

Left Side Neglect Caused by Brain Bleed from Hit in Head
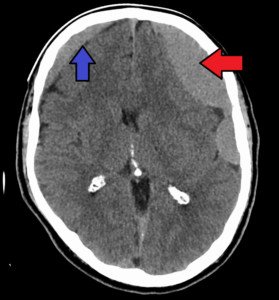
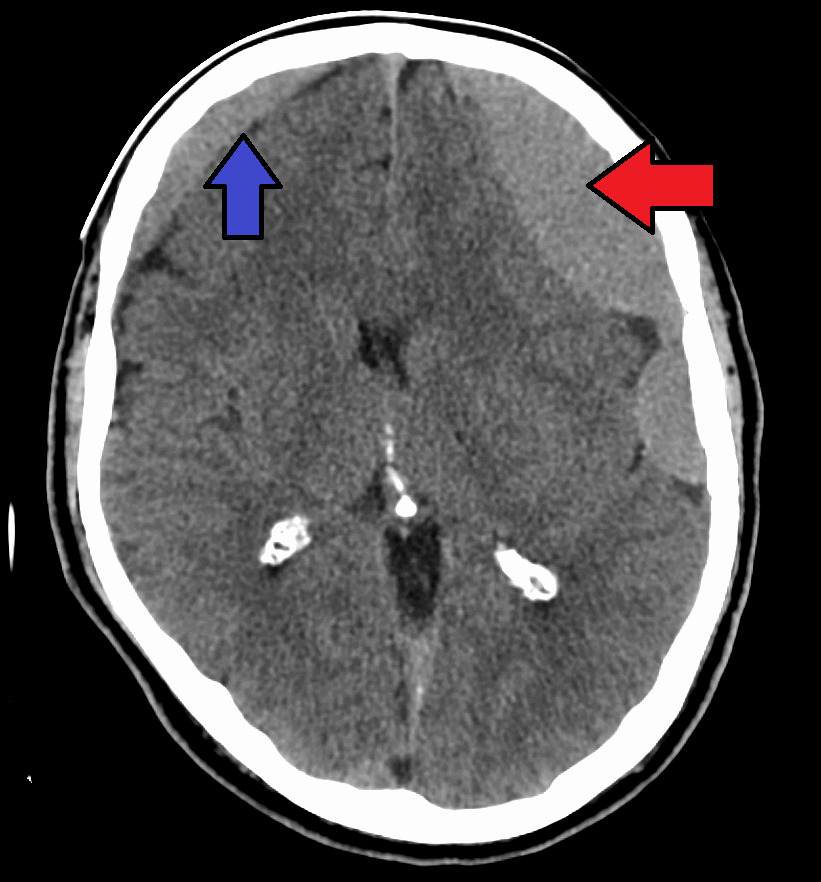
Left side neglect can be caused by a chronic subdural hematoma (a type of brain bleed) that’s on the right side of the brain.
My mother had a chronic subdural hematoma on the right side: twice.
There were no signs of left side neglect with the first chronic subdural hematoma.
It was drained, but about 10 days later she began dropping things with her left hand.
Over several days her gripping ability in the left hand deteriorated, along with fine motor control.
When my mother was recovering in the hospital following the second draining procedure, the physical therapist said she had left side neglect of the hand and leg.
In hindsight, it’s now clear that the motor control of her left hand, pre-surgery, was at least partially a left side neglect process, since she would try to pick things up and miss, yet think she had the item in her fingers, such as a hair clip.
She’d also try to pull up her panties or pants, and instead be pulling up air, believing she had the pants between her fingers, while the pants remained low on her body.
She’d then walk away, not aware that the left side of her pants/panties were not pulled up.
Pre-surgically my mother had wanted to go into the dining room from the kitchen, which requires a left turn.
But once through the doorway she veered rightward towards the living room.
At the time I thought this was some altered mental status, but in hindsight, I realize it was left side neglect, caused by a recurrence of the chronic subdural hematoma or brain bleed.
Post-surgically, she showed signs of left side neglect while working with her physical therapist.
The seating in her hospital room was to her left. If I started talking to her, while in the seat, while she was watching TV, she’d continue watching the TV, as though I weren’t there.
I’d then have to raise my voice to get my mother’s attention, or stand and move closer to her, more into her straight-ahead field of view, to get noticed.
This was left side neglect at work, even though the brain bleed had mostly been drained.
But residual fluid remained on my mother’s brain, and this remaining fluid caused more pronounced symptoms post-operatively while her body was working on resorbing it.
One she was transferred to a skilled nursing facility, the neurological phenomenon was more obvious.
She’d exit the bathroom (located at the beginning of her room) with her walker, and instead of making a 90-degree right turn towards the main room, she didn’t clear the turn and ended up hitting the wall (across from bathroom) with the left bottom of the walker.
In other words, when my mother was turning rightward, she wasn’t accounting for the left side of her surroundings.
When walking through the corridors, she kept getting sidetracked by rooms, doors and even wall pictures on the right. This was not normal behavior for her.
When a therapist had my mother fill in dates of a blank calendar, she started in the middle of the first row, which the therapist said someone with left side neglect would do.
Every time my mother exited the room, she’d make a right turn (which led to nowhere that would interest her: other patients’ rooms), even though we kept instructing “Go left” whenever she made this error (the dining hall was left, along with other main services).
As is typical with left side neglect, my mother was never aware there was something going on.
To someone with this intriguing condition, a therapist told me that it all seems normal to them, and that what they perceive as their “midline” is actually a rightward orientation.
The right side of my mother’s world was getting processed by her brain, yet the processing of the opposite side was compromised.
Chronic subdural hematoma on the right side of the brain can definitely result in neglect on the opposite side of the body.
As the brain bleed resolved, so did my mother’s left side neglect.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: James Heilman, MD, CreativeCommons

How Soon After Burr Hole Draining Can Chronic Subdural Hematoma Return?

Recurrence for chronic subdural hematoma is at around 15 percent.
The recurrence is not a sudden event, but unfolds over a short period of time.
My mother had a chronic subdural hematoma, and her neurosurgeon told me that one of the risks of the draining procedure was a 15 percent recurrence rate.
He did not tell me how long, after the draining it typically takes for a recurrence of a chronic subdural hematoma to develop.
Or, to put it another way, how long after treatment the symptoms of a recurrence would start presenting.
Variability in How Long It Takes a Chronic Subdural Hematoma to Come Back
“The recurrence rate is somewhat variable and will range anywhere from 10-30 percent,” says Kangmin Daniel Lee, MD, a neurosurgeon with New Jersey Brain and Spine.
“There is some variability in technique from surgeon to surgeon and will depend on the location and size of the chronic subdural hematoma.
“Sometimes two vs. one burr holes are used, and small vs. large sized burr holes are also used.”
My mother had one burr hole for her procedure. Dr. Lee continues, “There is also some discussion regarding the utility of a subdural drain once the burr hole washout is completed.”
My mother had such a drain after her surgery, and gravity was used to continue the draining while she was recovering in her hospital bed.
“However, the general consensus is that larger burr holes and the routine use of a subdural drain will minimize the risk of recurrence,” says Dr. Lee.
The post-surgical drain tube does not guarantee against a recurrence, because 10 days after my mother’s procedure, she started showing peculiar symptoms.
And it turned out she had a recurrence of the chronic subdural hematoma, and had to have a second burr hole operation.
But what about a specific time window or “grace period” following drainage of a first chronic subdural hematoma, as far as potential development of a recurrence? My mother’s time window was (to our observation) 10 days.
But is there data on how long after treatment would a patient be clear of ever having a recurrence of the chronic subdural hematoma?
Dr. Lee explains, “There is some variability with this number depending on the technique, but most recurrences, when it does occur, will happen in the short term. Most published reports range it from the 1-3 week period.”
]As you can see, my mother’s case clearly fits into what the published reports indicate.
Now, what usually causes the recurrence?
In my mother’s case, it didn’t seem related to the surgeon’s handiwork, because a CAT scan the morning after surgery was satisfactory to him, and the post-surgical drainage tube was ordered removed when it indicated that no more blood was coming out (though cerebral spinal fluid was, and the nurse told me that this was a sign that the drainage was nearing completion and that the tube should be removed).
I speculate that my mother’s recurrence of the chronic subdural hematoma was caused…believe it or not…by a second fall she took!
The first one was caused by striking her head on a bathtub after she fell. This fall was caused by blacking out while she was standing at the sink; she was experiencing frequent orthostatic hypotension.
The second fall occurred outside and I didn’t see it, but a witness said my mother did not hit her head.
The second fall apparently resulted from side effects of Keppra.
Though she didn’t hit her head, her neurosurgeon told me that the jarring from this second fall could have easily shaken things up in her brain and caused the recurrence of the chronic subdural hematoma.
The fall occurred the day after she was discharged from the hospital.

Dr. Lee focuses on minimally invasive techniques to treat traumatic and degenerative diseases of the spine and brain tumors. He’s been invited to speak at the regional and national levels on his research areas.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Alexander Raths

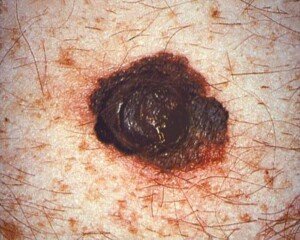
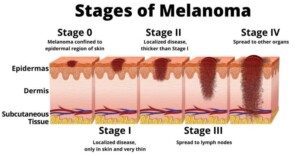
What Colors Can Melanoma Skin Cancer Be?

These four colors are just the tip of the iceberg.
It helps to know what the most common colors are for the deadliest skin cancer, melanoma.
Are there particular colors that melanoma skin cancer usually presents itself with?
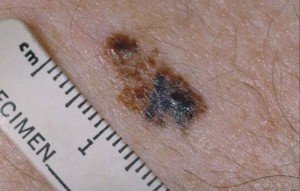
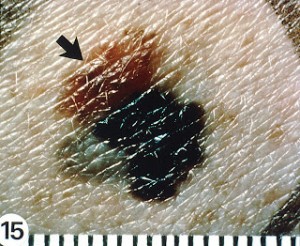
“Melanomas are usually multiple shades of red, brown or black,” says Glenn Kolansky, MD, with Advanced Dermatology Surgery & Laser Center of NJ.
“However, they can be one color.”
A normal mole, of course, is usually some shade of brown or tan. In fact, a benign mole can even be black or what appears to be black.
About one-third of melanoma skin cancer arises out of a pre-existing mole.
This is why it’s so critical to become very familiar with every mole on your body. This means you must locate all your moles.
You may have some behind your ear or just under your hairline, even between your toes.
Do don’t just look for moles in easy-to-look-for locations. Examine every area of skin possible, and even have someone check your scalp.
Use mirrors to check behind your ears and even inside the ears. Don’t forget the bottom of the feet and the eyelids.
What other colors can melanoma skin cancer be?
This killer of nearly 10,000 Americans every year can be brown, tan, grey, white, beige, beige-yellow, shades of pink, flesh colored, blue and violet. See the images below.

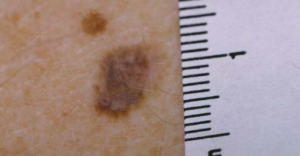


CDC, Carl Washington, MD, Emory Univ. School of Medicine, Mona Saraiya, MD, MPH
CDC, Carl Washington, MD, Emory Univ. School of Medicine, Mona Saraiya, MD, MPH
“Often a lesion can only be evaluated by doing a biopsy and looking under the microscope for a diagnosis,” says Dr. Kolansky. “This should be performed by a dermatopathologist.”
This cancer doesn’t necessarily present with changing color; it can also grow in size, change in texture, bleed, crust, become elevated and even itch.
Dr. Kolansky has received the Physician of Hope Award presented by the American Cancer Society and has lectured at local and national meetings.
has received the Physician of Hope Award presented by the American Cancer Society and has lectured at local and national meetings.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Fibromyalgia & Arm Pain When Fitness Walking: Solution

If your fibromyalgia gets in the way of your walking workouts by causing arm pain, there’s something you can do about this.
When you walk for fitness, especially on a treadmill, do you experience arm pain that you know is from your fibromyalgia?
Why does fibromyalgia induce pain in the arms from simply walking on a treadmill?
“This most likely occurs because you are using muscles you don’t usually use to either hold onto the bar or to keep your hands elevated,” explains Jacob Teitelbaum, MD, medical director of the Fibromyalgia and Fatigue Centers nationally, and author of “The Fatigue and Fibromyalgia Solution.”
I’m a former certified personal trainer and have helped countless clients bust the egregious habit of holding onto a treadmill while walking.

So very wrong! Shutterstock/LightField Studios
The harder you hold on, the more likely you’ll experience pain in the arms from your fibromyalgia.
I’ve even had healthy clients who, prior to hiring me, experienced unexplained pain while using a treadmill because they were holding on.
Holding on totally disrupts natural gait.
This can result in repetitive stress injuries in healthy people, so if you have fibromyalgia, this is all the MORE reason to walk naturally — that is, don’t hold on unless you need to steady yourself to change the settings or sip water—then let go once you’re done.
It may seem wise to hold on in the name of fibromyalgia, but on the other hand, holding onto a treadmill suppresses your body’s balancing mechanism—making you less efficient at movement.
If you have a pain disorder, the last thing you need is a suppressed balancing system.
The solution to arm pain while walking on a treadmill or outside, is to let the arms and shoulders move naturally, in synch with your lower body, the way nature designed your body to move.

Shutterstock/ LightField Studios
You can’t go wrong with natural movement when you have fibromyalgia.
Dr. Teitelbaum is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
is a board certified internist and nationally known expert in the fields of fibromyalgia, chronic fatigue syndrome, sleep and pain.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
What to Do After ADHD Diagnosis for Kids AND Adults

If you or your child’s been diagnosed with ADHD, you might really have sleep apnea and were misdiagnosed.
The symptoms of ADHD mimic the symptoms of sleep apnea.
It’s not at all uncommon for people (kids and adults) who’ve been diagnosed with ADHD, to actually have untreated sleep apnea instead.
People who have been labeled as “ADHD” should get tested for sleep apnea, which afflicts some 18 million Americans, and many don’t even know they have it.
What does the test for sleep apnea involve?
“Spend the night hooked to a machine that monitors your breathing, brain activity, eye movement, muscle tone and oxygen levels,” says Dr. Frank Barnhill, MD, board certified family physician practicing child and adult preventative care/ADHD-behavior medicine in upstate South Carolina.
Don’t let this description intimidate you.
The home test is quite simple: A device the size of a small TV is placed in your bedroom, and you simply clip a monitor to your finger at bedtime and snooze away with that on.
In the morning you remove it, and a technician will return to pick up the unit, which will have recorded all your overnight data. Or, you may drop it off at your medical office.
Sleep apnea is when a person stops breathing throughout the night (during sleep). Interestingly, the patient often is not aware of this.
The body’s autonomic nervous system kicks in and makes breathing resume, and the patient usually sleeps through these apnea episodes.
However, they leave their mark: Daytime symptoms that mimic ADHD are, says Dr. Barnhill:
“Irritability and impulsivity, poor concentration, difficulty maintaining focus, problems organizing, poor school performance.
“All of these occur as a result of not getting adequate rapid eye movement (REM) and deep stage sleep.”
What is sleep apnea?
In the early stages of sleep, a person (child or adult) begins snoring (obstructive sleep apnea), or develops “sighing breaths” (central SA or OSA-CSA combination).
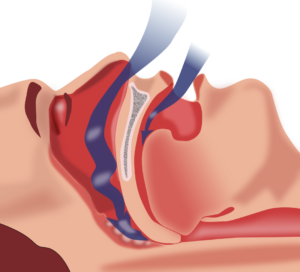
The obstruction in sleep apnea. Habib M’henni, Wikimedia Commons
As the SA progresses, respiration is interrupted by hypopneas (irregular partial breaths) or stopped breathing (apneas).
These breathing problems cause the person to either awaken with the sensation of struggling to inhale, or, the person only partially awakens and doesn’t remember the incident.
“Hypopneas are breaths that, while not normal, are at least partially effective in moving air in and out of the lungs,” says Dr. Barnhill.
“We call them mini-breaths — sort of like rapid shallow breathing. These episodes can occur hundreds of times a night.”
The individual ends up awakening throughout the night many times, getting no restorative sleep.
Fallout of Sleep Apnea
Being deprived of restorative sleep on a recurring basis means you’ll be prone to irritability, fatigue, even muscle aches, and “all of this causes problems with brain related functions such as short-term memory, thought processing, a decrease in the normal inhibition of impulsivity and aggressiveness (the judgment centers) and ability to maintain attention span,” says Dr. Barnhill.
The brain’s executive thought processing centers take a hit from the low oxygen levels caused by the sleep apnea. “It’s hard to think clearly when your brain is tired.”
If you don’t have ADHD and instead have sleep apnea, your ADHD medications will be pretty much useless.
However, it’s also possible that you can have both ADHD and sleep apnea.
ADHD is not a life-threatening situation, but sleep apnea can have life-threatening consequences.
Cardiovascular problems. The sudden drops in blood oxygen that result from stopped breathing can have devastating consequences, including sudden cardiac arrest.
Stroke and high blood pressure can also result, along with congestive heart failure and heart rhythm disorders.
Excessive fatigue. Though the patient is usually not aware of the apnea episodes, they do result in loss of restorative sleep, and this leads to daytime drowsiness, irritability, moodiness and poor concentration; those last three sound a lot like ADHD, right?
Other cognitive problems. Memory may be affected, and mood swings and depression may be present. You may even be a bit hyperactive.
Perhaps you believe that only overweight, thick-necked people get sleep apnea, and if you’re thin, you don’t believe you might have this condition and instead think you have ADHD.
However, sleep apnea can occur in skinny people, including children!
So if you’re a young adult with an ADHD diagnosis and weigh only 150 pounds, it would be smart to get tested for sleep apnea.
 In practice for 30+ years, Dr. Barnhill is the author of “Mistaken for ADHD.” He has additional training in Infant, child and adolescent medicine, urgent and emergent medicine, and gerontology.
In practice for 30+ years, Dr. Barnhill is the author of “Mistaken for ADHD.” He has additional training in Infant, child and adolescent medicine, urgent and emergent medicine, and gerontology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Sources: mayoclinic.com/health/sleep-apnea/DS00148/DSECTION=complications

How to Prevent Menstrual Migraine Headaches!

An OB/GYN explains causes of menstrual migraine headaches.
Migraine headaches can be caused by a woman’s period. These are referred to as menstrual migraines.
Though migraine headaches that come with a woman’s period can be painful and interfere with the day’s activities, they are nothing to become alarmed about.
For this article about migraine headaches related to menstruation, I asked Randy Fink, MD, Director of the Center of Excellence for Obstetrics & Gynecology in Miami, FL, if there was a way to prevent them.
Dr. Fink explains: “Some women suffer from menstrual migraine headaches. These headaches are thought to be caused by a drop in the normal hormone levels, leading to menstruation.
“When the brain realizes pregnancy has not occurred, it says, ‘Okay. Shut off the hormones, clean everything out, and let’s try again next month.’
“This is the signal to have a normal period. The falling off of the hormone level from normal is thought to be one cause of menstrual migraines.
“Therefore, one way of treating menstrual migraines is to use continuous birth control.
“By not letting the hormone levels drop (i.e., ‘skipping the period,’ menstrual migraines resolve in over 80% of women.”
What is the physiology behind why the drop in hormones causes these menstrual migraine headaches?
Dr. Fink explains: “Estrogen has many effects in the central nervous system. The serotonin system is one such place.
“A decline in the levels of estrogen (such as during the hormone free week of the birth control, or during the period week of a natural cycle) causes serotonin levels to fall. (This may be one mechanism for the mood changes associated with menses, or PMS.)
“Falling serotonin levels increase pain producing biochemicals; there is a release of calcitonin gene-related peptide and substance P from one of the cranial nerves, the trigeminal nerve.
“This leads to vasodilation of cranial vessels and sensitization of the portion of the nerve that supplies the meninges — the brain’s lining.
“Estrogen also affects other chemicals — magnesium, nitric oxide, prostaglandins — that alter nerve function and increase the sense of pain.
“There may also be a decrease in endogenous opioid activity.”
Another way to reduce migraine headaches that come with your period is to restrict the amount of sugar and processed foods in your diet, and to drink 6-8 glasses of water every day.

Creating an environment where the very best of medicine and gentle gynecology are practiced and where patients come first has always been Dr. Fink’s goal.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/wavebreakmedia

Why You Have More Sinus Headaches at Night

You may have read somewhere that one feature of sphenoid sinus headaches, or even those of general sinusitis, is that they tend to occur at night (while you’re still awake).
Or, if you have the headaches earlier in the day, they get worse as the evening wears on.
“There is no medical or structural reason to explain why a patient may have more sinus symptoms in the evening,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology; one of her specialties is sinus surgery.
“Some patients may be distracted by daytime activities which may find some relief only to find symptoms worsen when the distractions are gone.
“Ambulating helps move mucous and may also help relieve symptoms, and if sitting in one place at home for a while, the symptoms and pressure can build.”
This explains why, if you do some exercise in the midst of a sinus headache, the discomfort may subside or outright disappear, only to return once you stop exercise and assume a prolonged position before the TV or computer.
Dr. Silvers continues, “Position changes can worsen any type of headache. With sinus headaches if there is a fluid level in the sinus, with a shift of that fluid based on head position, headaches can worsen or improve.
“Patients will often complain about bending their head forward and may have relief when lying flat.”
However, lying flat can worsen a sinusitis head pain, which is why when someone has sinusitis, they often have a headache in the morning upon awakening.
Hours of lying flat have caused a buildup in the sinus cavities.
Bear in mind that a tension or stress headache feels very similar to that caused by sinusitis, and can be indistinguishable as far as symptoms.
For example, both types of pain “move” with the patient. That is, if the patient jumps up and down, he can feel the pain jumping up and down in his head. If he leans over, the pain seems to lean over inside his skull as well.
A tension (stress) headache will be more noticeable when you lean forward or bend over to tie a shoe.
A tension headache will also be associated with a lot of stress; they don’t just happen, and they tend to develop gradually.
However, a person can be afflicted with both a stress and a sinusitis headache.
Stress discomforts do tend to build up as the day goes on, and may reach peak discomfort in the evening.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image,hutterstock/Andrey_Popov

Does Angina Always Cause Chest Pain?

Does angina necessarily cause chest pain? Can you have angina and no chest pain?
Though it’s a strong fact that chest pain is a classic symptom of angina, or, to put it another way, that angina is a common cause of chest pain, it’s fair to wonder if every case of angina will always cause some chest pain.
“Angina or angina pectoris is the pain associated with poor blood flow to the cardiac muscle,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“It is typically described as pressure in the chest and can radiate to the neck, jaw, arm and back.
“Some patients may only have arm, shoulder or jaw pain with nothing in the chest, and others may only have a sensation of shortness of breath.”
People with angina typically have nitroglycerin tablets (available only with prescription) on them. Upon feeling the onset of angina symptoms, they take a tablet.
Nitroglycerin works by dilating all the blood vessels in the body, including coronary arteries.
This dilation allows more blood (and thus more oxygen) to flow through them, relieving the symptoms of chest pain, or whatever other symptom that the angina is causing.
Dr. Fiocco continues, “Rarely, ischemia (poor cardiac blood flow) will be without symptoms, i.e., without angina. This is most commonly seen in insulin dependent diabetics and it is unclear why.”
There Two Kinds of Angina
Stable and unstable.
Stable angina is the type that produces symptoms upon physical exertion or mental stress, but the patient feels fine when at rest or calm.
In unstable angina, chest pain, or shortness of breath, shoulder, arm or jaw pain will occur during rest for seemingly no reason, even during sleep, awakening the patient.
And of course, symptoms will occur during physical exertion and/or emotional stress.
Six to eight million people a year in the U.S. visit emergency rooms with complaints of chest pain, and some do end up eventually diagnosed with one of the two types of angina.
However, out of all those millions of people presenting in ERs across the nation with chest pain, only about 10 to 15 percent actually turn out to have some kind of heart problem.
Besides angina, other causes of chest pain include: aortic dissection, coronary spasm, inflammation of the sac surrounding the heart, atrial fibrillation, heartburn, esophageal spasm, inflammation of ribcage cartilage, gallbladder problems, sore muscles and panic attack, to name a few.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sukiyaki
Source: mayoclinic.com/health/chest-pain/DS00016/DSECTION=causes

How to Take Out Thick Ponytail without Pulling out Hair

Here is an ingenious way to take out a big thick ponytail without losing more than a few hairs.
I swear, every time I do this technique, I am very rarely aware of any hairs being pulled out along the way.
But even if one or two are getting by me (though again, I don’t feel the hairs being pulled out), this technique for sure is the best at minimizing hair loss when taking out a ponytail–particularly if it’s big, thick, poofy or bushy.
First, always use a rubber band designed for ponytails, and one that does not have a metal piece holding it together. Ideally, use the ones covered in cloth.
When it’s time to take out your ponytail, bend over so that your ponytail flops over the top of your head. This will clear your work area around the rubber band.
Pull one of the loops of the rubber band just enough to fit the tip of your index finger beneath it, between the underside of this loop and the other loop (or two) that binds the ponytail.
I use two loops of a single rubber band. Almost always, one of the loops lies a little higher than or on top of the other.
This is the one that I lift just enough to insert the tip of my index finger under.
I do this EXTREMELY CAREFULLY because invariably, there will be hair that is tangled with the loop. I do not want to break this hair.
My goal is to “clear” the loop of any hair, so that it’s just my fingertip against it—not a single hair caught in there.
The next step is how you will prevent losing the hair that normally results when you take out a ponytail.
Even if you very carefully remove the rubber band of your ponytail as you’ve always done, it’s almost impossible to avoid yanking some strands out of their roots.
So for this next step, you will need a toenail clipper—the kind with thin pointy ends–NOT the kind in which the ends get wider.
While you’re holding that loop, that you’ve already made sure is clear of any caught strands, you will carefully slip one of the tiny shears of the clipper underneath the band that’s being held out by the tip of your index finger.
Insert the shears under all the way so that when you close the other shear over it, it severs the entire width of the loop that you’re holding with your fingertip.
If you’ve “cleared” any caught strands, the clippers will snip ONLY the rubber band.
I do this entirely by feel. No mirror is necessary.
Snip the rubber band. Very carefully extract the severed rubber band from your hair—so that you don’t snag any strands with it.
DO THIS SLOWLY. If you just yank it out, you’ll pull hairs with it.
This technique means you must have a steady supply of rubber bands–and for thick or bushy hair, you’ll need strong rubber bands.
You will have to keep buying them. But hey…your hair is worth it, right?
For women who have palm calluses from lifting weights, strands of hair can get caught by these.
The solution is to use a fingernail fail to file at the calluses so that they are smoother.
While working with your ponytail, try not to press the callused area of your palms into your hair.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Skin Peeling On Your Hands: Doctor Explains Causes

If you’re suffering from peeling hands, there are many causes of this, says a dermatologist.
“Each and every day your hands are constantly being exposed to various elements that can cause irritation including chemicals, UV rays, weather conditions, irritants and allergens,” says Dr. Jennifer Gordon, who is board certified by the American Board of Dermatology and practices at Westlake Dermatology located in Austin, Texas.
“Repeated irritation of the skin on the hands can lead to excessive peeling, especially if you are genetically predisposed to this.”
Says Dr. Gordon. “Typically this peeling is accompanied by other symptoms like itching, burning or pain, making the situation even worse.
“Unfortunately diagnosing the source of this peeling can be difficult, as there are a number of potential root causes.”
Causes of Skin Peeling on the Hands
(no particular order)
Yes, believe it or not, stress can cause the skin of your hands to peel. “It’s not uncommon for people to experience peeling of the skin (in any area of the body, including the hands) due to periods of high or intense stress,” says Dr. Gordon.
This is because usually, stress exacerbates other conditions (following) that can lead to peeling hands.
Allergies: “Skin peeling may be the result of your skin coming into contact with a substance that you are allergic to,” says Dr. Gordon.
“Potential allergens can be found everywhere, including household items, foods and even skincare products.”
Infections: “Certain staph and fungal infections are known to cause skin peeling. Sometimes these infections occur alongside other symptoms like high fever.
“The infection may be in your skin or may be elsewhere in your body, so if you have any other symptoms, make sure to see your provider quickly.”
Eczema: “Hand eczema is characterized by a peeling of the skin on the hands as well as the fingers.
“This type of eczema is caused by genetics, but is worsened by triggers, with many individuals developing it after being in contact with chemical irritants or allergens.
“Other symptoms can include itchiness, development of fluid-filled blisters, swelling and cracking skin.”
Psoriasis: “Generally occurring due to genetic disposition, psoriasis can result in peeling along the hands.
“Psoriasis occurs with skin cell buildup in a specified area; resulting in irritating red patches, itchiness, peeling and sometimes pustules.”
Exfoliative keratolysis: “While this condition is characterized with peeling of the fingers, peeling of the palms or tops of hands is possible. Exfoliative keratolysis is mostly common in young adults and occurs during the hotter summer months.
“The peeling starts off with the development of a superficial blister which naturally pops and results in peeling skin.”

Dr. Gordon’s interests include medical dermatology, particularly the treatment and prevention of melanoma and other skin cancers in athletes. For 2016, 2017 and 2018 Texas Monthly Magazine selected her as one of the Texas Super Doctors Rising Stars.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}