
How Long Should Chest Pain Last Before Going to the ER?
How long should you wait with chest pain before deciding it’s time to visit the ER?
After all, you could be in that 15-30% of patients who end up having a heart attack.
“It’s important to have a pretty low threshold for having chest pain evaluated if it does not have a clear cause, such as injury or unusual exertion,” says Christopher J. Hanifin, PA-C, who was previously a physician assistant in open heart surgery with Cardiothoracic Surgery of South Bend in South Bend, IN.
“Musculoskeletal pain can develop in the chest just like in the rest of the body. For example, the prolonged coughing associated with a cold or the flu can lead to chest pain.”
You have muscles and other soft tissue in your chest. They are not immune from feeling strained or achy after mechanical exertion.
Waiting Time with Chest Pain Before Going to the Emergency Room
“Chest pain in a person with risk factors for cardiovascular disease should be promptly evaluated,” says Hanifin.
“People with a history of high blood pressure, smoking, diabetes, high cholesterol or a family history of heart diseases need to be educated regarding the warning signs of heart attack.
“Another red flag for chest pain is the presence of associated symptoms. The presence of shortness of breath, nausea, sweating or lightheadedness can signal a potentially life-threatening problem and merit prompt evaluation.
“Finally, different types of pathology are frequently characterized by different types of pain.
“Heart attacks and angina are usually associated with a pressure sensation.
“Aortic dissection is associated with a tearing sensation, and inflammation around the heart – pericarditis – is associated with a sharp pain. All of these should be urgently evaluated.”
This means don’t make up some time limit rule. Just get out the door (hopefully someone will be able to drive you to the emergency room).
Study: correlation between how long chest pain lasts and whether or not it’s a heart attack?
Researchers from Henry Ford Hospital decided to investigate. The study notes that about 15 to 30 percent of chest pain cases in the ER turn out to be a heart attack.
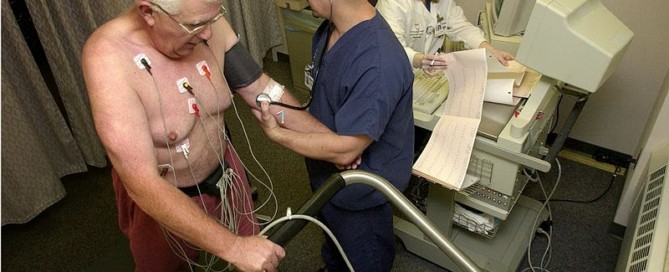
The paper points out that an electrocardiogram is “not 100 percent accurate,” though this, and a troponin blood test, are important to ER physicians in evaluating for a possible heart attack.
The study involved 426 patients with chest pain and a 30-day follow-up. Out of that, 38 were diagnosed with a heart attack.
Average duration of chest pain was 120 minutes for them. It was 40 minutes for patients who did not have a heart attack.
For patients who had chest pain for under five minutes, there were no heart attack diagnosis.
Conclusion
The report says that those with chest pain lasting under five minutes “may be evaluated as an outpatient” by a cardiologist.
But if chest pain lasts longer than five minutes and does not have a clear cause (such as diagnosed acid reflux), a person should “seek prompt medical evaluation in an emergency department.”
However, what if only one minute into your chest pain, you also feel nauseous, faint and are breaking into a sweat?
Though these symptoms can be caused by a panic attack (which doesn’t require an emotional trigger), they are far more meaningful within the context of a person at high risk for a heart attack:
- Over age 50
- Obese
- Smoker
- Diabetic
- Sedentary lifestyle
- High sodium diet, among other risk factors
Take things into context. A 60-year-old, nonsmoking, fitness enthusiast of healthy weight and other vitals who regularly runs and lifts weights is more likely having a panic attack than is a 40-year-old, smoking, non-exercising, overweight person whose father had a heart attack at age 42.
This study was small and further investigation is warranted. The full report is in the Sept. 2013 Critical Pathways in Cardiology.
Never think that you’ll be wasting an ER doctor’s time with your chest pain complaint as you try to convince yourself it’s only gas or a strained muscle.
When in doubt, go to the ER, especially if you have risk factors for a heart attack.
 Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University, NJ.
Christopher J. Hanifin, PA-C, is currently Department Chair and Assistant Professor, Department of Physician Assistant, Seton Hall University, NJ.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: sciencedaily.com/releases/2013/09/130911161006.htm

High Calcium in Arteries Linked to High Heart Attack Risk

The higher the calcium in your arteries (shown by a calcium score test), the likelier you’ll suffer a heart attack.
Maybe it’s time to get your calcium score!
Researchers may be able to predict future severe cardiac events in patients with known, stable coronary artery disease (CAD) using coronary calcium scoring, according to a study published in the online edition of Radiology.
“The amount of calcium in the coronary vessels, as measured by CT, is of high predictive value for subsequent serious or fatal heart attack in these patients,” says Marcus Hacker, MD, “independent of the patient’s age, sex and other coronary risk factors.”
Dr. Hacker is lead study author, and resident physician in the Department of Nuclear Medicine and leader of the research unit for nuclear cardiology at Ludwig Maximilians University in Munich, Germany.
According to the National Heart, Lung and Blood Institute, CAD is the leading cause of death in the U.S. for both men and women, killing more than 500,000 Americans each year.
Single photon emission computed tomography (SPECT) myocardial perfusion imaging is a nuclear medicine diagnostic procedure that provides excellent 3-dimensional images of coronary arteries to assist in diagnosis and treatment of CAD.
Currently, calcium scoring – measuring the amount of calcium in the arteries – is used as a screening exam and in cases of suspected CAD, but not in cases of known CAD.
Dr. Hacker and colleagues set out to determine if calcium scoring would lend additional prognostic value to SPECT findings in patients with known, stable CAD.
For the study, 260 patients with CAD underwent coronary artery calcium scoring in addition to SPECT myocardial perfusion imaging.
Over a median period of 5.4 years, the patients were followed up for severe cardiac events.
Twenty-three of the 260 patients had a fatal or severe heart attack, and 40 additional patients underwent bypass surgery.
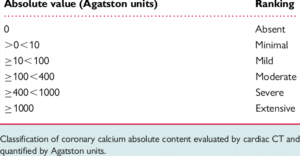
The results showed that patients with an initial calcium score greater than 400 were at significantly increased risk for severe cardiac events.
“We found that coronary calcium seems to play an important role in predicting subsequent heart attack or sudden cardiac death,” and this adds prognostic value to SPECT findings, says co-author Christopher Uebleis, MD, member of the research unit for nuclear cardiology at LMU.
Dr. Hacker pointed out that combining calcium scoring and SPECT can help identify patients with known CAD who are at highest risk for serious or fatal heart attacks.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sukiyaki
Source: thefreelibrary.com/High+calcium+level+in+arteries+’signals+heart+attack+risk’.-a0204641880
Women’s Heart Disease: Stress, Stiff Heart, High Blood Pressure
Don’t kid yourself: Women’s heart disease is very different from men’s in more ways than you may be thinking, and that includes the effect that stress has on the heart.
Dr. Gordon A. Ewy, MD, explains how women’s heart disease differs from men in the causation of stress, stiff cardiac muscle and high blood pressure.
Maybe you already know that women’s heart disease is a different animal than is men’s, but perhaps you don’t know that mental stress and high blood pressure play a much bigger role in women’s heart disease than they do in men’s. Also relevant is that of stiff cardiac tissue.
Stress and Heart Disease in Women
“Stress often triggers heart dysfunction in women,” says Gordon A. Ewy, MD, in an article he wrote for the University Sarver Heart Center newsletter (spring, 2010).
Dr. Ewy is the Director Emeritus of the University of Arizona Sarver Heart Center.
“Clinical observations of how some individuals experience severe stress or respond unusually to minor stress, have led to our understanding of a condition now called ‘stress cardiomyopathy,’” continues Dr. Ewy in his article.
He adds that most studies show that more than 90 percent of patients who have stress cardiomyopathy are women.
This condition is associated with high levels of the “fight or flight” hormone adrenalin, plus an irregular or fast heartbeat.
This stress-induced form of cardiac ailment, says Dr. Ewy, is reversible in most cases, though he also says in his article, “Tragically, the condition may result in sudden death in the most extreme cases – ‘She was scared to death.’”
Stiff Cardiac Muscle and Women
Dr. Ewy’s report continues, “Heart failure in women is often due to an abnormally stiff heart muscle.
“The heart contracts as it should, but is too stiff to relax normally and requires a higher amount of pressure to fill the major pumping chamber.
This higher pressure backs up into the lungs, resulting in symptoms such as shortness of breath, especially with exertion.”
Women should engage in structured aerobic exercise to help prevent this stiffness from developing.
High Blood Pressure and Women
“Hypertension (high blood pressure) is more common as one gets older, and if inadequately treated, often leads to heart failure due to an abnormally stiff heart, a syndrome more common in women since they tend to live longer than men,” says Dr. Ewy in the report.
What can women do to prevent heart disease?
The article explains, “First, the classic risk factors of high blood pressure, abnormal lipids, diabetes and others, which are often hereditary, need to be addressed.”
He urges a healthy diet, weight control, exercise and avoiding smoking/secondhand smoke.
 In the area of research, Dr. Ewy has made significant contributions to the defibrillation and resuscitation of patients with cardiac arrest. He is board certified in internal medicine and cardiology and has authored over 400 publications in medical journals.
In the area of research, Dr. Ewy has made significant contributions to the defibrillation and resuscitation of patients with cardiac arrest. He is board certified in internal medicine and cardiology and has authored over 400 publications in medical journals.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: heart.arizona.edu/news-info/documents/SHC57_h-is-for.pdf
CT Angiography vs. Stress Test for Heart Disease Detection

New research shows that the stress test is not effective at detecting obstructive heart disease, and that the CT angiogram wins considerably.
The CT angiogram wins out over the cardiac stress test when it comes to detecting blockages in coronary arteries that can necessitate medical intervention such as bypass surgery.
Beaumont Health System cardiologists led an investigation, and the report is in the Feb. 14, 2012 Journal of the American College of Cardiology.
A CT angiogram is an imaging study of blood vessels using a CAT scanner. The CT angiogram is non-invasive, as is the cardiac stress test.
If serious coronary blockage is detected via either of these means, the next step is the cardiac catheterization procedure, which is highly invasive.
My mother had this performed, and the consent form included generous language describing possible risks, which include heart attack and stroke.
The cath procedure is the gold standard for identifying coronary artery blockage (severe heart disease), but something must lead to this procedure in the first place.

Catheter angiogram. Shutterstock/MAD.vertise
In the case of my mother, an “abnormal” echocardiogram was the preceding test; her cardiologist skipped the CT angiogram and stress test altogether.
However, usually, it’s a stress test or CT angiography that precedes.
The Beaumont study showed that the CT angiogram is very effective at detecting obstructive heart disease (blocked arteries) — to the point that the patient must then undergo the cath procedure.
The study also showed that stress tests were not effective.
The Beaumont study examined 6,000 patients who underwent CT angiograms after a stress test.
“We concluded that CT imaging works very well as a ‘gatekeeper’ to the catheterization lab, and can help rule out patients who don’t require invasive coronary angiography,” says Kavitha Chinnaiyan, MD, Beaumont’s director of Advanced Cardiac Imaging Education, in a press release on the Beaumont Health System Web site.
The Beaumont study says that up to 10 percent of stress tests are inconclusive, and thus, lead to the risky cath procedure, which then often turns out to reveal no blockages.
The National Cardiovascular Data Registry of 400,000 patients reports that obstructive heart disease is present in only one third of patients undergoing the cath procedure (also known as invasive cardiac angiography).
The Beaumont study showed that stress tests failed to predict coronary artery obstruction.
The CT angiogram (i.e., with the CAT scanner) correlated nicely with the cath procedure findings, but the cardiac stress test did not.
“Our study shows that CT angiography can help to identify patients who need expensive, invasive testing, especially in patients with inconclusive stress test results,” says Dr. Chinnaiyan in the press release.

Dr. Chinnaiyan has authored and co-authored 100+ manuscripts and abstracts. She has served as the Chair of the Board of Directors of the American Heart Association of Southeast Michigan.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Source: beaumont.edu/news-story-beaumont-health-system-research-coronary-ct-imaging-predicts-need-for-heart-catheterization

Calcium Score Getting Higher Means Big Heart Attack Risk

If your coronary calcium score gets higher with each subsequent test, you have every reason to be very alarmed.
How many coronary calcium tests have you had, and has your score gotten higher each time?
If so, this should be great cause for concern, says a study that appears in the Journal of the American College of Cardiology.
I had my coronary calcium score test done in June 2011, and my score was zero (meaning, no detectable hard plaque in my arteries).
The “warranty” on this is good for five years, said my cardiologist.
I had the procedure because my mother’s emergency quintuple bypass surgery rattled me.
But what about people who have serial coronary calcium scans, and find that their number keeps getting higher and higher?
The study says these patients are over six times more likely to have a heart attack or succumb to heart disease than are people who don’t have an increasing calcium score.
The study recommends that for people with measurable plaque in their arteries, they should have more frequent tests.
The researchers, who analyzed serial calcium scoring in over 6,700 patients, found that the six-times increased risk of cardiac events was independent of other risk factors for coronary artery disease.
“We have known that coronary artery calcium can be related to heart disease,” says Matthew Budoff, MD, “but this study shows the progression of accumulation of the calcium in the arteries can be a significant factor in evaluating the risk that a patient may suffer a heart attack in the future.”
My calcium score test was not covered by my insurance.
I had it done at an independent cardiac imaging clinic.
I don’t recall the cost, but it can vary from $200 to $400.
The test takes five minutes or so.
You simply lie on a bed, with your chest and head inside a donut shaped piece of equipment (CT scanner) while it scans your heart. No contrast dye or injections are used.

Dr. Budoff is at the forefront of the medical community’s efforts to create early detection methods for coronary heart disease.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes
Source: sciencedaily.com/releases/2013/05/130502142657.htm
Chest Pain, ER Visit: Follow-Up within 30 Days Is Critical
You’re not out of the woods if a doctor discharges you from the emergency room after you reported chest pain.
It may be a matter of life or death that you follow up within 30 days of your ER visit, even if all tests were normal.
“Many patients who present to the emergency department (ED) with chest pain have risk factors for heart disease,” says Geoffrey Barnes, MD, cardiologist and vascular medicine specialist at the University of Michigan Health System.
“So even if your tests in the emergency department are normal, it’s a good idea to check in with your primary care provider or a cardiologist shortly after your ED visit.
“This is a great time to discuss what may be causing your symptoms, identify risk factors for heart attack, and discuss ways to reduce your chance of a heart attack, stroke or other blood clot in the future.”
Seeing a cardiologist within 30 days of an ER visit for chest pain lowered the risk of a heart attack or mortality among high risk patients — according to a study report in the journal Circulation.
A high risk patient, as defined by this study, was one with previously diagnosed diabetes or heart disease.
A discharge from the ER doesn’t mean your heart is fine.
If a patient presents with symptoms that are classic for a heart problem (chest pain, shortness of breath), that patient will undergo tests that determine if they had a recent heart attack, and if they are currently having a heart attack.
They will not receive tests that determine their risk of a near-future heart attack.
How do I know this? I’ve taken my mother to the ER several times when she complained of suspicious symptoms including chest pain.
I know the routine: troponin test, chest X-ray, EKG, blood pressure monitoring, heart rate monitoring and stethoscope exam.
None of these tests can accurately indicate propensity for a near-future heart attack; my mother’s EKG was non-concerning, but she soon after needed a quintuple bypass.
This is why it’s so important for that within-30-day follow-up.
Though being discharged from the ER has a reassuring ring to it, it’s still crucial to follow up with your provider within 30 days to lower the risk of premature death.
Even if the emergency room physician doesn’t make a point of rearranging the follow-up care, this doesn’t mean the patient should be passive.
They need to be proactive and arrange that follow-up themselves.
Study Findings
Over 56,000 patients with chest pain were analyzed. Variables like gender, age and health status were accounted for.
– Seventeen percent of high risk chest pain patients were seen by a cardiologist within one month of their ER visit; and 58 percent saw a primary care doctor. One-quarter had no follow-up.
– Patients who saw a cardiologist were 21 percent less likely to suffer a heart attack or die within 12 months, and the figure for those who saw a primary care doctor was 7 percent, compared to those who had no follow-up.
– People who saw a cardiologist underwent more extensive exams within 100 days of their discharge from the ER and had the most favorable health outcomes.
– One year out: Patients who saw a cardiologist were 15 percent less likely to suffer a heart attack or die, compared to those who sought a follow-up with a primary care physician.
The study focused on only high risk patients and thus, the results may not be applicable to other demographics with chest pain. Further investigation is warranted.
 Geoffrey Barnes, MD, is a cardiologist and vascular medicine specialist at the University of Michigan Health System and spokesperson for the World Thrombosis Day Campaign. Dr. Barnes’ clinical interests include treatment of vascular disorders, anticoagulation and general cardiac care.
Geoffrey Barnes, MD, is a cardiologist and vascular medicine specialist at the University of Michigan Health System and spokesperson for the World Thrombosis Day Campaign. Dr. Barnes’ clinical interests include treatment of vascular disorders, anticoagulation and general cardiac care.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Thumping Heart, Chest Pain, Dizziness, Fatigue: Serious Cause

The following symptoms together strongly indicate a serious heart problem: “thumping” heartbeat, dizziness, chest pain and fatigue.
Even three out of the four can suggest this serious problem with the heart: aortic stenosis.
Though these symptoms can be caused by more than one medical condition, one of those conditions is aortic stenosis — which requires surgery if the patient wants significantly improved long-time survival odds.
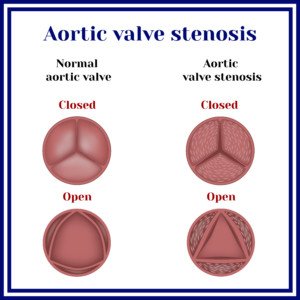
“Aortic valve allows blood flow from the left ventricle (main pumping chamber of the heart) to the aorta for distribution to various organs,” says Asim Cheema, MD, who’s board certified in internal medicine, cardiovascular diseases and interventional cardiology by the American Board of Internal Medicine. Dr. Cheema is with Your Doctors Online, an online doctor chat site.
“Aortic stenosis causes two problems,” continues Dr. Cheema. “On the left ventricular side, it increases the amount of work for the left ventricle, transmitting increased pressures to the left atrium and pulmonary vessels.
“On the downstream side, the effective blood flow to the body organs including coronary arteries is reduced.
“As a result, patients can have angina (reduced coronary flow), arrhythmia (increased pressure on the atria), shortness of breath (increased pressure in the pulmonary vessels) and low energy/fatigue/poor exercise tolerance due to decreased blood flow to muscle and body in general.
“The left ventricle may eventually become unable to generate enough pressure to push blood through the narrow valve and fail, causing heart failure.”
Source: Shutterstock/Mrs_Bazilio
Treatment of Aortic Stenosis
If you have the symptoms of chest pain with dizziness, fatigue, shortness of breath, a thumping sensation, etc., see a cardiologist immediately for a proper diagnosis.
Open heart surgery isn’t the only treatment option. There is a less invasive procedure that uses the Medtronic CoreValve® System.
A surgeon threads a catheter into the patient’s groin and up to the heart; the catheter deploys the device and places it, where it takes over the diseased valve’s function — allowing more normal blood flow throughout the body, ending the symptoms of chest pain, thumping heartbeat, fainting or dizziness, shortness of breath, fatigue, etc.
Though in isolation, a sensation of a thumping heartbeat is most likely benign, the index of suspicion soars when it’s coupled with chest pain and especially additional symptoms like dizziness.

Your Doctors Online offers a free 7 day trial where you can ask a doctor questions online and get answers in minutes from anywhere 24/7. Learn more here. Dr. Cheema teaches and provides supervision to graduate students at the Institute of Medical Sciences, University of Toronto.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can Too Much Milk Raise Your Calcium Score?

Find out what the latest research says about calcium intake and heart disease.
Milk is rich in calcium, and calcium deposits correlate to degree of heart disease, says Mayoclinic.com.
A calcium score of zero means no measurable coronary plaque buildup. I had my calcium score taken 17 months ago and it was zero, and since then (as has always been), I’ve been drinking up my milk.
A new study from the Institute for Aging Research at Hebrew SeniorLife concludes that there is no evidence of an association between calcium intake (which of course would include milk) and coronary artery calcification.
This is good news for milk drinkers such as myself, but also for people who take calcium supplements. The report is in the Nov. 7, 2012 American Journal of Clinical Nutrition.
The paper reports that subjects who had the greatest intake of this mineral (either from diet or supplements) had the same coronary artery calcium score as did subjects with the lowest intake of the mineral.
The report reminds people that the calcium score is very representative of the severity of calcified plaque buildup in coronary arteries.
The higher the score, the more plaque buildup, and in turn, the higher the likelihood of severe heart disease and a near-future cardiac event such as a heart attack.
“There was no increased risk of calcified arteries with higher amounts of calcium intake from food or supplements,” explains lead study author Elizabeth (Lisa) Samelson, Ph.D., associate scientist at IFAR.
The results of this study contradict the concerns in recent years that use of the supplements can raise the risk of heart attack.
The Institute of Medicine concludes that clinical trials do not provide evidence of this.
So the latest, then, is that you can feel safe drinking milk or having milk with your cereal.
Dr. Samelson does add, however, that for those wanting to take supplements, they should discuss appropriate doses with their physician.
If you’re concerned about your heart health, you can be very proactive by having your calcium score taken.
The procedure takes about five minutes, and as a screening tool, it likely will not be covered by your medical insurance.
The cost is anywhere from around $200 to $400. Don’t keep putting this off because of the cost.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources:
sciencedaily.com/releases/2012/11/121107145931.htm
mayoclinic.com/health/heart-scan/MY00327
Can Cozaar Drug Shrink Aortic Aneurysm in Non-Marfan Patients?

Since the Cozaar drug significantly shrinks rate of aortic aneurysm growth in Marfan’s patients, how well could it work for patients who do not have Marfan syndrome?
An aortic aneurysm is an abnormal enlargement of a portion of the aorta.
Though this potentially fatal feature is common in Marfan’s syndrome patients, it can also occur people without this genetic condition.
“Cozaar (losartan) is in the category of angiotensin receptor blocker used for hypertension,” says Michael Fiocco, MD, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“It has been found to blunt the effects of a protein that likely leads to aortic dilatation specifically in Marfan’s patients,” says Dr. Fiocco.
“This protein has not been found to be causative in other types of aortic aneurysms, i.e., atherosclerotic, aortopathy associated with bicuspid valves, etc. The research is ongoing.”
In the meantime, those with Marfan syndrome need to know about Cozaar.
Reducing the rate of aneurysm enlargement is not the same as shrinking these ballooned areas of the aorta.
A study showed that the rate of aneurysm growth in Marfan’s patients, after three years of treatment with Cozaar, was significantly reduced when compared to Marfan’s patients who were not given this drug.
The lead researcher of the Amsterdam-based study was Maarten Groenink, MD.
Marfan’s syndrome affects connective tissue. In many patients it causes progressive enlargement of the body’s largest blood vessel, the aorta.
As the aorta gets bigger (think a balloon expanding as it fills with air), its walls get weaker (the balloon’s walls become so thin that it bursts).
When the aortic walls are thinned out and weakened enough, the aneurysm can rupture or dissect. Death can occur in minutes.
People without Marfan’s syndrome can also have an aortic aneurysm.
How is an aortic aneurysm treated?
Surgical repair is the treatment — when the enlargement reaches a critical size — to prevent a rupture.
Otherwise, a surveillance approach is used, combined with medication to prevent high blood pressure, and restrictions on lifting weight.
There are no known drugs that can outright shrink an aortic aneurysm, and besides, shrinking the enlarged portion of the vessel wouldn’t necessarily mean that the walls would regain their original strength and durability.
Cozaar Study Results
The Amsterdam study showed that in patients who received Cozaar, the increase in aortic root enlargement over three years was 0.77 mm; in the control group it was 1.35 mm.
Plus, 50 percent of the Cozaar group showed no increased enlargement, yet only 31 percent of the control group had no enlargement.
These are striking results that show that the drug Cozaar has an inhibiting effect on the rate of aortic aneurysm growth in Marfan’s patients.
Hopefully, this research will continue and include non-Marfan’s patients with this condition.
NOTE: These results pertain only to enlargement of the “root” of the aorta, the area in Marfan’s that’s usually affected.
The study revealed that the drug did not significantly reduce growth rate of aneurysms elsewhere in the thoracic aorta.
The report points out that in no way does Cozaar postpone or prevent a ruptured aneurysm or even postpone or prevent prophylactic surgery.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Sebastian Kaulitzki
Source: sciencedaily.com/releases/2013/09/130902101857.htm

Can Exercise Cut Esophageal Cancer Risk?

Esophageal cancer has a very poor prognosis; certainly there HAS to be a way of lowering the risk: could exercise be one?
A meta-analysis of four studies shows an association between a reduced risk of esophageal cancer and exercise.
Siddharth Singh, MD, of the Mayo Clinic, found a 32 percent lower risk of a type of disease called esophageal adenocarcinoma in physically active subjects.
This can arise from a condition called Barrett’s esophagus, which can spring from chronic gastroesophageal reflux disease.
The overall risk reduction was 19 percent in the most physically active subjects, compared to the least active.
The Connection Between Exercise & Esophageal Cancer
One way that working out may have a reduced effect on the development of esophageal cancer is by reducing the incidence of obesity, which has been implicated as a risk factor for the disease, says Dr. Singh in his report.
The Issue of Cause and Effect vs. Association
“I’m a believer in the benefits of exercise, but Singh’s meta-analysis doesn’t convince me that it’s the exercise that reduces this particular risk,” says Alex Little, MD, a thoracic surgeon with a special interest in esophageal and lung cancer.
“His study looked at the association between the two; not the same as cause and effect.
“Although he identifies some ways in which exercise could cut the risk, it’s also possible that people inclined to exercise are born with good genes and/or immune systems, have better nutrition or a lifestyle that reduces the risk — and they would have this benefit even if they were prevented from exercising.
“None-the-less, I’m for regular exercise for all the reasons a personal trainer would know.”


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}