

Severe Knee Pain when Sitting: Causes, Solutions

Have you found that after sitting for a while, your knee begins hurting badly?
But then it gets better after you’ve been up for a while? What’s going on here?
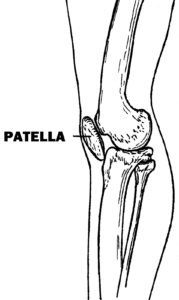
“One of the most common causes of knee pain is known as patellofemoral syndrome which simply refers to pain sensed by the nerves surrounding the kneecap,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
“This may result from a wearing away of the cartilage between the patella or kneecap and the femur, known as chondromalacia patella.” The femur is the thigh bone.
“This can lead to inflammation between the femur and patella, leading to pain with movement.
“There is often pain when standing and walking after a period of prolonged sitting, a phenomenon known as theater sign.”
Patellofemoral syndrome may also lead to what is known as a tracking problem with the patella.
The patella bone is supposed to track nicely in its groove, but if it strays off its natural fit in the groove…you may experience a lot of pain after sitting for prolonged periods.
Oddly, it may feel nearly fine after you’ve been up and about for a while.
Patellar tracking problems happen more often to women, but men are not immune.
Improper biomechanics during exercise or athletics may cause it.
Chondromalacia patella in athletes is commonly caused by jumping or fast running. But longer, slower running can also cause it.
Solutions
- Avoid the offending activity.
- Do leg extensions (“leg extension machine”) with light weight and high repetitions.
- Avoid hyperextending the knee.
- As you get used to the leg extensions, increase the weight so that you’re doing strength training on the machine twice a week.
- However, on other days, do weightless knee extensions, 20 reps toes pointed to ceiling, 20 with toes pointed out and 20 with toes pointed in.
After following these measures, you should no longer suffer so much with severe knee pain while sitting.
One More Possible Cause of Sitting Knee Pain
Much less likely, but not impossible, is a condition called patellar tendonitis: inflammation of the tendon that joins the patella to the tibia (main shin bone).
While seated, the pain can be triggered if your leg is bent under a chair. However, the pain wouldn’t necessarily be severe.
Running, jumping and squatting are chief causes of patellar tendonitis.
 Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik

Painful Bony Lump on Kneecap (Cancer?) Explained by Doctor

A doctor, not a layperson in a forum, explains possible causes (cancer??) of a painful bony lump on your kneecap (patella).
“The most common cause of a lump on the patella is Osgood-Schlatter disease,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
“This is caused by inflammation of the patellar tendon and is most common in adolescents,” says Dr. Peck.
“Risk factors include overuse from sports and periods of rapid growth as during adolescence. It is benign and is often easily treated with rest and ice.”
What about cancer?
Dr. Peck says, “A painful lump on the patella is very unlikely to be cancer. Most bone tumors are not malignant and may not be painful.
“With bone tumors, there will commonly be associated symptoms such as weight loss, fatigue or other symptoms, and pain will typically be progressively worse over time.
“There may be no pain, and bony tumors sometimes present as fractures, as bones affected by tumors become weaker.
“However, any new lump or mass should be brought to the attention of your physician.”
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Top image: Shutterstock/Syda Productions
Knee Pain after Hip Surgery: Causes, Solutions

A physician cites three possible causes of knee pain following hip replacement surgery.
“Knee pain after hip surgery is a poorly-understood phenomenon,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
“A small retrospective study examined 13 patients who’d had hip replacement,” continues Dr. Peck. “Eight of the patients reported knee pain after the surgery.”
Three Possible Causes of Knee Pain after Hip Replacement Surgery
Dr. Peck explains, “Biomechanical measurements before and at six weeks after surgery [in the aforementioned study] did not demonstrate significant differences.
“Reasons for this phenomenon remain unclear, but may include changes in gait and leg length, and elimination of a greater pain-generator (hip), leading to more noticeable discomfort in the knee.
“Patients with severe hip osteoarthritis may develop a gait abnormality, known as Trendelenburg gait, due to weakness in the hip abductor muscles.
“This gait can lead to uneven pressures across the knee joint, and resulting arthritis in that joint.”
Hip abductor muscles are located on the outer side of your hips and are primarily responsible for moving your leg away from your body’s midline.
Solutions to Knee Pain Following a Total Hip Replacement Surgery
“The best way to optimize outcome after any joint surgery is to optimize preoperative conditioning,” says Dr. Peck.
This means “participation and compliance with a formal PT program along with home exercises (very important!).”
If the patient has excess body weight, then losing this weight will also help relieve some of the pain, since the knee, being the most unstable joint in the entire body, is very sensitive to excess body fat.
Hence, even a 10 percent weight loss will yield some improvement in the way this joint feels.
The patient may believe that fat loss is impossible due to limitations in the ability to use the lower body.
However, upper body strength training exercises will facilitate fat loss.
By engaging in these exercises, you build lean muscle mass, which increases your overall metabolism.
This enhanced metabolic rate helps your body burn more calories, both during exercise and at rest.
This loss of body fat is so important for anyone who’s struggling with knee pain following surgery of the hip.
And of course, consuming fewer calories will get weight loss going.
This deficit forces your body to burn stored fat for energy.
Consuming fewer calories begins with replacing soda with water; juice with whole fruit; more home cooking and less fast-food, and mindful eating: the avoidance of eating for reasons other than hunger, such as when watching TV or using the computer.
Remember, even a 10% weight loss can improve knee discomfort that has resulted from a hip surgery.
Upper Body Strength Training Exercises

Shutterstock/Halfpoint

Freepik

Freepik

Shutterstock/Microgen

Freepik
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
How Long Does Knee Arthroscopy Rehab Take?

“There is a great deal of variability in terms of length of time taken to recover from knee arthroscopy,” explains Devin B. Peck, MD, owner of Austin Interventional Pain.
Dr. Peck continues, “This variability depends on both patient factors, including age, pre-operative physical condition and compliance with rehabilitation, as well as procedure factors, i.e., what type of repair is performed.
“In a patient with good pre-procedure fitness, recovery from simple arthroscopy including washout of debris but not requiring repair of major ligaments, can take as little as two to four weeks.
“Recovery from large repairs, such as of the anterior cruciate ligament (ACL), can take several months.”
Really bad ACL injuries can take about nine months to completely recover from as far as returning to pre-injury athletic activity.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/kazoka

Hip Pain when Standing Up: Causes & Solutions

“Hip pain present while standing may represent degenerative joint disease (osteoarthritis) of the hip,” says Devin B. Peck, MD, oowner of Austin Interventional Pain in Austin, TX.
The hip joint consists of a ball-and-socket design. The bone “ball” is not supposed to make contact with the bone of the socket.
There’s cartilage in between to prevent this. Wearing down of the cartilage is what occurs in osteoarthritis. Wearing down means less shock absorption.
Sometimes the cartilage is so worn down that these bony portions begin rubbing against each other, causing hip pain, including when you stand up.
Dr. Peck explains, “Risk factors include obesity, advanced age or prior trauma. This is the most common cause of hip pain in people over age 65 and can present as groin or thigh pain.”
Another risk factor is lack of weight-bearing exercise such as leg presses, squats and walking lunges.
“Severe, sudden onset of severe hip pain which may occur only with standing should raise concern for hip fracture.
“This can occur without significant trauma in patients with osteoporosis.”
In fact, a hip fracture can be caused by standing up from a seated position in someone with very brittle bones.
“Trochanteric bursitis is another common cause of hip pain which can be present when standing up, walking, climbing steps, driving or lying on the side.”
Solutions
“If pain is due to osteoarthritis, exercises that strengthen the abductors of the hip (gluteus minimus, gluteus medius, vastus lateralis) are important,” says Dr. Peck.
“A simple exercise is to lie on your back with knees bent, squeeze the buttocks, and hold for five seconds for 30 reps.” See the image below of the bridge position.

Bridge hold. Freepik.com, Mangostar
“To make this more challenging, you can lift your pelvis up off the floor and hold for five seconds,” says Dr. Peck.
“Be sure to brace the abdominal muscles while doing this to avoid low back strain.”
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/HENADZI PECHAN
Does Knee Bursitis Always Cause Swelling?

You may be aware that bursitis of the knee can cause swelling, but is this necessarily so in every single case?
“Knee bursitis may or may not result in visible or even palpable swelling,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
Palpable refers to detecting the swelling by feeling with your fingers, whether or not you can visually detect it.
Dr. Peck adds, “The more superficial bursae [plural of bursa], such as the prepatellar, superficial infrapatellar or pes anserine bursae, are more likely to lead to swelling that can be seen without MRI or CT scan.”
Another condition of the knee, chondromalacia patella (sometimes referred to as patellofemoral syndrome) may produce symptoms that make a person wonder if indeed the problem is actually bursitis.
The symptoms have some overlap, and chondromalacia of the patella does not cause swelling – just like sometimes, bursitis won’t cause swelling.
What to Do if Your Knee Starts Swelling
• Rest and Avoid Strain: Limit activities that put pressure on the knee to prevent aggravating the swelling.
Avoid walking long distances or engaging in strenuous activities that can worsen the condition.
• Apply Ice: Use an ice pack wrapped in a cloth and apply it to the swollen area for 15-20 minutes every 2-3 hours during the first 48 hours. This can help reduce inflammation and numb the pain.
• Elevate the Knee: Keep the affected knee elevated above heart level as much as possible. This helps reduce fluid buildup and encourages proper blood flow.
• Compression: Use an elastic bandage or knee brace to provide gentle compression.
This can help control swelling and provide support. Ensure the bandage isn’t too tight, as it could impede circulation.
• Over-the-Counter Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs), like ibuprofen or naproxen, can help reduce pain and swelling.
Follow the dosage instructions on the label and consult with a healthcare provider if you have any health conditions or are taking other medications.
• Seek Medical Attention: If swelling persists for more than a few days, is severe, or is accompanied by other symptoms such as significant pain, difficulty moving the knee, or a fever, seek medical evaluation.
Persistent or severe swelling might indicate an underlying injury, infection, or chronic condition that needs professional assessment and treatment.
• Gentle Exercises and Stretching: Once the initial swelling decreases, gentle range-of-motion exercises and stretching can help restore flexibility and strength.
Consult a healthcare provider or physical therapist for appropriate exercises that won’t aggravate the condition.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/DeepMeaning

Crunching Sound from Knees: Causes, Solutions

“Crunching sound in the knee is referred to by physicians as crepitus,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
What causes a crunching sound in the knees?
Dr. Peck explains, “It is typically caused by the rubbing of cartilage on the joint surface or other soft tissues around the knee during joint movement.
“When crepitus is painful, it may represent the sliding of an irregular, damaged or degenerated ligament.
“It can also indicate damage or irregularity in one of the menisci (plural of meniscus), the pads of cartilage which cushion the inner and outer aspects of the knee joint.”
If the crunching sound in your knee or both of them is not accompanied by any discomfort, there is no reason to be concerned.
Dr. Peck says, “Benign, painless crepitus is common and requires no treatment.
“However, painful crepitus can indicate degenerative arthritis, inflammatory arthritis (like rheumatoid arthritis) or an injury to one of the ligaments or menisci.”
Solutions
“Treatment will depend on the cause, but may include physical therapy, anti-inflammatory medications, injections or surgery.”
Which means, if you’re seeking solutions to a crunching noise in one or both knees that is also accompanied by pain or even a feeling of instability, it’s time to see a doctor to find out exactly what is wrong.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/thebigland

Can Knee Bursitis Cause Pain ONLY when Kneeling?

Is that knee pain you get only when kneeling possibly caused by bursitis in this joint?
“Infrapatellar bursitis can lead to pain while kneeling,” says Devin B. Peck, MD, owner of Austin Interventional Pain in Austin, TX.
Dr. Peck explains, “In fact, superficial infrapatellar bursitis is commonly known as ‘clergyman’s knee’ or ‘plumber’s knee,’ a reference to kneeling.
“Prepatellar bursitis can also lead to pain with kneeling, although it can also result in non-painful swelling over the kneecap. Prepatellar bursitis is sometimes known as housemaid’s knee.’”
Be aware that another condition, unrelated to bursitis, can cause pain in the knee only when kneeling.
It’s called chondromalacia patella or patellofemoral syndrome.
However, this condition usually also causes discomfort when going up stairs, running, jogging and/or sometimes jumping.
The discomfort may be a strong or dull ache and/or a sensation of fullness or tightness under the kneecap.
Dr. Peck’s areas of interest include chronic and acute musculoskeletal pain, sports injuries, arthritis and cancer pain, among many others. Austin Interventional Pain was established in 2019.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ThamKC

Wrist Pain While Lifting Weights: Causes, Solutions

A doctor provides causes and solutions to wrist pain while weightlifting.
What are the possible causes of wrist pain that is brought on during a weightlifting set?
“This can often be related to De Quervain’s tenosynovitis,” begins Asim S. Aijaz, MD, a board certified pain management specialist with Advanced Pain Care in Texas.
Dr. Aijaz continues, “This is pain along the radial (thumb) aspect of the wrist. While the exact cause is unknown, repetitive wrist movements can make it worse.
“It is often seen in new mothers who are lifting their babies repetitively. In weightlifting, hammer curls can reproduce this movement and can potentially aggravate the symptoms.”
When your wrists hurt during lifting weights, the tissue that’s involved usually relates to the tendons, as it does with De Quervain’s tenosynovitis, “but it may also be a problem in the joint such as with arthritis, or in the bone if there is a small fracture (more likely with impact exercises such as boxing or punching a heavy bag),” says Dr. Aijaz.
So which exercises should a person with wrist pain avoid doing?
Dr. Aijaz explains, “Hammer curls. Do supinated curls to relieve some of the stress along the radial aspect of the wrists.”

Supinated means palms facing forward when your arms are straight, and as you bring the dumbbells or barbell up, your palms are facing towards you.
Dr. Aijaz adds, “Avoid impact exercises. If doing burpees, make sure you are using proper form with the pushup part of the exercise and that you’re not hitting the ground too aggressively as you are approaching the pushup position of the exercise.
“Listen to your body, if you notice a certain repetitive exercise aggravates the pain, avoid it.”
What exercises can you do?
“If your pain persists you may benefit from having somebody evaluate your form to make sure you are not putting unnecessary stress on your wrists with common exercises such as pushups, bench press, curls,” says Dr. Aijaz.
“Sometimes it’s just a matter of proper hand positioning to reduce the stress: spreading out your fingers to distribute weight through your fingertips during pushups for example.”
If you’ve developed wrist pain in the course of your weightlifting regimen, ask yourself if this pain began after you one day decided to try an E-Z curl bar for biceps curls.
Though these bars are designed to reduce wrist strain, they can actually strain the wrists in someone who’s used to doing curls with a straight bar.
So if this describes you, abandon the E-Z curl bar and go back to the straight bar.
“Generally if the pain is related to a tendon issue or arthritis, one may find it beneficial to reduce the weight and adjust the form or take a break from exercises which stress the wrists,” says Dr. Aijaz.
“During your break from these exercises, you may find relief with ice and anti-inflammatories.
“As you’re getting back into your workout, you may consider wearing a wrist support and see if this helps in preventing the pain from returning.”
Carpal Tunnel Syndrome
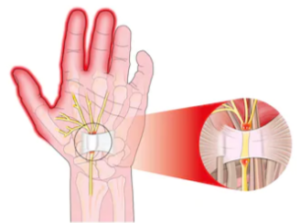
Shutterstock/Alexonline
“Occasionally patients with carpal tunnel syndrome will complain of hand and wrist pain that is exacerbated with weightlifting,” says Jonathan Oheb, MD, North Valley Orthopedic Institute, Chief of Orthopedic Hand and Upper Extremity Surgery.
 Dr. Aijaz has been involved with the Texas Pain Society, Spine Injection Society and the American Society for Interventional Pain Physicians.
Dr. Aijaz has been involved with the Texas Pain Society, Spine Injection Society and the American Society for Interventional Pain Physicians.
 In addition to hand, elbow and shoulder care, Dr. Oheb provides comprehensive surgical and nonsurgical treatment for all orthopedic conditions of the hip, knee and ankle, including broken bones and injuries. jonathanohebmd.com
In addition to hand, elbow and shoulder care, Dr. Oheb provides comprehensive surgical and nonsurgical treatment for all orthopedic conditions of the hip, knee and ankle, including broken bones and injuries. jonathanohebmd.com
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Top image: Shutterstock/ruigsantos

Stabbing Shooting Pain in Achilles Tendon: Causes, Solutions

A doctor explains why your Achilles tendon has shooting, stabbing pain and what can be done to remedy this situation.
“Pain here is generally the result of tendonitis or inflammation of the Achilles tendon,” says Asim S. Aijaz, MD, a board certified pain management specialist with Advanced Pain Care in Texas.
He continues, “You can also develop tears in the tendon which would also cause tendonitis and pain.”
So how does this situation arise in the first place?
Dr. Aijaz explains, “As with tendonitis in other parts of the body, this is often related to repetitive use or over-exertion, causing tears or degenerative changes in the tendon.
“Bone spurs at the heel can also cause small tears in the fibers, causing Achilles tendon pain.
“Tight calf muscles can also result in increased stress on the Achilles tendon.”
Solutions
“Rest, ice, anti-inflammatories, appropriate stretching (generally the calf muscles) and appropriate shoes,” says Dr. Aijaz.
“If symptoms persist, physical therapy can be very helpful.”
Also keep yourself well-hydrated, as tendons don’t get a lot of water because they are not densely vascular.
In fact, their low level of vascularity is why it takes tendons much longer to heal than do muscles.
Dr. Aijaz has been involved with the Texas Pain Society, Spine Injection Society and the American Society for Interventional Pain Physicians.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}