

What Does Pus Coming out of a Mole Mean?

This can mean melanoma, but a mole oozing pus can also have a benign cause.
“Pus or even infection in a mole is not in itself a sign of melanoma,” says Dr. Rebecca Tung, MD, a
“People can have an acne cyst at the same location as a mole — causing it to swell or become infected.
“Because some skin cancers produce unusually fragile skin which can be easily traumatized, they can become infected and produce pus.
“If your mole is behaving weirdly, a quick checkup with the dermatologist can help sort out if skin cancer is present or not.”

Melanoma. Laurence Meyer, MD. cancer.gov
The Acne Cyst
Acne cysts are deep, sometimes painful, and swollen nodules that can form when hair follicles become clogged with excess oil and dead skin cells.
The pus in acne cysts is usually thick, yellowish or white. It’s a collection of dead white blood cells, bacteria and cellular debris.
It can feel semi-solid or gel-like, and it may be under pressure, contributing to the pain and swelling of the cyst.
The pus can vary in color, ranging from white to yellow, depending on the stage of the infection and the presence of different types of bacteria.
It’s easy to see that is all of this is coincidentally occuring alongside a mole, or the irritated follicle just happens to be inside the mole, that it can make a person wonder if it’s melanoma.
Do not delay getting a mole, that seems to have pus coming out of it, examined by a dermatologist — who is better qualified than a general practitioner to inspect the spot.
A dermatologist is more equipped than a general practitioner to assess unusual moles.
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/New Africa

Scratch Mole, It Bleeds: Melanoma?

Do you have a mole that bled after you scratched it and are now fearing it’s melanoma, the deadliest skin cancer?
“If a mole that is scratched bleeds, this may signify skin cancer,” says Dr. Rebecca Tung, MD, a
In some melanomas (skin cancer), the architecture of the skin is abnormal and the skin is unusually fragile, leading to easy bleeding from only minor trauma.
“While it is possible to make any skin lesion bleed if it is scratched aggressively, a mole that bleeds from only minimal irritation deserves to be looked at by a dermatologist to determine if it is okay or needs further evaluation with a skin biopsy.”
I thought that the malignant cells of melanomas were so “sticky” that it would require quite a bit of trauma to shear the structure enough to cause bleeding. Dr. Tung explains:
“Skin cancers that grow rapidly typically have significant blood supply.
“These close to the surface vessels can be provoked to easy bleeding with only minimal skin trauma like scratching or rubbing.”
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/LightField Studios

When Should You Stop Getting New Moles?

Over age 40 and noticing what appear to be new moles growing on your skin?
“People in the 40-50 age bracket may begin to get scary looking pigmented growths called seborrheic keratoses — which are perfectly harmless and are a part of the aging process,” says Dr. Rebecca Tung, MD, a
“Freckles (which are also benign) may also come up over the course of a lifetime, especially if the person has significant sun exposure.
“Generally speaking, a new mole which crops up in an adult should be evaluated.”
A seborrheic keratosis (skin barnacle) can easily pass as a mole. I had one on my back for the longest time and had always believed it to be a mole. It was part of my routine visual skin inspection.
Then one evening I noticed it had changed in appearance. This alarmed me like mad—because all that time, I had thought it was a mole.
I was scared out of my wits and next day made an appointment with a dermatologist.
Her first words, after she took a look at it, was, “I don’t think it’s a mole.” She said it was a seborrheic keratosis.
I had it removed for biopsy anyways, and the result, indeed, came back as a seborrheic keratosis.
Nevertheless, don’t assume that the “new mole” might be a harmless skin barnacle.
People are not supposed to get new moles (as in nevi) as they get older. Have the spot checked by a dermatologist.
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Motortion Films

Can an Itching, Bleeding Mole Be Benign?

You’re not a hypochondriac if you fear that an itching, bleeding mole might be melanoma rather than benign.
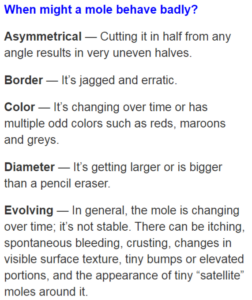
“While people are familiar with the ABCD’s of mole evaluation- – Asymmetry (one half of the mole does not resemble the other half), Border irregularity (jagged or scalloped), Color changes (the mole has gained or lost pigmentation), Diameter growing (growth in size) — the E factor (evolving), which encompasses itching, bleeding and any other change, can also signal skin cancer,” explains Rebecca Tung, MD, a
“Seeing a dermatologist can help determine what is going on with the mole in question.
“Sometimes people may shave or traumatize a benign mole, leading to symptoms of bleeding and itching.
“However, an evaluation will help to shed light on whether the mole is harmless or requires a skin biopsy to make certain it is not cancerous.”
Dr. Tung’s specialties include general dermatology with skin cancer surveillance, moles, melanoma, surgery (Mohs micrographic, laser, skin cancer reconstruction) and cosmetic dermatology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/dean bertoncelj

Do You Have Chest Pain in Different POSITIONS?

Positional chest pain can be due to a variety of causes including heart problems, says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
Positional chest pain isn’t always caused by acid reflux or costochondritis.
“Typically, chest pain associated with deep inspiration [inhaling] or lying flat may be indicative of pericarditis or an inflammation in the lining of the heart,” says Dr. Stevens-Cohen.
“Patients usually get relief with sitting up or forward. The sitting forward allows the lining of the heart (layers) to separate and provides relief.”
The esophagus is right behind the sternum. “Esophageal spasms or GERD may be some GI reasons for having positional chest pain,” continues Dr. Stevens-Cohen. “GERD may increase at night and cause pain.”
Avoid eating fewer than three hours before bedtime to see if this relieves GERD (acid reflux) related chest pain.
“Musculoskeletal (chondritis) is also positional and can be reproduced by touching the affected area.”
This kind of chest pain (also called costochondritis) can hurt quite a bit and can be caused by lifting weights.
“Pleurisy-inflammation in the lining of the lung can also cause positional pain. Localized inflammation.” This worsens with coughing and inhaling.

Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/New Africa

Heart Palpitations Lasting Daily, Sometimes Hours
What’s going on when heart palpitations persist for hours almost every day?
“Some people use the word [palpitations] to describe a fast or rapid heart rate; others to note an irregular heart rate,” says Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
“Non-cardiac causes may include thyroid disease, anxiety, hormonal imbalance, high blood pressure, pulmonary issues, GERD/reflux.”
I’ll confess that I once felt heart palpitations within seconds after beginning to read an article about…none other than heart palpitations.
The power of suggestion can be very powerful. After I realized how crazy this was, the symptom vanished.
I also experienced that attention-getting thumping heartbeat when I logged onto my e-mail and saw a message from someone — a message I was expecting — and I knew that the news might be very terrible (turned out it wasn’t).
But while I was waiting for the message to open…my heart was just thumping in a PVC type of way.
I don’t mean racing due to adrenaline…but what actually felt like palpitations from PVCs. Both of these incidents were extremely transient and precipitated by anxiety.
Dr. Stevens-Cohen further explains, “If symptoms persists or occur daily, or if they interfere with daily activities including exercise regimen, it’s time to see a physician and be referred to a cardiologist.
“There are some conditions — valvular heart disease (mitral valve prolapse or mitral stenosis) that are associated with palpitations.
“The most important diagnostic tests utilized are an echocardiogram (looking for structural heart disease) and an event or Holter monitor.
“The key is to catch the palpitations on a monitor so we can know if rhythm is dangerous or warrants further treatment.”
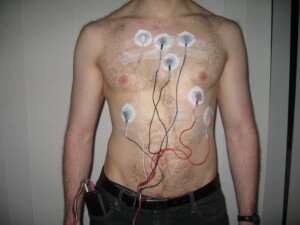
Holter monitor. Jason7825/en.wikipedia
A normal echocardiogram means that the palpitations you feel are benign.
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Ejection Fraction 20%: How Long Can You Live?

An ejection fraction of under 20 percent is frightfully low as far as survival…or is it?
“Having a low ejection fraction (absolute number) is not necessarily correlated to symptoms,” begins Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
“For example, a person with an ejection fraction of 40 may be more symptomatic than one with an ejection fraction of 15.
“However, having systolic heart failure with an ejection fraction < 35, there is an increased mortality related to poor cardiac output and arrhythmias.
“Medication and ICD therapy when indicated may help manage symptoms and prevent arrhythmias; however, the mortality is still high.”
ICD stands for implantable cardioverter defibrillator.
“The biggest correlation with heart failure deaths is related to hospital admissions and renal failure/injury.
“Patients with renal failure and more than three hospitalizations in one year may have a mortality rate (one year) of >50 percent.”
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Rocketclips, Inc.

Can CoQ10 Help PVC’s?

CoQ10 is one of the best antioxidant supplements, but how does it work against PVCs: premature ventricular contractions?
For this article I asked Pilar Stevens-Cohen, MD, FACC, Department of Cardiology, South Nassau Communities Hospital.
This is what Dr. Stevens-Cohen explains:
“Coenzyme Q is a powerful antioxidant that improves oxygen utilization.
“It may help with high blood pressure but has also been reported as causing palpitations. By itself, it is not a known treatment for palpitations.”
PVCs, though frightening, are often just benign premature beats that make it seem as though your heart is skipping a beat or inserting an extra beat.
If you’re worried, see a cardiologist, who will probably order an echocardiogram and will also have you undergo an EKG.
Dr. Stevens-Cohen is board certified in cardiology, nuclear cardiology, echocardiography and internal medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/OBprod

What Does Frequent Nausea with IBS Mean?

It is no secret that irritable bowel syndrome (IBS) can lead to nausea, but what should a sufferer do?
In fact, nausea that’s caused by irritable bowel syndrome isn’t even uncommon, says a doctor.
*****
“IBS is a condition that affects the function of both the upper and lower GI tract, so it would not be uncommon to see nausea, bloating or other upper GI symptoms with IBS, as they can all be related to abnormal gastrointestinal function,” explains Michael Blume, MD, a gastroenterologist at MedStar Good Samaritan Hospital, Baltimore.
“That being said, there are many problems that cause nausea, so while this can be seen with IBS, it is important not to get ‘tunnel vision’ and not consider other possibilities.”
This is especially true if you’re over age 50. Even 40. But even in younger people, unexplained nausea or stomach aches, constipation and/or diarrhea, need to be evaluated by a gastroenterologist.
Sometimes, nothing comes up in the test results. IBS is a diagnosis of exclusion, and if the patient then undergoes treatment for this disorder, and the nausea and other symptoms subside, then the diagnosis was likely very accurate.
If you’re having unexplained nausea and have been diagnosed with IBS, but the symptoms persist despite treatment…and especially if the symptoms are becoming progressive in some way and you’re a woman…then see a gynecologist about having your ovaries checked.
Ovarian and other gynecological conditions can cause symptoms that seem like they are digestive in origin.
Remember, cancer (which can cause nausea) can occur alongside IBS, though there is no causal relationship.
Another Condition Similar to IBS; Can Sometimes Cause Nausea
The benign condition of microscopic colitis is sometimes misdiagnosed as IBS.
However, in microscopic colitis, there is no constipation; it’s all diarrhea–and usually watery and “explosive.”
But there may be nausea and painful cramps, too. Only a colonoscopy can diagnose microscopic colitis.
If you’ve been diagnosed with IBS, have not had a colonoscopy, sometimes have nausea, and suffer only from diarrhea — there IS a chance you might actually have microscopic colitis.
 In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/KDdesignphoto

Can IBS Cause Severe Backaches and What’s the Remedy ?

Just what causes that backache from your irritable bowel syndrome?
Back pain is perhaps the world’s leading nonfatal health problem.
It affects millions of people, causing significant discomfort and impacting daily life.
The causes can range from poor posture to injury or chronic conditions — to a simple pulled muscle to PMS to fibromyalgia to multiple sclerosis to a pinched nerve to cancer metastases involving the spine.
That last cause, as scary as that is, is not at the top of the list for common causes of back pain.
Irritable Bowel Syndrome’s Connection to Back Pain
- The question isn’t if IBS can cause backache.
- The question is just how does this happen, and what can be done to remedy it?
“Colitic pain (usually crampy pain relieved by having a bowel movement or passing gas) can often be felt in the back,” explains Michael Blume, MD, a gastroenterologist at MedStar Good Samaritan Hospital, Baltimore.
“This represents a phenomenon called referred pain, and reflects the innervation of your colon.
“In short, it is how you are wired together. You treat the back pain by treating the IBS.”
Before you attribute your back pain to IBS, first make sure that you have IBS.
Don’t assume it just because other family members were diagnosed and/or your symptoms are a perfect match to this condition.
IBS is a diagnosis of exclusion, meaning, there is no test for this disorder. It is diagnosed when all other tests are negative.
This includes a colonoscopy. Even young adults with IBS-like symptoms should still undergo a colonoscopy to rule out other causes for the bloating, cramping, diarrhea, constipation and back pain.
A benign inflammatory bowel disease called microscopic colitis causes symptoms very similar to that of irritable bowel syndrome.
This includes back pain in a small percentage of MC patients!
Treatment of MC differs from that for IBS. This is why a colonoscopy is so important.
This procedure can also detect other conditions that can cause symptoms that mimic those of IBS that also cause back pain. Colon cancer, however, is very rare in people under 40.
In practice for 25+ years, Dr. Blume treats over 65 conditions including abdominal pain, appetite loss, blood in stool, celiac disease, colon cancer, esophageal and liver disease, gas and IBS.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}