

How a Panic Attack Feels When It Starts in a Night Dream

The panic attack began in a dream that I was having while asleep.
It was my first panic attack, and it began while, in the dream, I was outside on a hill with my brother. (more…)

Is a Fast Growing New Mole Always a Melanoma ?

Relax, do not panic if you discover what appears to be a rapidly growing mole on your face, leg, stomach, arm or any other area of your skin. (more…)

What to Do if You’re Still Getting New Moles in Your 40’s ?

Are you noticing a new mole here and there even though you’re now in your 40s?
This can be alarming to anyone who’s read that new moles after age 40 are cause for concern. (more…)
Can Melanoma Make a Mole Itch Before the Appearance Changes?

Bad news: Melanoma can make a mole itch even though the mole still looks normal and unchanged.
The itching can come before the mole starts looking different. (more…)

Benign Causes of Itching Moles Other than Melanoma

There’s a surprising number of benign reasons for a mole to begin itching.
Though melanoma indeed can cause a mole to be itchy, this symptom often has a cause other than cancer. (more…)
Can Melanoma Make a Mole Suddenly Get Bigger and Turn Red ?

You’re absolutely sure that a mole that you’ve always had has suddenly gotten bigger and also turned reddish in a matter of a day or two.
Melanoma or what can this be? (more…)
Death Risk from Normal Weight but Fat Belly vs. Fat All Over

Which is unhealthier and more likely to kill you: having a normal BMI but most of your fat in your middle or being obese evenly all over? (more…)
Pancreatic Cancer Risk Increases with Obesity & High BMI

If you’re obese, you have yet another health hazard to worry about: pancreatic cancer, especially if your body mass index exceeds 35.
Thirty and over is considered obese, and people with a BMI of over 35 have a greater risk of having a malignancy that has spread to the lymph nodes, plus a lower rate of survival, and a higher rate of recurrence after surgery for pancreatic cancer.
A study involved 285 pancreatic cancer patients who underwent surgery involving the pancreas, to treat their disease, between 1999 and 2006. Data was collected regarding the surgery, BMIs and outcomes.
The study was conducted by The University of Texas M. D. Anderson Cancer Center, Houston.
The study points out that in many obesity related conditions and cancers, a higher prevalence of pancreatic cancer was reported in many epidemiologic and cohort studies that focused on obese adults.
There’s more: Obesity was found to be linked to reduced survival in those with pancreatic cancer.
Seventy-five percent of the patients, who had a BMI of over 35, ended up dying, as of the time of the last follow-up, compared to 52 percent of the patients who had a BMI of 35 or less.
The heavier patients had lower estimated survival rates and disease-free rates. In the obese patients with a BMI of over 35, 95 percent had recurrence of their pancreatic cancer.
In the patients with a body mass index of 35 or lower, 61 percent had a recurrence.
This is not the only study to show an association between obesity and pancreatic cancer outcomes. Previous studies have shown similar results.
Thus far, the dynamics behind this association have not been discovered, and more research is needed.
Struggling with Obesity?

Tarso Meneghel, CreativeCommons
If you’re struggling with obesity, then make exercise a priority. If you’re already exercising, then make sure it includes cardio and strength training. Don’t just do cardio.
Both women and men need to work out with resistance, and not just tiny little dumbbells.
Many plus-size women avoid lifting weights because they think this will make them bigger. Wrong.
Lifting weights will force the body to burn fat for sustenance of new lean tissue gained from the exercise.
You will drop dress sizes and along the way, lower your risk of pancreatic cancer by becoming less obese.
Guidelines for Obese People Who Are New to Strength Training

Shutterstock/Reshetnikov_art
First off, remind yourself that body positivity includes doing what it takes to reduce the risk of obesity related cancers such as pancreatic.
Next, develop good form before you push for heavier resistance. If you’re not sure about the form of a particular exercise, it’s smarter to ask a personal trainer than to copy the next person you see doing the same exercise, since that person may be doing it with poor form.
Third, do not be self-conscious about walking into a gym. Everyone there has goals. Lowering the risk of pancreatic and other cancers should trump any feelings of self-consciousness.
Fourth, each set should be about eight to 12 or so repetitions. And each set should be challenging. Do not merely go through the motions.
If you’re not losing much weight despite faitihfully controlling your diet, you’re not working out hard enough. Up the ante. Push yourself without sacrificing good form.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/ Lyashenko Egor
Source: sciencedaily.com/releases/2009/03/090316173315.htm
Protein vs. Carbohydrate Drink After Cardio Exercise

Is a protein drink actually better than a carbohydrate drink after doing cardio exercise?
A study has an interesting conclusion. (more…)

Best Exercise for Chronic Heart Failure Patients

There are several types of exercise for chronic heart failure patients that research shows are very beneficial.
If you have heart failure, you will benefit more from exercise than from a sedentary life.
The first kind of exercise to consider is tai chi.
For patients with chronic heart failure, this form of exercise has been shown to improve their quality of life, as well as mood, plus self-sufficiency when it comes to exercise.
Unfortunately, up through to the late 1980s, those with chronic heart failure were instructed to avoid even light exercise — as they were deemed too frail for physical activity.
Exercises Other than Tai Chi that Are Best for Chronic Heart Failure
“In patients who actually have heart failure, ‘exercise’ means moderate levels of low-resistance aerobic activity such as walking, riding a bicycle or swimming at a comfortable pace,” says Roger Mills, MD, cardiologist and former professor of medicine, University of Florida, and author of “240 Beats per Minute. Life with an Unruly Heart.”
Want to try tai chi first?
A report on this form of exercise’s benefits to heart failure patients appears in the Archives of Internal Medicine (April 25, 2011).
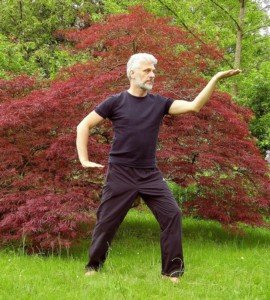
A tai chi pose
At the end of the study, the tai chi group and the no-exercise group were tested for peak oxygen uptake for a six-minute walk, and there was no difference.
This is not surprising because tai chi is not considered a “cardio” exercise. But keep reading.
There WAS a difference as far as improvement in quality of life in the tai chi group.
Not only that, but the tai chi group experienced increased confidence as far as performing some exercise-related activities.
Tai chi can thus be a stepping stone to more aerobic-type activities like swimming laps, bicycling or walking.
Dr. Mills explains, “A study of over 2,000 heart failure patients published in 2009 showed that structured exercise was safe and helped patients feel significantly better.”
For people with chronic heart failure, tai chi sounds like an ideal exercise, especially since there is no impact or sudden movements.
Check with your local recreation center to see if it offers tai chi classes.
However, to begin an exercise program, you need not take up tai chi.
Exercise for heart failure patients can come in all shapes and forms, including strength training.
Be sure to speak first to your doctor about exercise guidelines for your medical condition and any others that co-occur with the heart failure.

Dr. Mills is the former medical director of the heart failure and heart transplant service at the University of Florida, was a staff cardiologist at The Cleveland Clinic and has authored over 100 peer-reviewed publications.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}