
Benign Cause of Food Tasting Soapy

If your food sometimes tastes soapy, there may be a perfectly benign explanation for this.
Every so often I was noticing a soapy taste to my food.
I had always suspected that it was due to residue from the bar of soap at my kitchen sink making its way to the food.
When I began getting very strict about this, the periodic soapy taste disappeared.
What to Do if Your Food Tastes Soapy

Make a note of which foods seem to have the taste of soap in them.
After a while you may notice that it’s only certain foods. In my case it was only steamed vegetables.
Then ask yourself if those particular foods can, in even the most remote sense, come in contact with either dishwashing liquid or bar soap.
Also ask yourself if there’s any tiny soap splatter going on when the kids are helping you wash the dishes or just playing around.
Tiny drops of splatter could be making their way onto your bowl of fruit sitting on the counter.
In my case, I was washing my hands with the bar soap in the sink — and the sink was empty — there were no utensils or anything there.
Then at some point after, I’d use a strainer to rinse some chopped broccoli or cauliflower, then place the strainer over a pot of boiling water.
When I was done, I’d place the strainer in the sink. The bottom of it, of course, was making contact with the sink — where hours earlier, I had washed my hands with bar soap.
Though water had been running during that task, and also during the rinsing of the vegetables, it wasn’t enough to completely obliterate invisible soap residue on the sink that resulted from washing my hands.
And this residue was getting on the strainer. Next time I used the strainer, that residue would then make contact with the vegetables — and stay on them — even though I was rinsing them.
Then I’d steam them — and the residue would remain, and ultimately make its way to my mouth when I ate the vegetables — and hence, I’d taste soap.
It takes only a very tiny, tiny amount of soap residue to be detectable by your tongue.
Another way that soap can get into your food is if soap bubbles (that you may not see) are being released, and land on a plate that’s been sitting out, and then you put food on that plate — and it picks up the residue from the bubbles.
A fork, knife or spoon, left in a sink where you had been washing your hands with soap, could easily pick up invisible residue.
Then you use that utensil to eat, and voila, your food tastes soapy.
Prevent a Soapy Taste in Your Food
• Make it a rule: Any utensil or other food implement that ends up in the sink—you don’t use until it has been washed with the dishwasher.
If you accidentally place a perfectly clean item there, you can’t eat with it; assume it has soap residue, even if the last time you used soap in that sink was a few days ago.
• If you hand-wash your dishes, with a sink full of suds, make sure that there are no clean plates, utensils or glasses within “bubble-landing range.”
Have them all in the cupboards or drawers. In short, nothing that you’re going to be using to eat should be capable of catching airborne bubbles.
• Watch where you place utensils including spatulas. Did you just wipe the counter with a soapy substance to clean it? Then you placed a butter knife there?
Then you use that knife to put butter on your toast — and your toast tastes kind of soapy?
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com
Cloudy Urine and Changing Colors: Serious vs. Harmless

Cloudy urine can mean trouble.
So can certain colors of urine like cola colored or tea colored.
Cancer can cause urine to change colors. So can many other conditions including very strenuous exercise (dark color).
“Cloudy urine can be due to dehydration (concentrated urine), urinary tract infection (bacteria), blood in the urine, crystals in the urine (such as patients with kidney stones), elevated urine glucose (sugar) or medications,” explains Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
“Medications can change urine color,” continues Dr. Besser. “For example, OTC bladder infection medications; ‘AZO’ can turn urine orange; some vitamins can turn urine green or blue.”
Dehydration, even though you may not feel thirsty, can result in orange urine – which can be mildly murky or “cloudy,” or crystal clear.
Wide Color Range of Urine
Your flow can appear in a wide range of colors: cloudy, clear-yellowish, light yellow, medium yellow, dark yellow, bright yellow, orange, pinkish, red, maroon, tea, light brown, dark brown, and of course — green, greenish-blue and blue.
Sometimes, the color of the flow can be the gateway to your health or your body’s current medical or dietary status, be it cloudy, bluish-green or dark brown.
When it is bright, dark yellow or light orange, this usually means you are dehydrated, even though you may not feel thirsty.
To know if you’ve been getting enough water, simply check the color of your flow.
Flow should be a light yellow, which can also be described as clear-yellow, medium yellow or — in cases of well-hydration, like ginger ale.
Cloudy Urine: When to Worry
This is a Q & A interview with a urologist – Go to article
——-

Shutterstock/Igor Nikushin
Orange Urine: Causes, Solutions
A urologist explains causes and what to do – Go to article
——-
Top 8 Causes of Blood in the Urine
The image at the top of this article shows “gross hematuria,” which means visible blood in the urine.
A urologist provides information including about cancer as a potential cause – Go to article
——-
Dark or Brown Urine
Causes and solutions are given by a urologist. Most causes of dark or brown flow are serious, and there are quite a few causes – Go to article
All in all, the causes of color changes can either be quite benign and very interesting; or, are a symptom of a moderately-serious or easily treatable medical condition; or, are a symptom of a disease that can kill you.
Thus, it’s important to keep tabs on the color of your flow, and it will help to know which colors are the colors you never need to worry about.
Foamy Urine
Flow can also be foamy, and here’s information from a urologist about that.
Urologist Defined
A urologist is a medical doctor who specializes in the urinary tract.
You should check the color of your urine on a regular basis, and also check to see if it’s excessively murky or cloudy. Catching your urine in a clear plastic cup will allow you to accurately see what it looks like.
More on Blue or Green Urine
Explained by a urologist: Go to article
 Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Top image: James Heilman, MD

How to Relieve Muscle Cramps from Clavicle Fracture

Here is a non-drug way to instantly relieve muscle cramps from a clavicle fracture.
One day I experienced a hairline fracture to my clavicle — after having a freak fall while using an exercise stool for high-step aerobics.
Multiple times a day I’d get sudden cramping or a deep aching in the surrounding tissues: deltoid, triceps and the muscles of the scapula such as the middle trapezius.
Instant Relief from Muscle Cramps Caused by Clavicle Fracture
Most people might not ever think to massage the aching area. But that’s what I decided to do.
Give the cramping area your deepest, hardest massage — but do not massage or press down on the clavicle itself.
Knead and work the aching muscles.
For me, one minute or so of this made the cramps disappear — and they would stay gone for quite a while.
There is a caveat to this solution: Your fingers/wrist will fatigue quickly — unless you’re a trained massage therapist, rock climber or piano player.
The good news is that you need to bare with the hand fatigue for only about a minute.
Be vigorous and deep, like an expert massage therapist would be.
For those of you versed in anatomy, you’ll want to get a good kneading of the infraspinatus and teres minor (if these areas are aching).
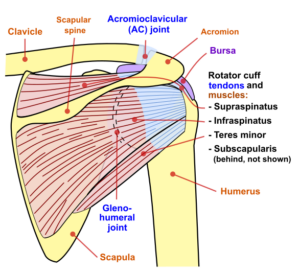
Back of the shoulder. Jmarchin, CC
For those of you familiar with the art of massage, you may discover a few “knots” in these areas. Press upon them and hold for 10 seconds to release them.
No kidding, 100 percent of the time I massaged my shoulder “complex” upon developing cramping or aching in that area, these symptoms full-out disappeared after only a minute or so.
My physical therapist said this was because the massaging promotes circulation — which is reduced when the shoulder is immobile for too long — which a person with a clavicle fracture may feel inclined to do throughout the day.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/pickingpok

Cause of Muscle Cramping from Clavicle Fracture

Do the muscles around your shoulder cramp up since you’ve had a clavicle fracture?
How does a bone break cause muscle cramping?
While your clavicle fracture heals, you may be experiencing sudden cramping or deep aching of the muscles surrounding the joint: deltoid, triceps, upper back muscles on the side of the injury.
I recently suffered a hairline clavicle fracture. I was getting frequent attacks of cramping or deep aching while sitting at my computer and also while walking on my treadmill desk. Sometimes the cramps would occur while I was watching TV.
What do these three activities all have in common? Minimal movement of the shoulder.
Now you’re probably thinking, “Well, the GOOD shoulder doesn’t move much, either, save for handling the mouse and hitting Return on the keyboard.
Actually, if you’re sitting at your computer or TV with a clavicle fracture, the “good” shoulder is going to be moving more. The good shoulder will probably be handling the remote.
In my case, my good shoulder was also my dominant arm, so this meant that the injured side was especially immobile.
What causes the muscles around the shoulder in a fracture clavicle patient to cramp up or suddenly develop deep aching?
My physical therapist told me it was…inactivity. Certainly, do not engage in movements that promote the pain of the injury, but at the same time, don’t overprotect the shoulder by freezing it up while you’re watching TV or at the computer, either.
Medical Doctor’s Explanation
I wanted a doctor’s take on this, so for this article I asked Carolyn Dean, MD, ND, Medical Advisory Board Member, Nutritional Magnesium Association at nutritionalmagnesium.org.
Here is what Dr. Dean explains: “The force that causes a fracture can leave the muscles and tendons inflamed and painful.
“Also any fracture will cause inflammatory products to flood the area, increase the lymph node size and lymph drainage and cause referred pain to the shoulder and triceps.”

Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Photographee.eu

Cause of Morning Pain from a Clavicle Fracture

Do you experience morning pain in your shoulder due to a clavicle fracture?
The pain may be described as a deep soreness, and is evident when the patient gets up to exit the bed.
It will also be evident if they move the arm around in bed. This morning pain or soreness may feel as though the patient had spent the entire night sleeping smack on the shoulder with everything getting scrunched.
However, this pain upon awakening can easily occur if the patient has spent the entire night sleeping on their back, with their arm lying straight out at their side.
What is it about a clavicle fracture that causes morning arm pain or soreness?
Five months ago I sustained a hairline fracture of my clavicle. I asked the physical therapist what causes the morning soreness.
He said it’s due to the injured area overnight becoming stiff and accumulating fluid (even though you may not see any swelling).
The soreness quickly dissipates or reduces once you’re up and about (i.e., moving the shoulder, even if it’s in a sling; there is still more movement than if you’re lying there in a deep sleep).
I asked him why this morning pain is greatly reduced if I sleep with my arm propped up on a pillow that’s on my chest. He said it’s because of making it more comfortable.
That last answer doesn’t quite explain it for me, but I decided to post this article anyways, because his first answer makes sense.
The PT added that despite morning pain in the patient who has a clavicle fracture, this soreness does NOT mean that anything was injured overnight.
Sports Doctor’s Response
“Fractures or broken bones typically cause pain when there is abnormal movement of the broken bone ends rubbing against each other,” says John-Paul H. Rue, MD, orthopedic sports medicine surgeon with Orthopedics and Joint Replacement at Mercy Medical Center in Baltimore, MD.
“It’s possible that at night, without realizing it, you may be rolling over on your shoulder or somehow causing increased pressure on the fracturef clavicle, causing stress at the fracture site, and maybe even movement, leading to pain.”
 Dr. Rue specializes in prevention and treatment of sports and exercise injuries. His primary focuses are knee, shoulder and elbow injuries including ACL and cartilage injuries, rotator cuff injuries and overuse tendonitis.
Dr. Rue specializes in prevention and treatment of sports and exercise injuries. His primary focuses are knee, shoulder and elbow injuries including ACL and cartilage injuries, rotator cuff injuries and overuse tendonitis.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Rustle

OVARIAN CANCER: the Deadliest Woman’s Cancer

Ovarian cancer is a stealthy killer, creeping up without warning and murdering thousands of women every year.
So creepy is this monster that there’s still no way to effectively screen for its presence. The Pap smear does not screen for this disease.
Usually this malignant illness lets its presence be known only after it has spread beyond the ovaries—making prognosis grim.
The symptoms can very closely resemble those of benign conditions, which is why this ruthless disease is one of the most misdiagnosed out there.
The symptoms of ovarian cancer are often vague as opposed to pronounced, severe or dramatic.
However, they tend to be persistent. And that’s a red flag.
The most suspicious signs that may mean ovarian cancer are “persistent lower abdominal pain with abdominal swelling and fluid accumulation in the lower abdomen/legs,” says Mark Levandovsky, MD, Founder and Medical Director of Preventive Medicine and Cancer Care.
Dr. Levandovsky is a board certified internist and oncologist/hematologist in practice for 25+ years.
The fluid accumulation is called ascites (uh-sight-eze). The presence of this fluid usually causes appetite suppression.
Misdiagnosis
One of the conditions that OC can be mistaken for is irritable bowel syndrome. This has happend quite a few times, especially in younger women.
Ovarian cancer is one of the most evil terrorists out there — why isn’t there yet an effective treatment?
What are world leaders doing about this killer that can even strike women in their 20s?
You’ll likely find your questions answered in one of the articles below…
All About Symptoms
- Symptom comparison of ovarian cancer pelvic pain to IBS
- Q & A with doctor about ovarian cancer’s symptoms
- How the symptoms of colon cancer compare to that of ovarian cancer
- Why does loss of appetite come with ovarian cancer?
Risk Factors for this Deadly Disease
Ovarian cancer’s known risk factors are as follows: Age over 55; family history; BRC1 and BRC2 mutations; previous breast, colon or uterine cancer; and zero pregnancies.
Studies show that women who’ve never been pregnant (nulliparity) have about a 24% higher risk when compared to women who’ve had at least one child.
This is due to the “incessant ovulation theory” which suggests that repeated ovulation without interruption from pregnancy contributes to cancer development.

Dr. Levandovsky provides personalized care to health conscious individuals as well as cancer patients and survivors, focusing on an integration of genetic/molecular risk assessments, prevention, education, nutrition and psycho-oncology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer. .
Top image: Shutterstock/Chinnapong

CALCIUM SCORING for Heart Disease Detection

The coronary calcium score test is an excellent screening tool for heart disease.
The calcium score number closely correlates to the likelihood of having coronary heart disease: mild, moderate or severe.
It also closely correlates to the likelihood of having a cardiac event in the next several years.
“Calcium scoring is an additional tool to assess cardiovascular risk,” says Nieca Goldberg, MD, medical director of NYU Women’s Heart Program and radio show host of “Beyond the Heart” on Doctor Radio SiriusXM.
Dr. Goldberg explains, “I use it in individuals who have an early family history of heart disease: a father less than 50 or mom less than 60 when they had their first heart attack.”
Dr. Goldberg also uses the calcium scoring for “people who have intermediate risk for heart disease, meaning, they are not clearly high or low risk.”
Most people have never undergone a calcium score test. Many don’t even know what this is.
Others think it’s too expensive, but the test can run between around $200 and $300–well worth it.
It takes only about five minutes, too. If you know that your calcium score correlates to mild coronary heart disease, you can then take measures to help prevent a progression such as quitting smoking and starting an exercise program.

Freepik.com
Don’t be in the dark about what’s going on inside your coronary arteries, like so many people are — and then one day they drop from a heart attack — that probably could have been prevented.
If you have a question about the calcium score test for detecting the likelihood of heart disease, check out the article links below.
A coronary calcium score can theoretically exceed 4,000. Yet scores over **400** already indicate extensive plaque and high cardiovascular risk.
Very high scores reflect widespread calcification but do not directly measure artery blockage severity; clinical context and imaging will guide treatment decisions.

“Can I be too young to have coronary artery disease?”
 Dr. Goldberg is senior advisor, Women’s Health Strategy, NYU Langone Health; founder and former medical director, Joan H. Tisch Center for Women’s Health; and clinical associate professor, NYU Grossman School of Medicine.
Dr. Goldberg is senior advisor, Women’s Health Strategy, NYU Langone Health; founder and former medical director, Joan H. Tisch Center for Women’s Health; and clinical associate professor, NYU Grossman School of Medicine.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/pickingpok
INSULIN RESISTANCE: Dangerous Harbinger to Diabetes

If you’ve been diagnosed with insulin resistance, you’re on a collision course with type 2 diabetes.
Make no mistake, insulin resistance – though it may sound rather benign – is a setup for the No. 1 cause of blindness and amputation in the U.S.: type 2 diabetes!
Insulin Resistance: Forerunner for Type 2 Diabetes
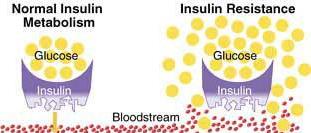
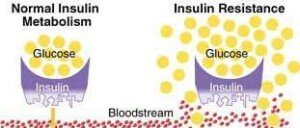
“In type 2 diabetes, the body becomes resistant to insulin,” says Susan L. Besser, MD, with Mercy Medical Center, Baltimore; Diplomate, American Board of Obesity Medicine and board certified by the American Board of Family Medicine.
Dr. Besser explains, “That means, even though the body is still producing insulin, it is working less efficiently to move glucose (sugar) from the blood into the body cells where it is used as energy.
“In the insulin resistant stage (prediabetes), the body is able to manufacture enough insulin to offset its inefficiencies.
“However, over time the pancreas (where insulin is made) tires and can’t keep up with the demand. Then you go from insulin resistance to frank type 2 diabetes.”
Insulin resistance may also be referred to as impaired glucose metabolism.
Call it what you may, but it is a stealthy condition that creeps up on men and women … even though it has very identifiable causes and risk factors.
Do you know your numbers?
Many people have NO idea what their fasting glucose number is or what their A1c number is.
These are easily determined with a simple blood test. Have you had yours taken?
Prediabetes IS reversible.
This is not achieved with a magic pill, but with sensible lifestyle changes.
And don’t think for a second that being thin protects you from insulin resistance or type 2 diabetes.
Other risk factors include a diet high in processed foods (even if you’re not overweight) and a sedentary lifestyle void of structured exercise.
Nevertheless, obesity is a major risk factor for disorders of glucose metabolism.
Did you also know that chronic stress and anxiety could give rise to insulin resistance?
Are you continually under stress? Have you found that it’s just impossible to get away from the stress and anxiety in your life?
This can have a really bad effect on your glucose metabolism!
Dr. Besser provides comprehensive family care, treating common and acute primary conditions like diabetes and hypertension. Her ongoing approach allows her the opportunity to provide accurate and critical diagnoses of more complex conditions and disorders.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

WHY You’re Starving the Day After Leg Workout

Okay, you know it happens, but here’s WHY you’re freaking starving the day after a badass leg workout!
You thrashed your legs in the gym, and usually a grueling leg workout includes at least one of two famed compound exercises: the back squat and the deadlift.
But other leg movements can also be very taxing: leg press, hack squat, front squat, weighted lunge, squat overhead press hybrid, and more.
When these exercises are done at intense levels, they drain the muscle cells of their fuel source: glycogen. Glycogen refers to the blood sugar that’s stored in muscle cells.
Muscle cells need this substance for fuel—not just to function, but to recover from a gym thrashing.
If your leg workout is punishing enough, your muscle cells will be left in such a deficit that they’ll be gulping any glycogen that comes along.

Shutterstock/Olena Yakobchuk
Glucose (blood sugar) is transported to the muscle cells via insulin, which is secreted by the pancreas.
The insulin shuttles glucose to the insulin receptor sites on muscle cells—where the transfer occurs, fueling the muscle cells.
If this transport service can’t keep up with the recovery demands of thrashed muscle fibers, then this means that the blood sugar levels are too low.
Low blood sugar will cause hunger.
The day after a leg workout, blood sugar levels may still be low, resulting in crazy hunger.
Athletes who suffer with this often claim that they keep eating and eating, but the hunger persists all throughout the day after their strenuous leg workout.
The supply (food) is not matching the demand (muscles starved for recovery fuel).
But why is this hunger so pronounced the day after the leg workout rather than the day OF the leg workout and leading up to bedtime?

Shutterstock/Photology1971
Though some muscle-building enthusiasts report insane hunger in the hours after the leg workout on the same day, many report that their appetite becomes a bottomless pit only on the day after.
Are you eating enough carbs or is it mostly meat/fish, low carb protein shakes (hardly satisfying) and low carb produce?
When blood sugar gets too low, this causes a signal to go to your brain that translates to FEED ME! I’M STARVED!
If you’re truly cramming down a lot of food and still suffering with hunger, you’re eating the wrong foods.
Processed foods from the supermarket, fast-foods and restaurant foods are notorious for stimulating hunger.
Even if you eat a “heavy” meal of such, don’t be surprised if two hours later you’re famished.
“Fatigue, tiredness, lack of sleep can stimulate hormones that make you feel hungrier than you actually are,” says Carolyn Dean, MD, ND – Medical Advisory Board Member, Nutritional Magnesium Association at nutritionalmagnesium.org.
Solutions to Insane Hunger Day after Leg Workout
• “Recovery from such workouts by supplementing with magnesium and other electrolytes and making sure you get enough sleep for recovery is the best remedy,” says Dr. Dean.
• Loading up on protein and low carb vegetables may fill up your stomach, but will do little to raise blood sugar; hence, you may still feel famished after two chicken breasts and a pile of steamed broccoli.
• Many muscle builders are hesitant to eat more on the day following a leg workout because they’re in a cutting phase or trying to lose excess body fat.
But depriving drained muscle fibers of needed recovery fuel will impede growth.
You must find that right balance, that sweet spot, that subdues raging hunger yet won’t cause fat gain.
• Opt for healthier high carb foods such as naturally sweetened oats, a boiled potato, barley, brown rice, quinoa or geez, even a whole grain (all natural) bagel.
Have protein alongside the carb dense food.

• Plan and be logistical, rather than spontaneous and frustrated.
Have a second potato and a tossed green salad and yogurt an hour later rather than mindlessly cramming down highly processed mac ‘n cheese and an ice cream bar.
• Loading up on water to kill the hunger won’t work. Drink water for its many benefits, but accept the fact that water intake won’t replace depleted blood sugar.
Face it; it’s a part of life: You will likely be crazy hungry the day after a crucifying leg workout!
Dr. Dean, in practice for 35+ years and author of “The Magnesium Miracle,” is also a naturopath, nutritionist, herbalist, acupuncturist, lecturer and consultant.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Monkey Business Images

How an ER Doctor Diagnoses a Transient Ischemic Attack

If you suspect you just had a transient ischemic attack (TIA), get to the ER stat (have someone drive you) so that a doctor can make a diagnosis.
It’s interesting to wonder just how a transient ischemic attack is diagnosed in the emergency room.
After all, when the TIA event is over, which may last less than a minute, the patient may have no symptoms to show for it by the time they get to the emergency room.
“A TIA is, by definition, a transient ischemic attack,” begins Rob Lapporte, MD, who is board certified in emergency medicine.
How a TIA Is Diagnosed in the Emergency Room
Dr. Lapporte continues, “In an ER setting, in order to meet criteria, a patient would have to:
-Have stroke-like symptoms within the last 24 hours
-Have a CT scan that showed no evidence of bleed or infarct, and
-Have complete resolution of his/her symptoms prior to being released from the ER.”
The “bleed” that Dr. Lapporte mentions refers to bleeding in the brain.
A chronic subdural hematoma, which is a common type of bleeding in the brain among the elderly, produces symptoms that are clinically indistinguishable from that of a TIA, other than that they are persistent rather than transient.
A TIA Can Be Misdiagnosed As a Stroke
“Sometimes patients are diagnosed with a stroke from the ER, and the symptoms resolve within a few hours,” says Dr. Lapporte.
“At that point his/her diagnosis would be a TIA rather than a stroke because of the transient nature of the symptoms.”
Symptoms of a TIA (or stroke) include:
#1 Sudden one-sided weakness or paralysis, which can also occur in the face
#2 Sudden-onset double vision, or a sensation that a shade is being pulled over one eye, obstructing vision
#3 Sudden heaviness or numbness on one side of the body
#4 Sudden clumsiness on one side of the body
#5 Sudden slurred speech or difficulty forming words
#6 Sudden cognitive difficulty or understanding speech
#7 Sudden severe headache
#8 Sudden difficulty swallowing
If these symptoms pass after only 30 seconds, this is just as emergent as if they were persisting for two hours.
GET TO THE ER for a proper diagnosis, whether it turns out to be a transient ischemic attack or some other condition.
 Dr. Lapporte has been practicing evidence-based clinical medicine in emergency rooms and urgent care centers for 25+ years. His experience includes that of medical director for Legacy ER and Urgent Care.
Dr. Lapporte has been practicing evidence-based clinical medicine in emergency rooms and urgent care centers for 25+ years. His experience includes that of medical director for Legacy ER and Urgent Care.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}