

Why Women Love the Hip Abductor Machine

So why do women love the hip abductor machine, and men don’t care for it so much?
The hip abduction machine targets two buttocks muscles: the gluteus medius and the gluteus minimus.
However, if you’ve ever used the hip abduction machine, it feels as though the outer thighs are being worked more than the butt.
The diagram on the hip abduction machine shows the area of the lower body that gets worked, and the outer sides of the thighs are highlighted.
Women see this and believe that hip abduction exercise will shave inches off their outer thighs.
Women, so much more than men, are concerned about excess fat in the thighs, particularly the outer thighs.

This is a hot button for throngs of women, and that’s why they gravitate towards the hip abduction machine.
However, another group of women uses the hip abduction machine to tone the buttocks.
Remember, this equipment targets the gluteus medius and gluteus minimus, which are buttocks muscles.
These muscles, though, are responsible for the joint action of hip abduction.
This joint action, against resistance, either with equipment, tension tubing, calisthenics or inline skating (especially up hill), will tone and strengthen these buttocks muscles.
But working these muscles will not – absolutely will not – take inches off the outer thighs!
These are small, relatively weak muscles. They do very little to power the legs during running, strenuous walking, hiking, and exercises like squats, deadlifts and leg presses.
To shave inches off the outer thighs, a woman must increase her body’s energy demands.
There is no better way to do this than to do exercises that target large muscle groups:
- the quadriceps (front thigh muscles
- hamstrings (back thigh muscles)
- gluteus maximus (main buttocks muscle; it’s bigger than you think)
- and large upper body muscles (back and chest).
Targeting these muscles with very challenging resistance loads — as shown in the following images — will force the body to use stored fat – including fat stored in the outer thighs — for recuperative energy!

Deadlift. Shutterstock/Tyler Olson

Sled push

Dumbbell deadlift. Shutterstock/Robert Taylor

Lat pull-down, wide grip

Dumbbell shoulder/chest press
Combine this with high intensity type of cardio and sensible eating habits, and voila, a woman will experience inches lost in her outer thighs.
As for that hip abduction machine, it’s a good piece of equipment to tone and strengthen the smaller butt muscles.
It’s also great to keep these muscles in shape for inline skating if you haven’t been inline skating for a while due to injury, lack of time or cold weather.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/lunamarina
Top Six Ways Men Can Be Rude at the Gym

Men can be very rude at the gym in ways that you just don’t see with the gals.
You’ve read about how people, in general, can be rude at the gym, breaching gym etiquette left and right. (more…)

Revolving Staircase vs. Real Staircase: Pros & Cons

So which workout is better, the revolving staircase or an actual staircase?
Wow, this is a real interesting question to answer, but as a former personal trainer for a health club, I will happily address it. (more…)
High Intensity Interval Training on a Revolving Staircase

Here’s the revolving staircase ultimate fat burning HIIT routine to blast off fat all through your body. (more…)

Dealing with Rude Gym Behavior: Solutions that Work

Rude gym behaviors require clever, effective ways of dealing with them that will not only cease the rudeness, but may even net an apology.
At a minimum, if you practice these witty ways of dealing with rude gym behavior, you’ll walk away feeling good and empowered, rather than miffed and upset for the rest of the day.
Do any of the following rude behaviors at the gym ever happen to you?
Sweat on the Equipment
Say, “Excuse me, but do you have a towel I can use to wipe up your sweat?”
I’ve done this several times, and in every single case, the offender apologized.
Water All Over a Locker Room Bench
If you know who the offender is, point to the puddles and say, “Oh, make sure you don’t sit here; someone left water all over the bench.”
(This ploy got me a confession and apology.)
Loud Grunting
When this gets pretty loud and frequent, it qualifies as inconsiderate. I myself have grunted — but I kept the volume controlled.
Sometimes you just can’t help it when you’re straining for the last repetition of a giant lift such as the deadlift, squat or bench press. But isolation moves?
Now remember, I’m talking about excessive grunting — and loud. I once said to a man, “You sound like you’re in a lot of pain.”
The man responded to me, “That’s the way it’s done,” but then wasn’t as loud afterwards.
Sitting on a Machine for a Long Time Doing Nothing
People who do this are short-sighted. They should know that by getting off the equipment for a long rest, this signals a nearby person that they can get in a set.
Stand near the equipment so that nobody actually takes it from you while you’re resting, but do expect someone to come over and ask if they can “work in.” And let them if it won’t interfere with your rest time.
As for that nearby person who’s wondering when someone who’s still sitting on the equipment is going to do another set, simply ask if you could “work in.” Often they’ll hop off the seat as though they have ants in their pants.
You can add humor to dealing with rude gym members.
Blocking a Mirror
This happens often to me, but it’s nothing that a passionate, “Excuse me, can you move so I can watch myself?” can’t cure.
About half the time, the offender appears annoyed, but they comply nevertheless.
Please, people, before you begin that set on your feet…make sure you’re not standing between the mirror and someone on equipment (which they cannot move) who’s facing the mirror. Step out of their line of sight.
Child Running Loose in Locker Room
Say, “Did you know that the daycare is open now?” If daycare is closed, say, “Excuse me, but there’s water on the floor and your child might slip and fall if she continues running all over the place in the locker room.”
If the offender gets sassy, point out that they should not let their child run loose in the locker room. It IS your business, even if the floors are bone dry.
One time when I was in a locker room, a few young kids were playing “I’m hiding in the lockers!”
When members opened lockers, the kids popped out at them. This is what happens when their mothers are not called on letting their kids use the locker room as a playground.
Toddler Wandering on Gym Floor
Does anyone NOT realize how risky this is? Never ignore this; say something to the parent! This goes beyond rude; it’s reckless.
One time a man — presumably a potential new member checking out the gym — was permitting this; toddler began exploring around a few stools that I had begun setting up.
There was no sales rep nearby, so I don’t know what the man was doing there.
I turned my back one second, then discovered the toddler under the stool I was about to use; father did nothing.
‘I said, “It’s against club policy to let your child in this area; it’s dangerous.”
He replied, “It’s not for YOU to worry about.”
I responded. “That’s right; it’s for YOU to worry about.”
I then marched to the front desk and reported the problem. Staff wasted no time following up on my report.
Locker Room Bench Cluttered with Belongings
A passive response to this inconsiderate behavior is to nonchalantly begin nudging aside their belongings to make room for yours or your body.
In my case, 100 percent of the time, the offender promptly gathers or moves their belongings and usually apologizes; never any hostility.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/UfaBizPhoto
Can Headache Be the Only Symptom of Sphenoid Sinusitis?
If you have an annoying headache but no sinus symptoms like nasal congestion or an aching or runny nose, can this solitary symptom be caused by sphenoid sinusitis?
“Headache can be the only symptom of sphenoid sinusitis,” says Dr. Stacey Silvers, MD, of Madison ENT & Facial Plastic Surgery in NYC, who is board certified in otolaryngology.
There are four sinus groups: sphenoid, ethmoid, frontal and maxillary. They are hollow cavities within the skull and can become infected or inflamed, causing a headache.
What is the function of the sinuses? Dr. Silvers explains that they produce a liter of mucous a day, “which helps us warm, filter, moisten the air and help digest our food.”
The next function is that they “aerate the skull (imagine if sinuses were solid bone or full of soft tissue). The head would weigh more and be exhausting to carry around.”
Finally, says Dr. Silvers, “They act as airbags to the brain: If an unfortunate trauma occurs to the face, the sinuses collapse, protecting the posterior vital structures.”
Headaches arising from specific sinus groups can have distinguishing characteristics, such as location.
A headache can definitely be the only symptom of this common condition that can go undiagnosed for a period of time before finally being correctly identified.
Dr. Silvers continues, “This (sphenoid) can occasionally be the only sinus involved. Patients may have no fever, congestion, or cough. The headache will present on the top of the head.”
Sometimes the sphenoid headache is felt in the upper back of the head, or between the top and the upper back.
“As it is not a classic location for sinus headaches, the sinuses may be overlooked as a cause,” says Dr. Silvers.
“A primary care physician does not have the tools to look into the back of the nose. Even an ENT (ear, nose and throat doctor) can have some trouble visualizing the sphenoid sinus opening depending on variations in patient’s nasal anatomy.”
So what would be a clue, then? Dr. Silvers explains, “Suspicion should arise based on the location of the patient’s pain which is typically on the top of the head.
“If a physical exam does not reveal the cause, then a CT scan of the sinus may be justified. With a sphenoid sinus infection the CT scan will show an air fluid level in one or both of the sphenoid sinuses.
“This may be found with or without congestion and swelling in the other sinuses.
“A proper treatment plan with decongestants, sinus washes, antibiotics and occasionally a steroid taper will quickly relieve the patient’s symptoms.”
How would the physical exam be conducted? A physician uses a lighted viewer to peer inside the nose, where swelling can be visible.
The doctor will also tap or press on the patient’s face to see if this brings on pain.
If you’re concerned about the radiation from a CT scan, ask your doctor about testing via MRI, endoscopy or sinus cultures to test for the presence of an infection or inflammation.
 An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
An NYC expert in ear, nose and throat care, Dr. Silvers has been named among America’s Top Physicians and Surgeons in facial plastic surgery and otolaryngology numerous times since 2003. Dr. Silvers is an expert in the field of minimally invasive rhinology, resolving patients’ breathing and sinus problems with simple in-office procedures.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick
Source: webmd.com/allergies/picture-of-the-sinuses

HIIT Q & A: High Intensity Interval Training All Questions Answered

Common Questions About HIIT Answered … for the already-fit to the very out-of-shape, overweight or older.
Is HIIT safe?
Yes, even for a person with a BMI in the obese range. If you have (or think you may have) a medical or orthopedic condition, explain HIIT to your physician to make sure it’s not contraindicated.
It’s unlikely that your doctor will warn you not do to HIIT on a stationary bike. I once had a client with peripheral vascular disease who performed HIIT on a bike.
Besides torching off fat, what are other HIIT benefits?
HIIT makes time go faster, offers an inviting change from the same ‘ol steady-state, improves sports performance, bumps up release of growth hormone and testosterone, tones and tightens, encourages lean tissue growth, and saves an abundance of time.
What is the definition of “sprint,” as applied to HIIT?
This doesn’t mean take off like a bullet.
“Sprint” means your very best effort, your fastest movement, your giving-it-all-you’ve-got…even if it’s just 5 mph.
At the end of the interval, you should be drained.
Is it okay to do HIIT and weights on the same day?
No. If you do HIIT first, you’ll be too sapped to attack the weights.
If you do weights first, your HIIT won’t really be HIIT.
You’ll be functioning at sub-intense capacity. Do HIIT on separate days.
Will HIIT make me a faster runner?
Of course, if your HIIT sessions involve your fastest sprints.
Can HIIT improve my endurance?
Yes. Eight walking or jogging cycles on an inclined treadmill will carry over to an outdoor hike. Eight running cycles will improve your steady-state jogging.

Shutterstock/Phase4Studios
How many cycles should I do?
Ideally do eight, and if you can do more, go for it.
If you can only get through four or six due to lack of conditioning or lack of time, that works too, but make at least eight a habit as much as possible.
Is it okay to do some steady-state after HIIT?
Yes. For example, steady-state walking on an incline or using the revolving staircase, following HIIT, will contribute to fitness needed for long challenging hikes.
It’s also okay to do steady-state sessions (under 20 minutes) before HIIT, as an extended warm-up.
What about work intervals under 15 seconds?
If you can run on a 15 percent treadmill incline at 10 mph for only 10 seconds before having to slow down to a 2 mph recovery walk, then this qualifies as an effective work interval. (Same with outdoor hills or steps)

Shutterstock/DedovStock
A person’s absolute fastest run (relative to an incline) may not be what he or she can do for a 30-second work interval.
For instance, a particular individual needs to jog only 7 mph on a 15 percent incline, to reach complete exhaustion after 30 seconds.
However, what can he or she do, for only 10 seconds at the same incline, before total exhaustion? Perhaps this individual can handle a speed of 12 mph.
Another example is a person who can sustain a 12 mph run at zero incline for barely 30 seconds, yet is actually able to run 15 mph for 10 seconds on the zero incline (some treadmills go up to 15 mph).
Running your absolute fastest, given the medium, will produce superior results, even if you conk out after 10 seconds.
Can walking be done as HIIT?

Cancer.gov
Yes. If you’re fit, your work intervals will require steep hills to bring on exhaustion within 30 seconds.
You can increase intensity also with weighted vests.
If you’re out of shape, you may need only slight inclines or even no inclines, depending on your condition.
Can I be too out of shape to do HIIT?
No. You can be too out-of-shape to run, but not too-out-of shape to put out your best effort.
A 300-pound smoker can pedal hard for 30 seconds on a stationary bike or elliptical machine.

Shutterstock/Creativa Images
If you’re in really poor shape, don’t necessarily limit your intervals to the bike or elliptical.
Do moderate to sub-intense intervals on a track (walking or very slow jogging).
Build up from there, over time. You can also include steady-state sessions as part of your conditioning program to prepare your body for eventual HIIT.
Should I get into HIIT shape by first doing intensity intervals lasting several minutes?
This is a good start, but not a requirement if you’d rather start off with the shorter intervals.
Longer intervals are also an option for the very fit; throwing in a 5-minute intensity interval during a HIIT session is perfectly fine.
How many times a week should I do HIIT?
Two times, though three is doable.
The third session can actually be sub-intense, longer intervals.
Will HIIT bulk up my legs?
A competitive sprinter may have “big” legs, but competitive sprinters also train nearly every day, many hours a week, including with heavy barbell squats.
A couple 30-minute sessions per week on a treadmill or staircase will not duplicate the legs of a sprint competitor who can blitz 100 meters in 10.8 seconds.
Can HIIT be done punching a heavy bag?
Yes. If you have an injured leg/foot, then throw your meanest punches at a bag.

Shutterstock/Dmitry Kalinovsky
But first make sure you learn how to safely throw a skull-shattering blow (hooks, crosses, uppercuts), before going all-out on a heavy bag.
If your legs are fine, each punch can be quickly followed by a kicking technique for extra intensity.
Can HIIT be applied to weightlifting?
Most certainly. Weightlifting routines, done to absolute failure, with rests up to 1-3 minutes (some schools of thought say briefer rests), are a form of HIIT.
Each set is a work interval. Or, stationary scissor lunges, following completion of an 8-12-rep max of leg extensions, would be a HIIT superset.
Squat-jumps for 30 seconds can be a work interval. Be creative!
Hopefully all of your questions about high intensity interval training have been answered in this post!
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: ©Lorra Garrick

What Causes Your Feet to Go Numb when Running ?

A leading neurologist explains about numb feet and running.
Ever get numb feet while running? Numb feet can be caused by a variety of factors, including neurological problems and cardiovascular problems. But what if you get only numb feet, and only while running?
First off, make sure your shoes properly fit. Tight shoes can cause feet to feel numb while running. Are your shoes new?
Or maybe you haven’t worn them in a while? Wearing extra thick socks lately?
Shoes may not feel tight, but constriction can be intensified while running, thereby creating numb feet.
“When you are running, your electrolytes (such as calcium) may be abnormally low (this is why people drink sports beverages with supplemental electrolytes), and this can cause tingling,” says Daniel Kantor, MD, director of the Neurology Residency Program, Florida Atlantic University.
“This can be relieved by making sure you are well-hydrated with sports drinks (you don’t want to dilute the electrolytes with water alone).
“Some people may have an underlying cause for their tingling, and heating up your nerves may bring out the symptom of tingling (this is rare if you are healthy enough to be running).”
The best way to prevent numb feet while running, says Dr. Kantor, is to simply stay well-hydrated: before, during and after the run.

Freepik.com
If despite making the above changes, you are still getting numb feet during running, consider trying a brand new pair of shoes, even if the ones you’ve been using seem to fit perfectly.
Maybe it’s time to purchase a new, and better, pair of running shoes; this may stop the numb sensations in your feet. An arch support may also help solve the problem.
Another thing that might cause numb feet while running is shoelaces tied too tight, or the Velcro straps being too tight.
And what about all that pounding your feet endure on hard pavement? This, too, can cause numb feet during your runs, especially if there are stones on the path.
Certainly you’ve heard of carpal tunnel syndrome. Ever hear of tarsal tunnel syndrome?
This is the “carpal tunnel syndrome” of the foot, in which the tibial nerve that runs through the inside of the ankle becomes compressed.
TTS has a variety of possible causes (nothing serious), so it’s best to consult with a physician.
Treatment may involve a custom-made shoe insert, rest and a cortisone injection. It these fail to alleviate the numbness in your feet while running, surgical release may be the answer, though often, nonsurgical treatment works.
Dr. Kantor adds, “Medications may also cause tingling and if you are on any, you probably want to talk to your doctor and ask if it may be contributing to your tingling.”
If numb feet while running continues despite making adjustments, then see your doctor to rule out any possible medical causes.
Dr. Kantor is also President Emeritus, Florida Society of Neurology.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/ zoff
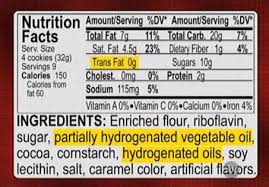
Easy Way to Tell if Food Has Trans Fats; Don’t Trust Labels
![]()
Don’t always believe nutrition labels that say “Zero Trans Fat,” but there is an easy way to tell if food contains this toxic substance. (more…)

How to Lose More Fat if You’re Not Overweight: Exercise Guide

Not overweight, but need to lose fat?
Do you feel “skinny fat” and want to replace some of that mush with lean firm muscle?


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}