
Can Chronic Subdural Hematoma Be Fatal if Untreated?
Is it possible for a chronic subdural hematoma to be fatal, being that the bleeding in the brain is slow?
Chronic subdural hematoma, unlike the acute (rapid bleeding) version, gives the patient plenty of time to get to the emergency room for treatment.
Chronic Subdural Hematoma Causes Slow Motion Brain Bleed
Unless the patient lives in the jungle or in a poorly developed nation with rudimentary medical facilities, he or she will see a doctor when the symptoms of chronic subdural hematoma begin developing.
Maybe not right away, but eventually. The symptoms of chronic subdural hematoma may be so slow-developing and/or seemingly innocuous, that the patient might end up choosing to make an appointment with his primary care physician, rather than get to the ER pronto.
My mother had two bouts of chronic subdural hematoma (the second was a recurrence of the first, and the second-time symptoms started out subtlety and gradually, whereas the first-time symptoms started out with a bang).
Because symptoms of chronic subdural hematoma can mimic that of a stroke, or interfere with daily living (e.g., a horrendous and persistent headache), the patient typically won’t waste too much time getting to a doctor…
Unless he resides in a developing nation with no adequate medical care, or lives alone and has pre-existing depression or other mental illness that keeps him in bed, or lacking insight, as the symptoms of chronic subdural hematoma worsen.
“A small cSDH with no or minimal brain compression could be observed expectantly with serial CT scans,” says Kangmin Daniel Lee, MD, a neurosurgeon with New Jersey Brain and Spine. (He was not my mother’s surgeon.)
This happened with my mother who had two chronic subdural hematomas on her first CT scan, but only the bigger of them (the one that eventually recurred) was surgically drained.
The other one was only four millimeters and was only observed.
Dr. Lee continues, “It would be important to get ‘treatment’ in the form of adequate blood pressure monitoring and modulation,” regarding cSDH’s with no or minimal brain compression.
“Evaluation of blood work to diagnose coagulation disorders is also important.
“So there are a number of other treatments besides surgery that are necessary for an adequate evaluation of someone with a chronic subdural hematoma.
“In the situation where all of these other factors are monitored and controlled, a patient with a small chronic subdural hematoma could easily be observed and monitored without surgical intervention.”
The 4-mm chronic subdural hematoma in my mother resolved without treatment.
Dr. Lee says, “If no rebleeds occur and the SDH does not grow in size, then the SDH would likely eventually get reabsorbed.
Occasionally the SDH may just remain stable in size indefinitely, and if the patient has minimal or no symptoms, then no intervention would be indicated.”
My mother’s first set of symptoms were not minimal and could not be ignored. They started out with a headache of crippling proportion, along with profound weakness in her legs. Who can let something like this go untreated?
Can You Ever Die from a Chronic Subdural Hematoma?
Dr. Lee explains, “Chronic subdural hematoma can definitely be fatal, if reabsorption of the hematoma does not occur then, but in general patients do seek medical care prior to getting to this point.”
The day of my mother’s first occurrence, I took her to the ER. The recurrence, however, came on gradually, with its first symptom masquerading as a post-surgical daily headache that we thought would eventually stop. But it got worse.
And then came the accidentally dropped items that, initially, masqueraded as lack of attention.
But when my mother couldn’t place her left index finger to her nose while her eyes were closed, and when she struggled to pick a straw up with her left hand, I knew that the chronic subdural hematoma was recurring.
Dr. Lee says, “There is very little data regarding mortality of untreated chronic subdural hematoma.
“This kind of data would be generally difficult to collect, but mortality from chronic subdural hematoma after surgical treatment is low – about 13 percent.”

Dr. Lee focuses on minimally invasive techniques to treat traumatic and degenerative diseases of the spine and brain tumors. He’s been invited to speak at the regional and national levels on his research areas.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Does Vomiting After Coronary Bypass Mean Something Serious?

If a person vomits after coronary bypass surgery (CABG), is this significant?
One must also consider how long after the coronary bypass surgery that the patient began vomiting.
Has the vomiting been ongoing since immediately following the CABG?
Or did the vomiting start up several days, or a week or so, after the coronary bypass surgery?
“Vomiting is poorly understood since it not only is caused by direct irritants to the stomach, but also by certain smells, tastes, sights, and even by motion,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
“After CABG, vomiting is usually a sign of poor gastric (stomach) motility.
“This is more prevalent in diabetics who are notorious for having poor gastric emptying.”
Diabetes is a major risk factor for coronary artery disease. But many coronary bypass patients are not diabetic.
Dr. Fiocco continues, “Other causes include medication irritating the stomach and severe constipation.
“For patients in the hospital, you may be faced with three or four morning medications plus pain medication before being served breakfast.
“Insist on something to eat first, or nausea and possibly vomiting will be the result.
“No matter the cause, vomiting after CABG is not common and usually self-limiting.”
My mother had some bouts of vomiting after her quintuple bypass surgery.
It began in the hospital after she was moved to the cardiac recovery wing, and it was soon realized by staff that the vomiting was associated with a vaso-vagal response (orthostatic hypotension), which she began experiencing nine days after her coronary bypass surgery.
The orthostatic hypotension has resolved, but to this day, it has not been determined what the cause was.
The three suspects are:
1) Impaired vascular tone from the coronary bypass surgery,
2) Pacemaker syndrome (the first orthostatic episode occurred the morning after my mother had a pacemaker implanted … nine days after the CABG), or
3) Side effect from the anti-arrhythmic drug amiodarone (within a day and a half of my mother stopping this drug, the orthostatic hypotension began decreasing until it disappeared).
My mother had occasional miscellaneous bouts of vomiting in the weeks following the coronary bypass surgery, that were not related to orthostatic hypotension.
Most of this vomiting occurred while she was struggling with constipation on the toilet (at home).
Another instance of at-home vomiting apparently was related to the emotional turmoil caused by the coronary bypass surgery.
Immediately following coronary bypass surgery, a patient may vomit as a result of the general anesthesia.

Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com/ stefamerpik

What Does Abdominal Pain After Coronary Bypass Mean?

Abdominal pain after coronary bypass surgery can be mild or considerable, and make the patient think something is wrong.
Pain can be frightening, especially after coronary bypass surgery (also known as CABG).
“This is an extremely common problem which in the vast majority of cases is benign and self-limiting,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
So then, what are some causes of post-op pain with coronary bypass surgery?
Dr. Fiocco continues: “The most common causes are pain from the drains which exit the body in the upper abdomen, causing some pain and occasional muscle spasm and constipation.
“The discomfort from the drains subsides when the drains are removed 48 hours after surgery.
“Constipation is usually resolved before discharge, but may linger depending on the patient’s level of activity and their use of narcotic pain medicine.
“More narcotics, less activity, means more constipation. These common causes of abdominal pain rarely last for more than a few days and the pain is usually quite mild.”
But if the pain is more than mild, say, approaching a 7 or 8 on the hospital’s pain scale, where a rating of 10 means the worst pain you can imagine, this may reflect:
Simply the patient’s general physical condition (is the patient older, out of shape?)
The patient’s natural tolerance for pain
And if other issues are going on with the patient, such as clinical depression (primary or secondary), which can amplify perception of pain, and abdominal pain from coronary bypass surgery is no exception to this amplification.
There can also be more serious, though much rarer, causes of abdominal pain following CABG.
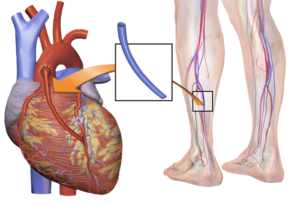
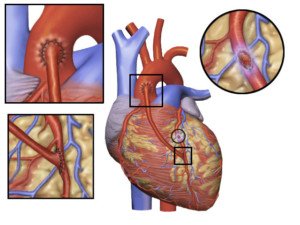
CABG. Source: Blausen Medical Communications, Inc.
Dr. Fiocco explains, “More concerning and fortunately very rare is pain from pancreatitis, bowel distention, and peptic ulcer disease. These disorders require longer stays in the hospital and close observation.”
What would be the course of treatment in the event of these complications following CABG?
“CT scans, upper and/or lower endoscopy, and frequent blood tests are needed to diagnose and treat these problems,” says Dr. Fiocco.
“They are rarely life threatening, but may be quite debilitating for several weeks.”
Can abdominal pain following coronary bypass surgery ever mean a life threatening situation?
“The most unusual cause of abdominal pain, but the most dangerous, is ischemic bowel, or loss of blood supply to the bowel,” says Dr. Fiocco.
“This occurs secondary to a clot or piece of plaque flowing downstream to the arteries of the intestine, similar to how a stroke affects the brain.
“This may require emergency surgery in its most severe form.
“The most important message for patients is that abdominal pain may occur after CABG, but is almost always self-limiting, mild and benign.”
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/antoniodiaz

Chest Pain: How Long After Bypass Surgery Is It Normal?

Still having chest pain even after your coronary bypass surgery?
It’s understandable for a person, fresh from coronary bypass surgery, or even several weeks out, to think he’s having a heart attack or something wrong with his heart, when he has chest pain.
“Chest wall pain after cardiac surgery may normally last 3-6 weeks, but may last as long as 12 weeks on rare occasions,” says Dr. Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
Think of it this way:
A surgeon just cut open your chest. This involves “cracking” open the sternum and using a crank-like device to pry it apart to expose the sac that surrounds the heart.

Source: Shutterstock/mountainpix
After the bypass surgery, the surgeon reattaches the sternum, which is bone, using wire. Of course you will have chest pain after bypass surgery!
Dr. Fiocco explains, “This pain has a different quality from angina and most patients know the difference without question.
“Post-op pain is also related to movement, coughing, and normally can be reproduced with palpation of the chest wall, none of which occur with ischemic pain (angina).”
Palpation means feeling and pressing with your fingers against your chest.
“It’s extremely rare to have angina following CABG (coronary artery bypass grafting), and differentiating between angina and post-op pain should be simple with just a physical exam,” continues Dr. Fiocco.
Think of coronary bypass surgery as new plumbing for your heart.
The new plumbing (veins harvested from your leg and/or arm) is free of the clogging and blockage that necessitated the operation in the first place.
As a result, oxygenated blood easily flows through these vessels, supplying your heart with oxygen.
Angina is chest pain that results from restricted blood (oxygen) flow to the heart.
Thus, the discomfort you feel following coronary bypass surgery, like Dr. Fiocco says, is typically related to motion and coughing. Coughing creates motion of the chest wall, which was just cut open.
Movement such as shifting positions in bed or even taking a deep breath, causes the chest cavity to expand or lift.
It was just operated on; chest pain is to be expected.
The chest pain may seemingly come and go for no apparent reason, but even subtle motion can bring it on.
Don’t let chest pain, that follows coronary bypass surgery, alarm you, even if you’re experiencing it weeks after.
However, it’s important to note concerning discomfort to your surgeon and cardiologist.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Photographee.eu

Why Do I Have NO Appetite Since My Heart Bypass Surgery?

Of course you’ll have no appetite in the days right after coronary bypass surgery — but what if the appetite suppression persists?
Your appetite a few weeks after coronary bypass surgery may still be somewhat suppressed, though some patients will be eating quite heartily even one week out from CABG.
This depends on their preoperation eating habits, and whether or not they decide to change their eating habits for the better, post-operatively.
“Change in the taste of food after surgery is not unusual immediately after surgery, and mostly resolves with time,” begins Michael Fiocco, Chief of Open Heart Surgery at Union Memorial Hospital in Baltimore, Maryland, one of the nation’s top 50 heart hospitals.
But there are numerous other reasons for losing one’s appetite after coronary bypass surgery.
Ten weeks after my mother had quintuple bypass surgery, she still had much appetite suppression.
“I have to force myself to eat,” she had said. From the get-go, she had no appetite in ICU, but ate a little more once she was moved to recovery.
Once she was home, she hardly ate, though there had been improvement as far as variety of food.
My mother was never a big eater, but the difference in her appetite post-surgery, and her appetite prior, was enough to have caused her weight to drop from 141/140 to 128, though sometimes it was 130.
Initially she claimed that all food, except eggs and potato chips, tasted like cardboard.
Even when Taste Is Normal, Appetite May Still Be Suppressed Weeks after CABG
CABG. Credit: BruceBlaus
Over time she began re-expanding the menu to include just about all foods — but in small amounts.
Eventually she was eating every type of food she normally ever did. Her taste had returned, but the appetite still remained suppressed for some time after that.
She had supposed that maybe her stomach had shrunk, and that it would take time to regain her appetite.
“Loss of appetite after surgery is well-described and poorly understood,” says Dr. Fiocco.
“It can be caused by persistent pain, constipation and depression, as well as many poorly understood factors.”
When Eating Less Causes Weight Loss
You might be thinking that weight loss from appetite suppression is a good thing for an overweight coronary bypass patient.
But what if the patient wasn’t overweight in the first place?
My mother is a senior citizen, had not been exercising and had not been eating much following the bypass surgery. This translates to loss of valuable muscle tissue.
A senior citizen cannot afford to lose muscle.
When they do, they become weaker; or, to put it another way, they are not as strong as they could be.
My mother is about 5-4, and when she was 128 pounds, she weighed as much as her 5-6 daughter-in-law. But there’s a huge difference in their body compositions.
The younger woman had been working out to the Insanity DVD series, and plus, she had an excellent appetite and hence, ate full meals.
Though she’s very lean in appearance, she has a healthy amount of muscle.
My mother has always had excess abdominal fat, and following the coronary bypass, had visible loss of muscle in her legs and arms.
My sister-in-law has tight, fit-looking legs and arms (though I think she can add more muscle), and hardly any fat in her abdominal area. In short, two entirely different body compositions were going on.
So what was the cause of my mother’s loss of appetite since her coronary bypass surgery? I don’t know, and neither did her doctors.
Solutions to Appetite Loss After CABG
Dr. Fiocco explains, “Patients with persistent problems will usually find relief through changing or eliminating medications.
“The suggested solutions are as numerous as the causes, including treating the above ailments, using supplements like Boost, eating small non-fatty meals, eating with other people, eating several smaller meals each day, and even stimulating your appetite with small amounts of dark chocolate.”
If you or someone you know is experiencing appetite loss following CABG, it will likely return, as did my mother’s.
Dr. Fiocco specializes in treating artery disease, valvular disease and aortic aneurysm. His heart care expertise has earned him recognition by Baltimore Magazine as a Top Doctor in 2010, 2011, 2013, 2016 and 2017.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Photographee.eu

Best ER Test for Chest Pain; Rules Out Severe Heart Disease

Chest pain is frightening and if you’re in the ER, there’s a test you’d better request.
A test that research shows is very reliable for detecting a heart problem.
The best test, shown to be effective and safe, is the CTA (computed tomographic angiography), says a long-term study.
If you come to the ER with chest pain, you should have the CT angiogram done, says University of Pennsylvania School of Medicine research.
But ER doctors don’t always order this test for patients coming in with chest pain – certainly not in the case of my mother, who I took to the ER because of her chest pain. The CT angiogram was not ordered!
Troponin tests were, and this is standard for patients coming to the ER with chest pain. Eight million people go to ERs every year in the U.S. with chest pain.
However, 5-15 percent are actually having heart attacks or some other cardiac issue.
Over half are admitted to the hospital for observation and further testing (such as my mother after her second ER visit two days later; she had not had a heart attack).
Her next test was an echocardiogram to see if she was suitable for a treadmill stress test.
The echocardiogram was “abnormal,” so the next step was the invasive and risky catheter angiogram … which showed dangerously blocked coronary arteries; two hours later she was in the OR undergoing quintuple bypass surgery.
The CT angiogram is much safer in that it doesn’t carry the risks of blood clots, infection, stroke and cardiac arrest, like the catheter angiogram does, though these complications are rare.
The CT angiogram offers a faster and less costly way to determine which ER patients have had a recent cardiac problem.
“The ability to rapidly determine that there is nothing seriously wrong allows us to provide reassurance to the patient and to help reduce crowding in the emergency department,” explains Judd Hollander, MD, the study’s lead author, professor and clinical research director, UPSM’s department of emergency medicine.
Of the 481 patients in this study who had negative CT angiograms, meaning, no evidence of seriously blocked coronary arteries, none of these patients had heart attacks in the year following their exam, and none had bypass surgery or even stenting.
How much does an ER CT angiogram cost?
About $1,500. But admit a patient to the hospital for telemetry monitoring and stress tests?
You’re looking at over $4,000.
This often happens to patients who turn out not to have any serious coronary blockage, and could have been avoided with the quicker, much cheaper CT angiogram.
“The evidence now clearly shows that when used in appropriate patients in the ED, we can safely and rapidly reduce hospital admission and save money,” explains Dr. Hollander.
Perhaps a “national coverage decision” is just around the corner that will “facilitate coronary CTA in the emergency department,” adds Dr. Hollander.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ Photographee.eu
Source: sciencedaily.com/releases/2009/05/090515104219htm

Low Thyroid May Be Causing Your Clinical Depression
One cause of depression can be a thyroid problem: more specifically, an underactive thyroid, also known as hypothyroidism.
Yes, you read that right: hypothyroidism can lead to clinical depression.
The disease of hypothyroidism, when the thyroid is underactive, is commonly associated with weight gain or difficulty losing extra weight.
This component of low thyroid gets so much attention that the component of depression gets buried.
But clinical depression is one of numerous possible outcomes of a malfunctioning thyroid.
“When the body doesn’t create enough triiodothyronine (T3) or thyroxin (T4), it causes your thyroid stimulating hormone (TSH) to rise,” says Walter Gaman, MD, FABFM, board certified in family medicine and the author of several award-winning books including “Age to Perfection: How to Thrive to 100, Happy, Healthy, and Wise.”
“The body then experiences symptoms of depression, such as fatigue, loss of ambition, trouble concentrating and generalized feelings of sadness.
“Many doctors may immediately test your thyroid when you complain of these symptoms, while others will assume it is clinical depression without a primary source. This is why some patients do not respond to antidepressants.
“The flipside of this is that people with hypothyroidism may also develop clinical depression that has actually altered the brain chemistry.”
If you have symptoms of depression or know someone who is showing signs of depression, don’t blow off the possibility that an underactive thyroid can be the underlying cause.
A blood test will determine if the thyroid is working properly.
This doesn’t mean that most people with feelings of hopelessness and despair, lethargy, fatigue and loss of appetite have hypothyroidism.
But every person with depression should have a complete physical workup to see if thyroid hormone levels are normal.
Besides depression, classic symptoms of hypothyroidism include:
- Often feeling cold even though the temperature is normal and everyone else in the room feels fine
- Hair loss that doesn’t seem in alignment with male pattern baldness or aging
- Hoarse voice
- Fatigue and lethargy
- Excessive sleepiness and wanting to sleep all the time
- Moderate weight gain (though not all people with hypothyroidism will gain weight, especially if depression is killing their appetite
- Constipation; and tingling in the hands and fingers.
A patient will not necessarily have every symptom listed here, and may only have a few at the time of diagnosis.
It’s interesting to note that sometimes, depression is the first clue that a person’s thyroid is not producing enough hormones.
“The thyroid medication alone may not be enough to reverse the symptoms, and an antidepressant may be necessary in the short run,” says Dr. Gaman.

Dr. Gaman is with Executive Medicine of Texas and is with the Staying Young Radio Show 2.0 podcast.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Steroid Psychosis from Medrol DosePak: Yes, It Happens

Medrol can cause very nasty side effects like psychosis — called steroid psychosis.
And it’s not uncommon for ER physicians to see this.
My mother’s neurosurgeon said “one percent,” and then “half of one percent,” while in the surgery prep area where mother was being prepped for evacuation of a chronic subdural hematoma.
This was a recurrence of the chronic subdural hematoma, and the neurosurgeon had prescribed the Medrol Dosepak.
He never mentioned the possibility of mental side effects, though the insert mentioned them. He did mention, however, that constipation could result.
Several hours after taking her first Medrol tablets, my mother became a raving, delirious stranger, highly agitated, and had lost all rational thought processes.
My father asked if this could be a side effect of the steroid, and I said, “No, steroids don’t cause these kinds of side effects.”
I thought that the ranting, bouts of crying, complaints of being unable to breathe, and general delirium, were from a recurrence of the chronic subdural hematoma, with some panic attack mixed in (my mother has a history of panic attacks).
After all, she had already been experiencing two other symptoms that were obviously from a recurrence (and later confirmed via CAT scan) of the chronic subdural hematoma: searing headaches that increased in frequency, and deterioration of fine motor control in her left hand.
So my mind, then, was locked on the conclusion that the rapid-onset madness was yet another symptom of a recurring chronic subdural hematoma.
In the ER, the doctor suspected steroid psychosis from the Medrol, but couldn’t rule out a recurrence of the chronic subdural hematoma until the CAT scan results were in.
The CAT scan showed nothing that could explain such behavior, and the doctor diagnosed her with a bad reaction to the Medrol, known as steroid psychosis.
Steroid psychosis is not the same as “roid rage.”
There are two kinds of steroids: anabolic and catabolic.
Anabolic steroids are what athletes use, to build muscle (anabolism). Corticosteroid drugs, used to control or bring down inflammation, are catabolic (promote muscle breakdown), and often cause fat gain.
The ER doctor said she sees steroid psychosis often, but also said it’s not common.
The neurosurgeon, of course, said that steroid psychosis occurs in one percent, and one-half of a percent, in patients.
Interestingly, my mother tolerates Cymbalta and Effexor beautifully, and antidepressants are notorious for causing a myriad of intolerable side effects, but for my mother, Medrol was a horrible drug.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Can Cymbalta’s Discontinuation Syndrome Be Prevented?

What a shame that the drug companies can’t make an antidepressant like Cymbalta that doesn’t have a discontinuation syndrome, but there’s hope if you want to get off this drug and similar ones.
Antidepressants like Cymbalta, Effexor and Paxil may very well have the worst discontinuation syndromes, even when these drugs are tapered off gradually.
The problem is magnified when people quit Cymbalta and other antidepressants cold turkey, or, they don’t taper off Cymbalta, etc., gradually enough.
I asked an expert if there was a way to prevent discontinuation syndrome from Cymbalta and similar antidepressants: Joe Wegmann, psychopharmacologist and licensed clinical social worker, author of Psychopharmacology: Straight Talk on Mental Health Medications.
“There really is no way to eliminate discontinuation syndrome with Cymbalta,” says Wegmann. “After 4-5 weeks of use, anywhere from 35 to 75 percent of Cymbalta users will experience withdrawal symptoms upon discontinuation.
“The withdrawal symptoms associated with this drug range from mild in some people to moderately severe in others.
“The length of the withdrawal process tends to be dose-dependent – that is, the higher the dose, the longer it takes the discontinuation symptoms to abate.”
A person who’s been on Cymbalta for a while may feel so good, that he or she might then start believing they don’t need the antidepressant any longer.
But the reason they’ve been feeling so normal and motivated is because Cymbalta has been working on their brain chemistry; go off it, and chances are, the symptoms of depression will return.
Depending on a person’s grade of depression, it may be best to keep using Cymbalta or similar antidepressants until an outright, one-dose-pill cure for depression is discovered.
Wegmann continues: “The onset and severity of the discontinuation syndrome with antidepressants is linked to their half-lives – the amount of time, on average that it takes for 50 percent of the antidepressant’s active ingredient to be eliminated from the body from peak plasma levels.
“The short-half life antidepressants – Paxil, Zoloft, Effexor, Cymbalta – tend to produce the worst discontinuation syndromes.
“Prozac however, because of its long half-life (seven days), tends to produce very little, if any, discontinuation symptoms at all.”
I’m an “anti-drug” person, in that I believe that rather than rely upon drugs, people should practice natural, holistic ways of living to be strong and feel uplifted; that pills and capsules are not the answer; that feeling depressed is part of being human.
However, depression can also render a person bedridden — and then what?
Or, if they’re out of bed, they are frequently crying, refuse to eat, and do little more than sit in a chair and stare into space, worry, have panic attacks, and frequently complain about physical pains.
You can’t get somebody like this to exercise, take a brisk walk on a mountain trail, attend cognitive behavioral therapy, or eat lots of natural foods when it’s a battle just to get them to take a few bites of toast — as with what had happened with my mother when she developed severe clinical depression.
In that case, antidepressant intervention is necessary, when all else has failed, and the depression will not go away on its own.
Cymbalta is recommended for depressed people whose illness also creates physical pain.
In some people, this drug works wonders, but doggone it, this drug, along with Effexor, Paxil and Zoloft, are cursed with discontinuation syndrome.
Wegmann explains: “Tapering is dependent on the milligram strengths in which an antidepressant is available. In my experience, regardless of the antidepressant, anyone should be able to discontinue without severe withdrawal symptoms over a period of three months.
“There is a tendency for people to commiserate on these blogs (about their horrible discontinuation syndrome experiences with Cymbalta, Effexor, etc.).
“Many are quitting cold turkey and not admitting it. Others are likely taking multiple medications, some of them psychotropics, which are affecting the discontinuation process.
“Unmentioned physical illnesses and substance abuse may also be contributors. Bottom line: Severe discontinuation syndrome is avoidable with slow, steady tapering.”
 Joseph Wegmannis a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
Joseph Wegmannis a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

What to Do if You Gained Weight from an Antidepressant

Antidepressant weight gain happens, but there are ways to fight back.
Here are solutions to weight gain from antidepressants.
There are two types of weight gain from antidepressants.
It’s the second type that can have many people up in arms; after all, an antidepressant is supposed to help you gain back a positive mood, not weight.
It’s no secret that antidepressants can cause certain individuals to put on weight.
Let’s look at the second type of weight gain from antidepressants first: putting on extra pounds that weren’t there prior to antidepressant use.
“There is evidence that serotonin activation leads to an increase in appetite,” says Joe Wegmann, psychopharmacologist and licensed clinical social worker, author of Psychopharmacology: Straight Talk on Mental Health Medications.
Serotonin is the neurotransmitter that helps regulate mood, of which deficient levels are associated with depression.
Antidepressants cause an increase in serotonin levels.
Wegmann continues: “There are 14 different serotonin receptor subtypes. The activation or inhibition of some of these serotonin receptors keeps the brain’s ‘satiety switch’ in the ‘off’ position.
“As such, some individuals using the serotonin antidepressants in particular aren’t able to recognize when they feel full while eating, and as such, don’t feel satiated, and continue to eat unnecessarily.”
And that explains why putting on weight can result from using antidepressants. The body fat gain can be offset by exercise.
It’s difficult or impossible to stick to exercise while being ruled by depression, but once an antidepressant subdues those feelings of apathy, lethargy, sadness or that bottomless-pit feeling, you can work towards committing to moderate to vigorous exercise (build up gradually to vigorous if you haven’t exercised in a long time).
Wegmann adds, “Paxil tends to produce the most weight gain among the SSRIs. Weight gain with the SSRIs and SNRIs tends not to exceed 10 pounds in most people.
“There are of course exceptions. Wellbutrin, since it has no serotonin effects, is essentially weight neutral. Some people even lose weight with Wellbutrin use over time.”
The other type of antidepressant weight gain involves putting back on the pounds that you lost due to suppressed appetite from depression/anxiety.
Says Wegmann, “Most people meeting criteria for clinical depression do experience weight loss, precipitated by psychomotor retardation (slowed mind, slowed body) amotivational syndrome, and anhedonia (an inability to experience pleasure).
“Eating is a pleasurable experience for us non-depressed folks, but for depressed individuals, the above mentioned symptoms inhibit appetite.
“So when placed on antidepressants, as the retardation, lack of motivation and inability to experience pleasure improves, eating becomes more pleasurable, appetite increases and weight gain (of the lost pounds) ensues as a result.
“In very severe depressions, significant weight loss may occur. So regaining this weight is essential to health.”
Joseph Wegmann is a licensed clinical pharmacist and clinical social worker with more than 30 years of experience in the field of psychopharmacology.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}