

How Normal Is Pain After Carpal Tunnel Release?

There are two explanations for pain persisting after carpal tunnel release.
What is a carpal tunnel release?
The median nerve and tendons pass through a narrow passageway in the wrist: the carpal tunnel, formed at the wrist bones on the bottom, and the transverse carpal ligament that goes across the top of the wrist.
The tissues will swell when this area is tight (or injured), causing pressure on the median nerve: hence the numbness and tingling, sometimes pain.
In the release procedure, the ligament that’s pressing on the carpal tunnel is cut, making more room for the median nerve/tendons to pass through.
- So why, then, can the pain, numbness and tingling continue after this procedure?
- After all, it seems like a pretty straightforward fix.
“Pain after a carpal tunnel release can be due to either persistent carpal tunnel syndrome or recurrent carpal tunnel syndrome,” says Jonathan Oheb, MD, Chief of Orthopedic Hand and Upper Extremity Surgery at North Valley Orthopedic Institute.
Dr. Oheb explains, “Persistent pain, in which the pain never improves after surgery, can often be due to an incomplete carpal tunnel release.
“This is differentiated from recurrent carpal tunnel syndrome in which the pain resolves and then recurs over the course of time as scar tissue that forms places pressure back over the median nerve.”
Scar Tissue Formation
This is not an uncommon complication after carpal tunnel release.
The carpal tunnel, having been snipped, triggers a healing response from the body, resulting in excessive scar tissue in some cases.
Nearby soft tissues then get bound together, and the skin nearby may feel tight.
Hand and wrist movement may feel restricted.
But that’s not all. The scar tissue can bind the median nerve and tendons, keeping them from smoothly gliding within the carpal tunnel. Pain is the result.
If the pain can’t be managed, then a second carpal tunnel release may be performed.
 In addition to hand, elbow and shoulder care, Dr. Oheb provides comprehensive surgical and nonsurgical treatment for all orthopedic conditions of the hip, knee and ankle, including broken bones and injuries. jonathanohebmd.com
In addition to hand, elbow and shoulder care, Dr. Oheb provides comprehensive surgical and nonsurgical treatment for all orthopedic conditions of the hip, knee and ankle, including broken bones and injuries. jonathanohebmd.com
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik/krakenimages.com

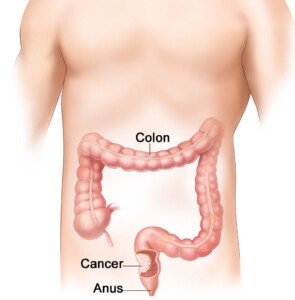
Can One Bowel Movement a Week Be Normal?

If you’re having only one bowel movement a week, this can mean an obstruction, says gastroenterologist Sander R. Binderow, MD.
“It is important to also ask patients if they are passing gas if they have not had a bowel movement for a week,” explains Dr. Binderow, who’s with Atlanta Colon & Rectal Surgery.
“If the person has not passed gas nor had a bowel movement, then there could be an obstruction, and they should seek immediate medical attention if they have not already.”
Can one bowel movement a week ever be normal?
Dr. Binderow says, “If someone is not having bowel movements, but they’re passing gas, have no pain, are not nauseous – then they are probably constipated.
“Although they still may need medical attention, it is not immediate. Laxatives may help.”
This isn’t to say that being this constipated is normal.
But at least the presence of passing gas, and absence of other symptoms, point away from an obstruction as being the most likely cause.
More on Bowel Obstruction As Cause of One Bowel Movement a Week
“A patient with the above symptoms and no BM, especially if onset is sudden and acute, may have a bowel obstruction,” continues Dr. Binderow.
“They need to seek medical care immediately. Laxatives may further harm this situation.”
So will trying to “push” the constipation out by loading up on heavy, rich foods. This won’t push it out; it will only add to it.
Can a change in diet or a particular kind of diet cause a person to poop only once a week?
“Diet won’t affect this at all,” says Dr. Binderow.
And here is some striking news: Suppose you take laxatives and these produce a bowel movement—finally.
Do not make the mistake of thinking that this is a sign that “it can’t be cancer.”
Here is what Dr. Binderow says: “Laxatives may still work in a partially obstructing colon tumor. It does not point away from a tumor.”
If your constipation continues — even if you don’t have pain, nausea or even if you’re regularly passing gas, you should opt for a non-invasive, cancer colon screening exam such as Cologuard.

This can be done at your home and it “only requires following up with a colonoscopy if you receive positive results,” says Dr. Binderow.
Cologuard uses the latest in DNA technology to identify abnormal cells in your stools.
 Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sasha2109

Does Housework Count As Physical Therapy for a Herniated Disc?

Huge mistake if you think your housework magically replaces the physical therapy you’ve been prescribed for a herniated disc.
You’ve been diagnosed with a herniated disc.
You had a session of physical therapy with a specialist, who showed you how to do the exercises at home.
After your first home session, you’ve decided that the exercises are a waste of time.
They’re boring and don’t even seem like they could help anything — mostly easy movements that don’t immediately make your sciatica feel better.
(Tip: You should wait about three weeks to determine if physical therapy works—and that’s only if you’ve been sticking to it faithfully, by the book.)
“Physical therapy is not just about movement,” says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
“It incorporates using your muscles and increasing your flexibility through a set of engagements that are focused on a particular area. You aren’t going to get that in daily activity.
“You need to intensely focus on that particular part of your body.
“Physical therapy is designed to alleviate pain and strengthen and tone core muscles.
“And once you learn these modalities, you can do a lot of them at home.”
If you still believe that “all that housework” you do is just as good as any physical therapy exercises, then how come you developed a herniated disc in the first place?
 Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com, pressfoto

Can Excessive Rest Interfere with Herniated Disc Rehabilitation ?

A spine doctor has bad news for those with a herniated disc who spend lots of time lying around, even if they do therapy exercises.
So you have a herniated disc and it hurts like mad. You do therapy or rehab exercises and do other things for pain management such as taking medications and using heat.
However, the recovery or rehab process will be hampered if you lead a sedentary life, even if you use the pain as an excuse to spend a lot of time in bed or in your favorite reclining chair.
“Yes,” says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
“Studies show that bed rest is actually detrimental to you as far as recuperation from a back injury. I don’t recommend bed rest in any form for someone with a problem in their back.”
And you can bet on it, “sitting” way back in a recliner chair and watching TV counts as bed rest.
Dr. Perry continues, “Being very active, with little down time, is important. Don’t take specific hours of the day to lie down for back pain because inactivity is not good for the spine.
You need to be mobile. If you have neck or back pain, you should incorporate low-impact exercises such as walking, yoga and Pilates into your daily routine to help strengthen your core muscles.”
As a former certified personal trainer for a large health club, I never tire of telling people that HOLDING ONTO a treadmill while walking can potentially cause repetitive stress injuries in various joints, as this throws the body’s natural gait, spinal alignment and posture off-whack. Read more about treadmill incline walking and back pain.
It may seem counterintuitive not to take to sleeping off pain from a herniated disc, but all that sleeping or excessive lounging around will do is numb your awareness of the pain, or put your body in a position that helps conceal some of the pain.
But it does nothing for healing, zero for recovery. Get up and move! The human spine was designed for lots of movement, not inertia.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/fizkes

Are Epidural Injections Safe for the Elderly?

A doctor explains the safety of an epidural injection for the elderly patient including those with heart disease.
You may also be wondering if this procedure is done under general anesthesia (to guarantee the patient won’t move).
“General anesthesia isn’t required for an epidural injection,” says Dr. Michael Perry, MD, member of the North American Spine Society and American College of Sports Medicine.
“Typically, they can be done with local anesthesia. If the patient is very anxious, a light sedation can be used.”
Epidural steroid injections are usually administered to people who have pain from a compressed nerve at the location of their lower spine.
The irritation results in local inflammation. The drug that’s injected calms down this inflammation, thereby reducing pain.
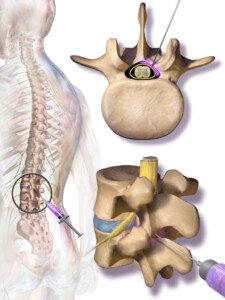
Epidural injection. BruceBlaus/CC
Whether the patient is younger or elderly, these epidural injections typically last around three months, sometimes a little longer. They are quite safe for an older patient, but what about one with heart disease?
Heart Disease in an Elderly Patient
“As it relates to heart disease, as long as the patient is in good medical health or being followed regularly by a doctor, an epidural injection is not very risky,” says Dr. Perry. “The problem comes in if the patient is on blood thinners.
“In this case, if you do an epidural, there is a risk of developing a hematoma (collection of blood), which can cause spinal cord compression and be very dangerous.
“Their doctor should ask if they’re on anti-coagulation/blood thinners before giving an epidural injection. For the most part, age doesn’t matter when it comes to epidural injections. And neither does the patient’s history of CABG.”
If anything is harmful to the aged person, it’s living with the pain that a compressed or “pinched” nerve in the lower back causes. Pain is also not always the only symptom; there may be tingling, numbness and weakness in the leg.
The drug that’s used for an epidural injection is a corticosteroid.
Dr. Perry is chief medical director and co-founder of USA Spine Care & Orthopedics, and is frequently sought out for his minimally invasive spine surgery expertise.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Voronin76
Is One Bowel Movement Every 3 Days Normal?
Here’s what a gastroenterologist says about having one bowel movement every three days.
Some people have been led to believe that we “should” have one bowel movement every day—that it’s not normal to skip a day.
But some people have, on average, one bowel movement every three days. Is this normal?
“Normal bowel movements and normal bowel movement schedules range from up to three bowel movements per day and all the way to one bowel movement every three days,” says Sander R. Binderow, MD, FACS, FASCRS, with Atlanta Colon & Rectal Surgery.
He adds, “Not everyone has a bowel movement every day.”
Don’t panic if it’s been two days since your last bowel movement.
In fact, even if three days go by, there’s really no need to lose sleep. Dr. Binderow says that “a lot of people react to their bowel movements when they shouldn’t.
“If there is one incident of diarrhea, and then the person takes Imodium, and then they’re constipated so they take laxatives, they’re creating more of a problem than if they do not react to their bowel movement habits when any change occurs.
“If a person is concerned about a change in their bowel habits that does not return to normal within a few days, they should consult with their doctor to address their concern.”
What may seem like three days without a bowel movement might actually be two days if you’re a very busy person.
So it’s recommended that you track your bowel movements on a daily basis.
This way, over time, the picture will become clearer as to what is normal for you.
For example, what’s normal for me are what I call “doubles.” These are two days without a bowel movement.
It’s normal in that, though this is not a common occurrence, it’s also not what I’d consider rare or too unusual, either. It happens.
I could flip through my pages of daily trackings and see that every so often, a double comes up.
There’s even been a few instances of triples: three days without a bowel movement.
To ease any worries about your stools, you may want to have a non-invasive screening test for colon cancer called Cologuard.

Cologuard uses up-to-date advances in DNA technology to identify abnormal cells in the stool sample that may be a sign of colon cancer or precancer.
Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Stool Texture vs. Black Tarry Color for Colon Cancer Sign

Just what is meant by “tarry” stools, and is texture important as a sign of colon cancer?
How often have you read that “tarry” stools are serious cause for concern and warrant a prompt visit to a gastroenterologist?
But just what does “tarry” mean in this context?
“Tarry black stool usually refers to a dark black color,” explains Sander R. Binderow, MD, FACS, FASCRS, with Atlanta Colon & Rectal Surgery.
He adds, “Until a bowel movement is truly black, there is no need for concern.”
Bowel movements can easily appear black in non-bright lighting, especially if the toilet bowl is stained from not having been cleaned in a while.
To get a clearer view of your BMs, you should remove some from the toilet and place on a white paper plate under good lighting.
If your vision isn’t clear with close-up views (i.e., you need reading glasses), then make sure your reading glasses are on.
If you still have problems with clear vision for up-close inspections, then inspect your stools without any visual aid — see if that yields a good clear view.
What appears to be a “tarry” stool may in fact just be a very dark green/brown or dark magenta/brown (from beets).
How important is stool texture as far as possible colon cancer?
Dr. Binderow says, “Texture rarely is addressed to determine any health issues because this can vary based on a numerous amount of conditions including your environment and what you eat or drink.
“People place much more importance on the texture of their bowel movement than is necessary.
“The color, if it is not dark brown or dark green and resembles the color of tar, is more of a concern and should be discussed with the person’s physician.”

Black stools
Tar is as black as black can get — ever see hot tar in liquid form in a vat before it’s laid on the ground?
The stuff is blacker than black — and stinks to high heaven, too.
Anyways, don’t get caught up with the texture of your stools, but rather, pay note of the color.
As for colon cancer, you’ll want to consider Cologuard, which is a non-invasive screening test for cancer of the colon.

Cologuard uses the latest advances in stool DNA technology.
It detects the changed DNA from abnormal cells in stool samples which could be associated with cancer or a precancerous polyp.
Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/serato

Thick Stools Suddenly Get Thin: Colon Cancer?

So many people are scared of seeing the so-called pencil-thin stools—even if the day before, their bowel movements were thick or fat.
“The reason that a stool changes from wide and then thin can be caused by what a person drank, ate or what environment they have moved to,” says Sander R. Binderow, MD, FACS, FASCRS, with Atlanta Colon & Rectal Surgery.
He continues, “It is an overall non-specific variable. If a person has a tumor, the stool can become thinner from obstruction, but this is NOT common.
“Colorectal [colon] cancer wouldn’t cause the thickness of stool to change, but a tumor in the lower anus or rectum could.”
How does cancer make stools come out thin?
BMs come out the anus, which is of a certain width range when normal, allowing the stool matter to come out.
If there’s a cancer mass near the anus or rectum, then the bowel movements that are on the way out would have to go through a narrower pathway or channel, as the tumor would be obstructing the pathway.
The stools would then be compressed into a thinner diameter.
It’s the same principle when the opening of a tube of toothpaste becomes obstructed by dried, caked-on toothpaste.
You squeeze the tube hard, and the paste comes out with difficulty — and it’s much narrower than normal, because the hole that it comes out of is partially blocked by the dried toothpaste.
Dr. Binderow says, “Most persons will see their stools vary in thickness throughout their life, which is considered normal.
“Consistency of the stool and size are not as important as some [people] place on these changes.
“If a person is concerned, they should always discuss with their physician before drawing conclusions and to know what is normal and what to expect moving forward.”
Fear of Colon Cancer
With the increasing publicity about colon cancer, there’s an increase in anxiety over this in people who have taken to inspecting their stools.

Cologuard is a non-invasive screening test for colon cancer.
Cologuard uses the latest advances in bowel movement DNA technology, thus detecting the altered DNA from abnormal cells in the stool sample.
These cellular abnormalities may be associated with colon cancer or precancer.
Dr. Binderow performs minimally invasive, robotic and laparoscopic surgery for Crohn’s disease, ulcerative colitis, colon cancer and other colorectal conditions. Adept at routine procedures, he also sees patients with complex, atypical maladies.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Ruptured Aneurysm Headache vs. Acute Subdural Hematoma

A headache expert describes the difference between ruptured aneurysm head pain and that from an acute subdural hematoma.
“Headaches related to ruptured aneurysm can be difficult to distinguish from that of a subdural hematoma,” says Noah Rosen, MD, Director, Northwell Health’s Headache Center in Great Neck, NY.
What a headache from a ruptured aneurysm has in common with the head pain from an acute subdural hematoma is that both are very intense — often described as a thunderclap headache.
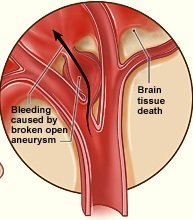
However, in the case of a ruptured aneurysm, the thunderclap is more pronounced and sudden, like BOOM!
This is easy to understand when you visualize the aneurysm suddenly rupturing or bursting, spewing blood onto the brain.
“Thunderclap headaches are almost always a warning of some dangerous situation that requires immediate attention,” says Dr. Rosen.
“This can include bleeding such as that of a subarachnoid hemorrhage, intracerebral hemorrhage [hemorrhagic stroke] or epidural or subdural hematoma.”
The term, subdural hematoma, is not to be equated with chronic subdural hematoma.
In fact, the more specific term of the condition associated with a sudden, roaring headache is acute subdural hematoma.
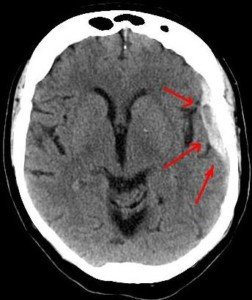
Subdural hematoma. Credit: Lucien Monfils
But often, the term “acute” is left out. “Acute” means sudden, as in head trauma resulting from going through the windshield of a car.
In the case of a chronic SDH, the bleeding in the brain is very slow—so slow that eight weeks may pass before the patient begins developing the first symptoms.
The symptoms are not immediately life-threatening in the chronic type.
In the case of my mother, her surgery to drain her chronic SDH was scheduled for the morning following her early evening admission to the hospital.
Her first symptom (a severe but non-thunderclap headache) came six weeks after hitting her head in a fall.
Dr. Rosen explains, “Acute subdural hemorrhage often presents as a thunderclap headache due to rapid expansion, irritation of local blood vessels and the meninges (or covering of the brain).”
Headache of a Ruptured Aneurysm
“They are also thunderclap in onset, are generally associated with more rapid loss of consciousness or other focal neurologic deficits,” says Dr. Rosen.
Whether ruptured aneurysm or (acute) subdural hematoma, both conditions require “immediate emergency evaluation and neuroimaging (such as a CAT scan) to determine the next course of action.”
The way these headaches feel to the patient, then, may be indistinguishable.
However, one of the hallmark features of an acute subdural hematoma is a type of vomiting called projectile.
An example: If a football player takes a very hard hit in the head and is walked off the field, sitting there on the sidelines dazed, and then suddenly vomits in a projectile path, chances are high that there is rapid bleeding in his brain. This is a medical emergency.
 Dr. Rosen’s career is dedicated to treating what he believes is an underserved patient population: those with migraine and other headache disorders.
Dr. Rosen’s career is dedicated to treating what he believes is an underserved patient population: those with migraine and other headache disorders.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/KDdesignphoto

Can You Die Directly from Multiple Sclerosis?

A neurologist answers the question of “Can you die directly from MS?”
Anyone who has ever known someone who was suffering from multiple sclerosis may wonder if this autoimmune disease can actually be fatal.
Some patients are bedridden from this illness.
Many need a wheelchair to get around.
Can Multiple Sclerosis Kill?
“The disease is not fatal,” says Karen M. Blitz-Shabbir, DO, a neuro-rehabilitation and multiple sclerosis specialist based in Islip, NY.
She explains, “Most patients have normal life spans. Patients with advanced disease and disability can develop infections or other complications that lead to death.”
Infections and complications are potential secondary outcomes of MS, but multiple sclerosis, in and of itself, is not a directly fatal condition.
MS Complication that Can Be Fatal
Excessive bed rest, from being bedridden, can lead to a blood clot in the leg.
In fact, confinement to a wheelchair raises this risk as well.
There is nothing about MS itself that causes blood to pool in the legs and clot up. It’s the inertia of the legs that lead to this.
The name of such a blood clot is deep vein thrombosis. Excessive time in bed, regardless of condition (recovery from surgery, pregnancy, depression, mobility impairment) is a risk factor for a DVT.
This is why anybody who is bedridden from multiple sclerosis needs to have their legs, particular the lower portions, checked daily for signs of a DVT.
A DVT can break loose from where it has formed and travel to the lungs, blocking airflow, resulting in death.
Symptoms of a DVT
• One leg is suddenly swollen. This is often in the calve, but can occur above the knee.
• The leg may have a reddish discoloration. The color may also be pale.
• The leg may be unusually warm to the touch.
• The patient reports that it feels tender when touched.
• The calve area hurts or feels cramped up. This does not go away when seated or even lying down.
• These symptoms may also appear around and behind the knee, as well as in the pelvic area.
People with multiple sclerosis whose mobility is significantly impaired should ask their doctor about blood clot prevention.
 Dr. Blitz-Shabbir is also the medical director of rehabilitation with Holy Name Medical Center MS Center.
Dr. Blitz-Shabbir is also the medical director of rehabilitation with Holy Name Medical Center MS Center.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}