot that has dislodged. So if the clot originates in the lungs, it’s not a “pulmonary embolus.”
“Not infrequently a patient has a pulmonary embolus, but a source cannot be found,” continues Dr. Gashti.
“In these cases the possibilities include: thrombus completely broke off from the original vein and therefore none can be found now; thrombus was in a vein in the upper extremity which normally is not studied in a patient with a PE unless clinically indicated, or that it came directly from the right heart (after open heart surgery), after having a heart attack, or from a tumor, i.e., myxoma.”
A myxoma is a rare, usually noncancerous tumor made of soft, jelly-like tissue, and it often arises in the heart, which can sometimes cause blockages or heart problems.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can a DVT Cause Swelling in the Ankle Only & Nowhere Else?

How likely is it that the swelling in only one ankle, but nowhere else in the leg, is being caused by a deep vein thrombosis?
A DVT typically causes swelling up and down the lower leg and may include the ankle.
But is it possible for this kind of blood clot to swell up ONLY the ankle?
Can a deep vein thrombosis cause swelling only in a person’s ankle?
“That would be unusual, unless the very distal tibial veins are thrombosed, in which case it would not be of great significance, again because these emboli would be very tiny,” explains Seyed-Mojtaba Gashti, MD, a board certified vascular surgeon with Broward Health Medical Center in Florida.
The distal tibial veins are the veins in the front or anterior of the lower leg where the tibia bone is.
The tibia is the larger of the two lower leg bones. Distal means distant from the center of the body, so in this case, the location would be near the ankle.
Thus, if a DVT forms near the front of the lower leg near the ankle, the clots would be, as Dr. Gashti says, “very tiny,” and thus not potent enough to cause swelling going up the leg, but rather, more likely confining it to only the ankle.

Scientific Animations, Creative Commons/BY-SA
Warning Signs of a DVT Other than Swelling
• One area of the leg is much warmer than the other.
• Area of suspicion is unusually tender to the touch.
• There is pain, even at rest, in the calf or behind the knee. The pain may feel like a strong soreness or a cramp.
• The area is noticeably reddish.
• You very recently had joint replacement or abdominal surgery.
• You’ve recently had excessive bed rest.
• You’ve recently been on a long airplane flight.
Dr. Gashti specializes in the diagnosis and treatment of vascular disease including abdominal and aortic aneurysm. He received his medical degree from the University of New England College of Osteopathic Medicine and has been in practice for more than 20 years.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}