

Neck, Throat Soreness: May Be Caused by Exercise

I was noticing a strange though mild soreness in the front of my neck soon after I awakened, and initially didn’t know what could have caused it.
Then I soon realized that the day before, I had been doing standing overhead presses.
This exercise involves standing in one spot with feet about shoulder width apart, and pressing a barbell overhead.
This is not the most common exercise, but it’s a very functional one that also strengthens the lower back. Proper form is crucial.
You may think that the standing overhead press works only the shoulders, arms and core, but pay closer attention next time you’re pressing up a heavy barbell.
The muscles in the neck are subjected to isometric contractions: The muscles are under tension, but do not lengthen or shorten.

If you raise your head just even a little bit while fighting to get the barbell completely over your head, this can set you up for some neck soreness (in the front) the next day.
Since the muscles in the neck go over the throat, you may perceive what seems to be soreness in the throat area as well (not like a “sore throat” from a cold, but a soreness in the front of your neck where the throat is). The soreness may also be under the jaw.
Whenever I have this soreness, it’s the day after heavy standing overhead presses. It’s also very transient in that it dissipates as the day proceeds.
Pay attention to your neck the next time you’re pushing up heavy weight.
You will note that the muscles in this area are straining. They certainly aren’t doing nothing, that’s for sure.
This will be particularly evident if you use good form: feet flat on floor, no jerking up the weight.
A calm rather than jerky pressing motion will enable you to better tune in to how your various muscles are making this exercise possible. The neck is not excluded.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/9nong

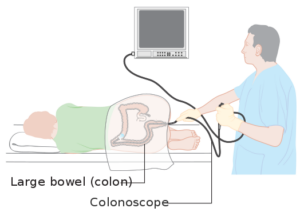
Did the Colonoscopy Miss a Cancer or It’s a New Fast Tumor?

When colon cancer develops between routine colonoscopies, does this mean it was missed or is it usually a new fast growing tumor?
We are advised to have a screening colonoscopy beginning at age 45 and then every 10 years to catch colon cancer.
People with above average risk, including those for whom polyps were found, have shorter intervals between screening colonoscopies.
Nevertheless, it happens: A colon cancer is discovered between colonoscopies.
This includes at some point after the previous colonoscopy was deemed normal.
Imagine being told, “Your colonoscopy was normal,” and then several years later you begin developing concerning symptoms and are diagnosed with colon cancer.
Did the colonoscopy miss this cancer or did it spring up out of nowhere a few years later?
“Interval colon cancers are defined as those cancers diagnosed after a previous colonoscopy and before the next screening/surveillance colonoscopy,” says Santosh Sanagapalli, MD, a consultant gastroenterologist, endoscopist, colonoscopist and specialist in esophageal and bowel disorders.
“There are four possible reasons for interval cancers developing.”
• Polyps that were missed on the initial colonoscopy, that progressed to a cancer.
• Polyps identified on the initial examination, but incompletely resected.
• New polyps developing following the initial colonoscopy, that rapidly progressed (the standard rate of progression from small polyp is generally thought to be at least a decade or more).
• Failure to visualize a cancer that was present on the initial colonoscopy.
“It is very difficult to determine which of the four causes is responsible for development of an individual case of interval cancer.
“However, using mathematical models, others have concluded that the majority of interval cancers result from missed rather than new lesions.
“The colonoscopy is highly dependent on its operator, and there is now plenty of evidence for this.”
How does a colonoscopy miss a tumor?
Cancer Research UK
“There is substantial variation in detection of adenomas (the most common precursor of colorectal cancer),” continues Dr. Sanagapalli.
Researchers from Huntsman Cancer Institute (HCI) at the University of Utah looked into this phenomenon and discovered:
1 The interval colon cancers tended to appear in patients 65-plus
2 In patients with a family history of the disease
3 In those who’ve previously had polyps
Not only that, but the “missed” cancers in the study’s patients tended to appear on the right portion of the colon, which, interestingly, is at the far end of the reach of the colonoscope.
“Further, large U.S. studies have shown that the adenoma detection rate of a colonoscopist (measured as a percentage of all colonoscopies they perform where they detect an adenoma) is inversely proportional to the rate of interval cancer in their patients,” says Dr. Sanagapalli.
“Put in other words, the more adenomas a colonoscopist detects in their colonoscopies, the less likely they are to ‘miss’ significant lesions that can turn into an interval colon cancer.”
This is why, when you’re seeking a gastroenterologist to perform your colonoscopy, you should ask what his or her adenoma detection rate is.
It is perfectly fine for the patient to seek this information, and you should never be reluctant to.
It should be at least 15% for female patients and 25% for male.
Don’t Squawk About the Prep
“If the bowel is not adequately cleansed, fragments of stool and debris can easily obscure a small polyp/adenoma that may then be missed and turned into cancer,” says Dr. Sanagapalli.
“For this reason, much research has gone into improving the quality of bowel preparation in recent years.
“One major advance in recent years is our understanding of the value of ‘split’ bowel preparation.
“This is where the last dose of the bowel preparation is taken on the day of the surgery (usually two to four hours prior to the procedure), rather than the night before.
“This has been shown to improve the quality of bowel preparation significantly, especially in the right colon.
“By doing so, the rate of detection of polyps is improved, and therefore the risk of interval cancers is reduced.
“For this reason, ‘split’ bowel preparation has now become the standard of care.”
Can we ever prevent a missed colon cancer?
“Even with the best colonoscopists and perfect bowel preparation, not all interval cancers will be prevented.
“There is evidence to suggest that around a quarter of interval cancers occur through no deficiency of the initial colonoscopic examination, and are simply due to a new polyp that rapidly progressed.
“Ongoing research is focused on identifying characteristics of patients and polyps that may have rapidly progressed, so we can schedule more frequent colonoscopies for such patients.”
- Blood in the stools — could be red, reddish brown or even black with a tarry look
- Pencil-thin or ribbon stools
- Feeling of incomplete voiding after a bowel movement
- Constipation or diarrhea
- Alternating constipation with diarrhea
- Odd change in bowel habits
- Abdominal pain or cramps, gas
- Feeling of bloating or fullness
- Unexplained weight loss or fatigue
- Back pain
 Dr. Sanagapalli is a gastroenterologist and director of the Esophageal Disorders Center at St Vincent’s Hospital, Darlinghurst. He performs diagnostic and therapeutic endoscopic procedures, and enjoys providing comprehensive and holistic care to patients with a wide variety of disorders affecting the gastrointestinal tract.
Dr. Sanagapalli is a gastroenterologist and director of the Esophageal Disorders Center at St Vincent’s Hospital, Darlinghurst. He performs diagnostic and therapeutic endoscopic procedures, and enjoys providing comprehensive and holistic care to patients with a wide variety of disorders affecting the gastrointestinal tract.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: sciencedaily.com/releases/2014/03/140320173512.htm

Extremely Dense Breasts: Mammograms & Advanced Imaging

It’s not pretty finding out you have “extremely dense” breasts — because this is a big risk factor for breast cancer; what makes this worse is that a tumor can pass as benign fibrous tissue on a mammogram reading.
A cancer surgeon and a diagnostic radiologist weigh in on extremely dense breasts, mammograms and an advancement in imaging.
Do you have “extremely dense breasts” and have read that this is a risk factor for breast cancer and/or that this situation makes it more difficult for a tumor to be detected by eye on a mammogram?
For this article I consulted with Dr. Steven Standiford, MD, Chief of Staff Emeritus at the Cancer Treatment Centers of America Breast Cancer Institute across all five CTCA sites, and Dr. Debora Fineman, MD, a diagnostic radiologist formerly with the Philadelphia CTCA.
“Regarding extremely dense breasts and the risk of breast cancer, the issue is more that extremely dense breasts make it difficult to DETECT cancer mammographically,” says Dr. Fineman.
Imaging for Extremely Dense Breasts
“A fairly recent advancement in mammography, Tomosynthesis, is quite beneficial in evaluating dense breasts, as it enables visualization of the breast in ‘layers,’” says Dr. Fineman.
“Most insurance companies will not cover this as a screening procedure. We do get tomosynthesis coverage for performing diagnostic workups such as evaluating an abnormal screening mammogram or evaluating a clinical problem.
“Screening tomosynthesis is readily available, with some institutions collecting a nominal out-of-pocket.”
Your gynecologist may order this test for you if it’s available in your health network even if it isn’t covered, so ask about it.
What about the MRI for extremely dense breasts?
Dr. Fineman says that coverage for the cost varies across insurance companies, and that most insurance companies will not pick up the cost for MRI screenings.
“I believe the research has not yet been finalized as to risk stratification and frequency of performing screening MRI evaluations,” adds Dr. Fineman.
Dense (fibrous) breast tissue appears as white on a mammogram. So do tumors. But in addition to this visual issue, it’s true that having more fibrous tissue and less fatty tissue increases a woman’s risk of the cancer.
Just how much of an increase is up for debate. This all begs the question: Why isn’t an MRI screening covered by insurance for patients with dense breasts?
Dr. Standiford has this to say: “I worry about policies mandating coverage of a specific, as yet unproven test – for as yet, MRI has not impacted breast cancer mortality, and the resources could be better utilized in expanding mammography coverage – the impact would be far greater.
“Also, newer technology is on the way, for example higher resolution ultrasound, tomosynthesis mammography and breast CT, which may have more utility in screening dense breasts.”
 As a part of Dr. Standiford’s life-long commitment to improving cancer treatment, he has partaken in wide-ranging research and has been awarded grants to study breast and colon cancer.
As a part of Dr. Standiford’s life-long commitment to improving cancer treatment, he has partaken in wide-ranging research and has been awarded grants to study breast and colon cancer.
 Dr. Fineman has been in practice for 30+ years.
Dr. Fineman has been in practice for 30+ years.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Billion Photos

Can Breast Cancer Be Spread by Mammogram Compression?

Find out what a breast cancer surgeon has to say about the idea that a mammogram can compress a pre-existing tumor and make it spread.
The compression from a mammogram can hurt quite a bit.
This can make some women wonder if this painful compression could somehow squeeze out an undiagnosed malignant tumor to the point of scattering it beyond its local position.
So the big question becomes: If there’s cancer in the breast, can what feels like excessive compression can make it spread or disseminate it to other parts of the body?
The Answer
“Manipulation of a tumor – whether by exam, compression of a mammogram, ‘disrupting’ the tumor with a needle biopsy, or manipulating the tumor at surgery – has NOT been shown to increase the risk of tumor recurrence or dissemination of metastases,” explains Dr. Steven Standiford, MD, Chief of Staff Emeritus at the Cancer Treatment Centers of America Breast Cancer Institute across all five CTCA sites.
Spread of Cancer Cells
Dr. Standiford explains, “Cancer metastasis is a complex dance between tumor cells separating themselves from the initial tumor, having the biochemical reactions that loosen the bonds between cells so that one can break free, having access to blood vessels or lymphatics to have a highway to travel, avoiding identification by the immune system, and having a site which provides an appropriate milieu for the cell to develop into a metastatic lesion.
“Compression, or exposing the tumor to the air, or any other single factor will not change the nature of the disease, which is determined by the tumor and not how hard it is squeezed.”
In short, malignant breast tumors are “tough” and don’t just break apart.
If you are still concerned about the “spread” of cancer cells during a mammogram, you may want to consider having a whole-breast screening performed via ultrasound — as this does not involve compression of the breast tissue.
You should discuss the pros and cons with your women’s health physician regarding screening technology.
Keep in mind that not all insurance plans will cover the cost of a screening ultrasound, and in fact, the procedure may not even be offered by your health plan.
However, independent imaging centers will provide screening ultrasounds for breast cancer, though you may need an authorization from your doctor to have it done.
As a part of Dr. Standiford’s life-long commitment to improving cancer treatment, he has partaken in wide-ranging research and has been awarded grants to study breast and colon cancer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Cancer.gov/ Bill Branson

Menstrual Pain Every Day but Gyno Tests Are Normal?

Have you ever had menstrual pain or cramps but no period?
If your only symptom is pelvic discomfort, a number of conditions can cause this.
But the more locations of your body, that have the aches or pains, that get added into this equation, the fewer the conditions that can explain this.
Thus, the possibilities get narrowed slightly when, in addition to pelvic cramps, you also get low back aches.
Toss in wrist, ankle and neck aches, and this eliminates gynecological causes such as pregnancy, ovarian cysts, endometriosis and gynecological cancer, and it also eliminates colon cancer.
Joint aches other than in the back are not on the symptom lists for these cancers.
So what on earth can possibly cause period pain in the absence of the above, and in the absence of pregnancy, periomenopause, menopause and celiac disease?
Consider the possibility of inflammatory bowel disease! One such condition is microscopic colitis, a benign inflammatory bowel disease that will never turn into anything serious.
“How can I have colitis if I don’t have any digestive symptoms, no diarrhea, no constipation, no flatulence, no gas?”
Microscopic colitis, as well as other IBDs like Crohn’s and ulcerative colitis, can cause “extra-intestinal” symptoms (e.g., beyond the intestines), that can surface IN THE ABSENCE of gut-related symptoms.
What causes menstrual joint pain?
Prostaglandins, which are hormone-like chemicals produced throughout the body, including the uterus.
This is why ibuprofen alleviates this pain, because it inhibits production of prostaglandins.
What’s believed to cause the joint aches of microscopic colitis?
Prostaglandins.
“Aching joints can be a symptom of microscopic colitis, but not necessarily. Many patients with aching joints don’t have microscopic colitis, but aching joints and gut problems often go hand-in-hand.
“They’re both associated with inflammation, and many doctors speculate that cyclo-oxygenase (COX 2) or prostaglandins are involved because of the function they provide.
“Prostaglandins are chemicals that generally cause inflammation of our joints.”
– Dr. Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving, as interviewed in my article, Why Does Microscopic Colitis Cause Joint Pain?
If you’re having unexplained joint aches and pelvic cramping that feel menstrual, like you’re about to get your period, but the period never comes, there IS some degree of possibility that this could be microscopic colitis, if all of your other tests have turned up negative, and ESPECIALLY if you’re over 50.
Even if there’s no diarrhea. However…the diarrhea may come yet. When I had my second flare-up of microscopic colitis, the period pain was present (and significantly) for about 27 days BEFORE the diarrhea and other gut symptoms started.
Then out of 32 days that followed from the first day of diarrhea, I had a total of 27 episodes of diarrhea.
The diarrhea came on rather suddenly and tapered down over the next 32 days.
The feeling like I was going to have my period any day disappeared a few days after the diarrhea began, BUT … throughout the diarrhea’s course, I continued, almost every evening, getting that menstrual feeling, albeit milder.
PROSTAGLANDINS!
Your health insurance should cover a colonoscopy, which is the only way to diagnose microscopic colitis. If you’re at least 50 and haven’t had one, get one.
Tell the doctor to swab for microscopic colitis. The joint aches of IBDs are called “enteropathic arthropathy.”
This situation is non-destructive, will eventually remit (though future flares are possible), and will NOT damage your joints or weaken them. I continue deadlifting heavy barbells and doing pull-ups without a problem.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
Sources:
mayoclinic.org/diseases-conditions/menstrual-cramps/basics/causes/con-20025447
webmd.com/women/guide/menstrual-pain
ccfc.ca/site/pp.asp?c=ajIRK4NLLhJ0E&b=6349433&printmode=1 (flare-up of joint aches can occur separate from gut problem flare-ups)
ncbi.nlm.nih.gov/pmc/articles/PMC3629156/ (prostaglandins and MC)
ncbi.nlm.nih.gov/pubmed/6350580 (prostaglandins and PMS)
ncbi.nlm.nih.gov/pubmed/19594490 (prostaglandins and IBD)
rheumatology.org/Practice/Clinical/Patients/Diseases_And_Conditions/Psoriatic_Arthritis/

Acid Reflux Can Affect Throat without Chest Burning

Don’t assume your throat issues can’t be acid reflux just because you have no heartburn, chest discomfort or abdominal pain.
My father was recently coughing for no apparent reason, and I suggested it might be acid reflux. He said it couldn’t be because he didn’t feel any burning in his chest or stomach.
I told him you could have acid reflux affecting the throat without feeling any burning in the chest.
Why can acid reflux cause throat related symptoms in the absence of chest or stomach related symptoms?
“On occasion acid reflux can cause throat symptoms with no burning sensation in the throat or chest,” says Dr. Jeffrey Fine, MD, the chief of gastroenterology at the Medical Surgical Clinic of Irving.
“This is referred to as extra-intestinal manifestations of gastroesophageal reflux disease (GERD).
“It can be a direct effect of acid refluxing all the way up into the throat from the stomach. GERD can be caused when esophageal and cricopharyngeal muscle disorders occur at the same time.”
One day I developed a cough—every few minutes something would tickle in the back of my throat and necessitate a cough. No other symptoms.
At the time, it didn’t occur to me that acid reflux was the only explanation.
But in retrospect, this had to be acid reflux, affecting only my throat and without heartburn or chest pain—triggered by extreme emotional duress.
This every-two-minutes need to cough developed a few days prior to having to literally chase after my beloved dog down a busy street, trying to catch up to him before he got hit by a car.
Actually, my parents owned him, but I was staying with them to give the dog his brain cancer treatment because my parents couldn’t handle the injections.
He was deranged from the disease and had gotten loose from the yard after the lawn care people left the gate open.
I was running through traffic since the dog was running through traffic. This was a German shepherd and I began losing distance.
Finally, I saw a man approaching from another direction who was trying to help.
Suddenly I got really close to my beloved furry angel and reached out to grab his collar, but he tried to bite me, causing me to retract.
Then I reached out for his collar and almost had him–he bolted off, even ignoring my father as my father pulled alongside the dog and opened the car door and called for him to jump in—something the dog always loved to do—but now, only ran away in his demented state.
I called out to the man who had joined in on the attempt to catch the large dog, “A hundred dollars if you can catch him!”
Within a minute, the man had the dog. (And I stuck to my word and paid him $100.)
I knew it was time to call the vet and have him euthanized; he had taken a rapid turn for the worse over the past few days—this coincided with development of my cough; my heart was just breaking—I was about to lose my golden love.
He no longer “knew” his family and was defecating in the house, spending hours pacing frenetically.
Throughout this course I had also suddenly developed a change in bowel habits that included frequent diarrhea and foul smelling and weird looking stools.
I couldn’t help but think colon cancer. I scheduled a colonoscopy, which turned out to be two days after the dog was put down.
The stress and anxiety were ridiculous. I’d be sitting there at my computer, coughing every two minutes, taking swigs of the almost-nauseating syrupy solution to clean my colon out for the exam.
Stress-induced acid reflux?
Acid reflux can cause a persistent cough — a throat symptom — without causing any heartburn, chest or abdominal discomfort. I had the cough all the way into the exam room.
When the colonoscopy was over, and the doctor said everything looked normal, and I began coming out of the sedation. The cough was completely gone. It never came back.
The diarrhea and abdominal rumbling turned out to be microscopic colitis, a benign condition not related to acid reflux.
If you have a nagging cough or other throat symptom like a hoarse voice, but no heartburn or chest pain, this might be acid reflux.
But to be sure, see a physician, since throat symptoms can have other, more serious causes.

Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Rocketclips, Inc

Can Excessive Burping Be Caused by Anxiety?

Though cancer can cause burping, this symptom can also be caused by psychological factors.
Anxiety can cause a LOT of symptoms, including headache, backache, stomach ache, a knotty feeling in the stomach, diarrhea, a racing heart, a fluttering heart, a lump feeling in the throat …
But what about belching?
Burping is associated with obnoxious behavior and eating too much, and with gulping air with a carbonated beverage.
But can anxiety actually cause one to burp?
“Yes. Anxiety can cause excessive burping,” says Dr. Jeffrey Fine, MD, the chief of gastroenterology at the Medical Surgical Clinic of Irving.
How does this happen?
“When people become anxious, they may swallow excessive amounts of air,” says Dr. Fine.
“This is called aerophagia. When this happens, air goes into the stomach and is then forced back through the esophagus and out of the mouth – more commonly thought of as burping.”

Freepik.com/katemangostar
The solution would be to make sure that your mouth is closed during periods of anxiety. But this tactic isn’t always easy to pull off, especially if the anxiety is of an acute and severe nature.
If you’re still burping, put yourself in a state of mind that induces relaxation and calmness, and see if it goes away.
For instance, settle down in your favorite piece of furniture with some soothing music, and focus on something that will distract your mind from anxiety, such as counting backwards by seven from 100; or counting each tick of the clock in the room.
Or repeat in your head your favorite poem or song lyrics over and over.
Do this for a while and see if the burping goes away.
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Aaron Amat

Can Acid Reflux Cause Bloody Stools?
Is it possible for acid reflux disease to cause blood to be in one’s stools?
“It is unlikely that acid reflux can cause blood on or in the stool,” says Dr. Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“To have blood on or in the stool, the patient would have to have massive gastrointestinal bleeding from the esophagus and this is unlikely.
“The only way acid reflux could cause blood in a patient’s stool is if they had an esophageal ulcer eroding into a blood vessel causing rapid gastrointestinal blood loss.
“When a patient has this condition, they are more likely to be vomiting blood than to see it in their stool.”
If you’re experiencing any unnerving symptoms, insist upon a colonoscopy, even if you’re under age 50.
A colonoscopy can rule out or in a number of conditions. Do not fear a colonoscopy.
If you haven’t had any peculiar symptoms but are at least age 45, it’s time to ask your physician about a colonoscopy as a screening for colon cancer.
The age for starting screening colonoscopies was changed to 45 by the American Cancer Society in 2018 — due to the rise in colon cancer diagnosis in people under 50.
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can Exercising on an Empty Stomach Cause Acid Reflux?
Are you wondering if that discomfort in your chest or stomach while working out on an empty stomach might be from acid reflux?
“Yes, exercising on an empty stomach can cause acid reflux,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
How does this happen?
“Exercising on an empty stomach can increase intra-abdominal pressure,” explains Dr. Fine.
“Anything that increases intra-abdominal pressure can overwhelm the lower esophageal sphincter (LES) and result in reflux.”
The symptom can linger for a while after the exercise is over.
Symptoms of Acid Reflux from Exercising on an Empty Stomach

The symptoms are those that are typical of acid reflux: a discomfort in the abdominal area that can be described as an ache, mild pain or burning sensation.
This feeling can also make its way to the chest area, including what seems to be below the sternum (the esophagus is right behind the sternum).
If you’re getting chest pain every time you exercise on an empty stomach, but not when you have some food in it, then yes, this can be acid reflux.
However, make sure you have a thorough exam with a cardiologist so that a cardiac cause can be ruled out.
For example, suppose you have a normal coronary calcium score (within five years of having the test).
Suppose also that your blood pressure and cholesterol profile are in the normal range.
And let’s also say that you don’t have diabetes.
Finally, you have not noticed any unusual shortness of breath or decline in physical abilities due to increased fatigue.
Given all that — chances are extremely high that the discomfort in your chest (and especially if it’s in your abdomen) is being caused by acid reflux if it comes only when you exercise on an empty stomach.
To help prevent this annoying problem, make a point of taking in some food prior to exercising.
This could be a little yogurt, some fruit, a hardboiled egg, a handful of nuts or any small helping of a healthful food so that your stomach isn’t completely empty.
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Gurgling from Stomach: Could this Be Acid Reflux?

Is that gurgling inside your stomach coming from acid reflux, cancer or what?
Now, gurgling from your stomach can be either annoying, embarrassing or scary (if you read somewhere that it could be a sign of cancer or even a brewing condition involving your heart).
Can Acid Reflux Cause a Gurgling Sound in the Belly?
“No — When your GI tract moves, it generally causes a gurgling noise,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“This is part of the natural digestive process and not due to acid reflux.”
What are the symptoms that acid reflux does cause?
The most common symptom of this very common condition is a burning or slightly abrasive feeling in the chest and/or upper abdomen.
However, the chest or abdominal discomfort from acid reflux isn’t always of a burning nature.
It can sometimes be described as a dull ache, strong ache or a pressure or heaviness.
The chest symptoms of acid reflux can mimic those of heart disease or of a heart attack.
Another common symptom of acid reflux is “burping” up a small amount of bitter tasting liquid after eating a meal — especially if you ate a lot of food in a short period of time.
The good news is that a gurgling stomach — either that which you can hear or only feel — is not cause for alarm.
The GI tract is supposed to move. The esophagus and intestines contract as part of the digestive process.
The esophagus and intestines are made of muscle, and muscle in the GI tract moves things along to get food digested. This movement is called peristalsis.
If you hear it, that’s normal. Whose stomach doesn’t gurgle sooner or later?
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}