

Blood Clots (DVT): Q & A with MD about this Silent Assassin
Dr. Darren Klass answers questions about deep vein thrombosis, a potentially fatal type of blood clot that can strike anybody, any fitness level, any age.
Darren Klass, MD, is Clinical Instructor of Interventional Radiology at the University of British Columbia and the Vancouver Coastal Health Association.
In layman’s terms, what is DVT?
DVT is deep vein thrombosis; this term generally refers to the development of a clot in the deep veins in the legs and pelvis.
The deep veins in the legs run between muscle compartments and cannot be seen without medical imaging.
How is it caused?
DVT is caused by blood within moving veins clotting. The clot is cause by three factors:
- Slow flow in the vein
- Abnormal clotting factors in the blood which cause it to clot more than normal
- Damage to the lining of the vein
Are there ways to prevent?
There is no way of completely preventing blood clots without medication, which in itself has risks. Ways to decrease the risks are:
- Keep well-hydrated; dehydration thickens the blood.
- Avoid sitting in the same position for long periods of time (i.e., long plane flights).
- Avoid tight constricting clothing at the hip, which may squash the vein in the groin and slow flow.
How can I be on the lookout for a clot?
If one part of your leg (the calve, thigh or both) suddenly becomes swollen and painful, or suddenly veins which were not visible under your skin become more prominent, you should consult your family doctor.
What are the risks if it’s not caught?
DVT may cause little or no long term complications if treated early. If left untreated, the risks are the following:
- Piece of the clot may break off and travel to the lung causing a pulmonary embolism.
- The clot may extend into the main vein in the abdomen (termed the IVC) and stop the flow of blood from the pelvis and opposite leg, which may cause complications.
- If the clot involves the veins in the pelvis, this may require treatment in a hospital to break up the clot (thrombolysis performed by an interventional radiologist). The aim of the treatment is to clear as much clot from the veins as possible and allow healing of the vein.
If the vein is left untreated and the clot is absorbed by the body, the vein is often left scarred.
The scarring may damage valves in the vein, which can lead to a chronic swollen leg, which is difficult to treat and may cause significant limitation in everyday activity. This condition is called post-phlebitic syndrome.
What are the options for treatment of DVT?
DVT can be treated in the following ways:
Medication to thin the blood and decrease the risk of the clot extending.
However, the clot remains in the vein until the body reabsorbs it and the vein is often left scarred.
The clot can be removed by a minimally invasive procedure performed by an interventional radiologist.
The procedure involves using special medication and advanced equipment to break up the clot and remove it from the vein and restore flow immediately.
The procedure is done through a tiny hole made in the vein behind the knee and a very small cut in the skin about 3 mm in length.
 Dr. Klass specializes in interventional oncology, aortic intervention, PVD, venous disease and venous access. He has been inducted into The Leading Physicians of the World, published by the International Association of HealthCare Professionals.
Dr. Klass specializes in interventional oncology, aortic intervention, PVD, venous disease and venous access. He has been inducted into The Leading Physicians of the World, published by the International Association of HealthCare Professionals.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Cause of Heavy Bleeding after Missed Period

The cause of heavy bleeding in menstruation that follows missed periods is quite logical.
Many women wonder and are even worried about the cause of heavy flowing in a period after menstruation has been missed once or a few times.
“The cycle consists of estrogen stimulating the lining of the uterus (endometrium) and ‘building up’ the lining,” begins Dr. Marlan Schwartz, MD, FACOG, robotic surgeon with Lifeline Medical Associates.
“If this is not shed, and there are multiple reasons that could cause this, it will likely be kept being stimulated by more estrogen, thus causing the lining to be even thicker.
“If one then has a period or loss of this lining, as it has been made thicker (six or seven weeks of stimulation versus three weeks), there is more to shed.”
 Dr. Schwartz is the past Chairman of the Department of Obstetrics and Gynecology at Robert Wood Johnson University Hospital-Somerset.
Dr. Schwartz is the past Chairman of the Department of Obstetrics and Gynecology at Robert Wood Johnson University Hospital-Somerset.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Are There Reasons a Colonoscopy Can Miss Colon Cancer?

You know a colonoscopy can miss colon cancer, right? So find out exactly why, and what questions to ask your doctor.
Though a colonoscopy has saved the lives of many people by detecting precancerous polyps, it can also miss actual colon cancer.
“Endoscopy is not perfect and that’s tough fact to deal with as a gastroenterologist,” says Whitney Jones, MD, a national expert and frequent speaker on early-age onset colon cancer prevention, and Founder, Colon Cancer Prevention Project.
For average-risk people, colonoscopies should begin at age 45 — according to the U.S. Preventive Services Task Force — and be done every 10 years after.
“The 10 year interval as we all know is a negotiated time frame, not a date set in stone from God,” says Dr. Jones. “It’s the best estimate.”
The truth is, a colonoscopy can provide “incomplete protection,” adds Dr. Jones, which “usually lies with three factors.”
Three reasons a colonoscopy can miss colon cancer
#1. “Operator characteristics: Not all docs who do endoscopy do the procedure equally well,” says Dr. Jones.
“Many are benchmarking and working on continuous improvement, i.e., tracking fecal intubation rates, withdrawal times, adenoma [cancer] detection rates, of using split dose preps which better clean and prepare the right [sided] colon.
“These are questions any person having a colonoscopy should ask their physician.”
The second reason a colonoscopy can miss colon cancer is “anatomic considerations,” says Dr. Jones.
“It is impossible to see every square cm of the colon with any modality. There is a miss rate of up to 10% for 1cm adenomas, even by experts.”
Reason #3 for why a colonoscopy can miss colon cancer: “Biological issues: Right colon adenomas are much more likely to have an evolving pathology called serrated adenomas; these polyps evolve into cancer through a different pathway called hyper- methylation. They are not your mother’s colon polyps/cancers.
“They have several differences including a more flat nature, making them harder to identify, be obscured with mucus or stool, progress to cancer in a shorter time frame and be located obviously in the right colon, which is harder to reach.”
Dr. Jones advises high-risk people to request more frequent screening and to consider asking their doctor for a stool test between colonoscopies.
 Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Dr. Jones’ practice interests include prevention and treatment of colon cancers, pancreatic disease and biliary disease. He has authored numerous scientific articles, reviews and abstracts and presented at a variety of national and international scientific meetings. Colon Cancer Prevention Project
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/9nong
What if You Get a Pulmonary Embolism on a Plane?

Suppose a passenger on an airplane develops an apparent pulmonary embolism; what should, or CAN, you do?
A deep vein thrombosis can develop while a person is on an airplane.
What might be done for help if this DVT migrates and becomes a pulmonary embolism, and a doctor just happens to be on the plane—a doctor who has treated pulmonary emboli?
“You will not show signs of a pulmonary embolus on an airplane,” says Michael P. Zimring, MD, Director, Travel Medicine, LLC at Mercy Medical Center, Baltimore, Maryland..
“The PE usually breaks off from a clot starting in the lower extremities — and that takes a while to develop.
“You usually show signs of a pulmonary embolus after a significant time of first forming a clot in the leg. Sometimes it is fast, but not usually.”
In a hospital setting, the treatment for a pulmonary embolus is IV administration of a “clot busting” or thrombolytic drug.
Doctor on Airplane Suspects Passenger Has a Pulmonary Embolism
But what if a doctor on a plane suspected that a passenger had a PE (based on symptoms, risk factors), and that doctor just happened to have a clot busting drug and syringe in his medical kit?
These are fair questions for a layperson to wonder about.
Though thrombolytics carry the risk of dangerous internal bleeding as a side effect, it’s reasonable for a layperson to wonder about this if a passenger has an apparent pulmonary embolism and is 35,000 feet off the ground.
Diagnosing a Pulmonary Embolism
A pulmonary embolism cannot be confirmed based on just symptoms (sudden difficulty breathing, chest pain, coughing up blood) and risk factors for DVT (prolonged inertia in an airplane, obesity, smoker, among many others).
Back to that doctor on the plane. What if he also has a stethoscope and listens to the distressed airline passenger’s heart?
A pulmonary embolism can change the way the heartbeat sounds through a stethoscope.
Dr. Zimring explains, “A typical physician will not hear a strain of the right heart through a stethoscope, and no one will be able to detect a PE by physical means.
“No one would dare treat a pulmonary embolus by injecting a thrombolytic on a plane because there is no way he could be sure the patient has a PE.
“There are many factors to be taken in consideration before injecting a thrombolytic in the best hospital environment.
“In addition, the physician might not be covered under the Good Samaritan Laws if he did such a specialized procedure in an emergency situation.”
Prevention of Blood Clots Triggered by Air Travel
If you’re worried about developing a pulmonary embolism as a result of flying, take precautions:
Stay well-hydrated throughout the plane trip; exercise the calve muscles every 15 minutes during the flight; don’t be seated for more than an hour; and avoid alcohol.

Exercises during air travel
 Dr. Zimring has 40+ years of experience diagnosing and treating a host of medical conditions.
Dr. Zimring has 40+ years of experience diagnosing and treating a host of medical conditions.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Quick Easy Way to Tell if Red in Stools Is Beet Juice

Here’s how to tell within seconds if the “blood” you see in your bowel movements is actually undigested beet juice.
I juice beets all the time, and I experience “stool beeturia” as a result.
Perhaps the biggest telltale sign that the red in your poops is from the beet pigment betain, is that it has a glowing, neon-like quality.
Even veteran beet eaters can still wonder if the red in their stools is blood, especially if they’ve recently had a digestive problem.
This is the same glowing, neon-like quality you see when a glass fills with the juice of a fresh beet being juiced.
Pictures of glasses of beet juice on the Internet don’t do this pigment justice.

Shutterstock/bitt24
Most website images of beet juice in glasses seem to be beet juice blends.
Read the descriptions; almost always, there are other items juiced into the beverage, such as carrots, blueberries, apples, celery or some leafy green.
This suppresses that glowering, neon-like color. If you juice ONLY beets, you’ll be struck by the amazing crimson glare.
It’s beautiful and bright. This quality is retained in your stools when betain does not get absorbed.
Blood in the stools does not look like this.
Though blood in the stools may be fresh (and “bright red”), it lacks that glow, that neon-like feature, that distinct ruby-magenta or crimson-magenta color, whereas blood is simply a solid red.
There’s a difference between crimson-magenta and solid red.
The exact color of betain in BMs seems to be 80 percent crimson, 20 percent magenta, with neon. This hardly describes blood, fresh or old.
As a woman, I’ve seen blood in the toilet with (NOT in) my stools as a result of menstruation.
If blood is being discharged from my vagina at the same time I’m having a bowel movement, the blood will sometimes get “mixed” with the poops.
I know what this looks like all too well. And it cannot pass for betain. Quite simply, betain often just GLOWS.

Freepik.com
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/KarepaStock
How Many Burps per Minute from Anxiety? How to Stop?
Wait till you find out how many times per minute anxiety can make a person burp.
It’s no secret that anxiety can cause burping, but just how much?
“In extreme cases, belching can occur up to 20 times a minute,” says Dr. David Robbins, a gastroenterologist at the Manhattan Endoscopy Center, NY.
“But in these cases it’s usually release of air from the esophagus back up into the pharynx without ever getting down into the stomach.”
The sound of a belch occurs when air escapes from the esophagus into the pharynx, says Dr. Robbins.
But he adds, “The most common type of belching originates when swallowed air from the esophagus enters the stomach, only to be released when the valve at the bottom of the esophagus relaxes.”
He refers to the type of burping, in which the released air was never in the stomach (only in the esophagus) as “supragastric.”
Most patients who have this type of burping “suffer from some element of anxiety,” continues Dr. Robbins.
“Studies have shown that the symptoms increase along with increasing stress. It’s also been described with obsessive-compulsive disorder and various eating disorders.”
So how does one stop burping 20 times a minute?

Shutterstock/Aaron Amat
“Interestingly, many patients can ‘squelch the belch’ while speaking,” says Dr. Robbins.
“This is basically a sort of distraction maneuver. This type of belching never occurs during sleep, again pointing to an active anxiety component.”
If you find yourself burping many times in just one minute, talking incessantly to squelch it isn’t practical, for obvious reasons.
What else can you do, then, besides making efforts to manage stress?
“There are no established treatment regimens for excessive belching,” says Dr. Robbins.
However, he adds, “Extreme cases require the help of a cognitive behavioral psychologist or a psychiatrist. Speech therapy and biofeedback have shown some modest results, while drugs such as simethicone (or Gas-x) have not.”
When circumstances are normal, says Dr. Robbins, burping “actually occurs up to 30 times a day” and is a “normal physiologic phenomenon,” even though we all have known at least one individual who can emit loud belches seemingly at will.
 Dr. Robbins is board certified in both gastroenterology and internal medicine. He has been invited to speak internationally and has published and lectured widely.
Dr. Robbins is board certified in both gastroenterology and internal medicine. He has been invited to speak internationally and has published and lectured widely.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

How Many People in Their Mid 30s Get Colon Cancer?

People in their mid 30s get colon cancer.
Many doctors don’t first suspect this in a symptomatic 30ish person, and the disease thus progresses until it’s finally diagnosed.
At the age of 35, the last thing Dr. Stan Frager was worried about was colon cancer.
On family vacation, Stan’s dad noticed that Stan had bleeding in his urine, and recommended that he see a doctor.
Upon returning from vacation, his father called Stan every day until he got screened.
35 too Young?
Stan says, “I only agreed to be examined to get him off my back.” Up until that point, he had been ignoring the bleeding in his urine, figuring it would go away.
But following a biopsy, a doctor informed Stan he had stage three colon cancer; his colon wall was penetrated, and he had a 90% morbidity rate.
“My father saved my life,” says Stan. Following a surgery, he went into stage 5 radiation treatments — the highest treatment available.
Before his diagnosis at age 35 for the colon cancer, Stan was an athlete and the baseball coach at the University of Louisville, Kentucky, where he was also a professor of psychology.
He had spent years in a medical environment and knew his way around the hospital, but never thought to get screened for colon cancer.
After his surgery he spent the rest of the baseball season coaching the team from the dugout, where he sat on a doughnut while he healed.
Despite the grim diagnosis, Stan has been a survivor for 38 years as of March 6, his surgery date.
He now has two full grown children, one of whom is a 28-year-old male who has already had a colonoscopy.
Stan hopes that audiences will take two simple messages away from his story:
- Know the symptoms and signs of colon cancer.
- Get checked out if something doesn’t seem right.
Age 35 is not too young to develop colon cancer.
“I spent 12 years in academia, and I was stupid. My, and many others, most common thoughts are ‘Why me? Maybe it’ll go away. I won’t get cancer.’ Then I did,” says Stan.
“This could have been prevented if I just took my head out of the sand.”
To learn more about this unforgiving disease, visit the Colon Cancer Prevention Project.
How often do people in their 30s get colon cancer?
Of all the cases in the U.S., the percentage of colon cancer patients between 20 and 34 is 1.4 percent; and between 35 and 44 is 4.2 percent.
There are no statistics that precisely define how many people in their 30s each year are diagnosed with colon cancer.
 Update: Stan Frager passed in 2021.
Update: Stan Frager passed in 2021.
Top image: Shutterstock/Antonio Guillem
Source: seer.cancer.gov/statfacts/html/colorect.html

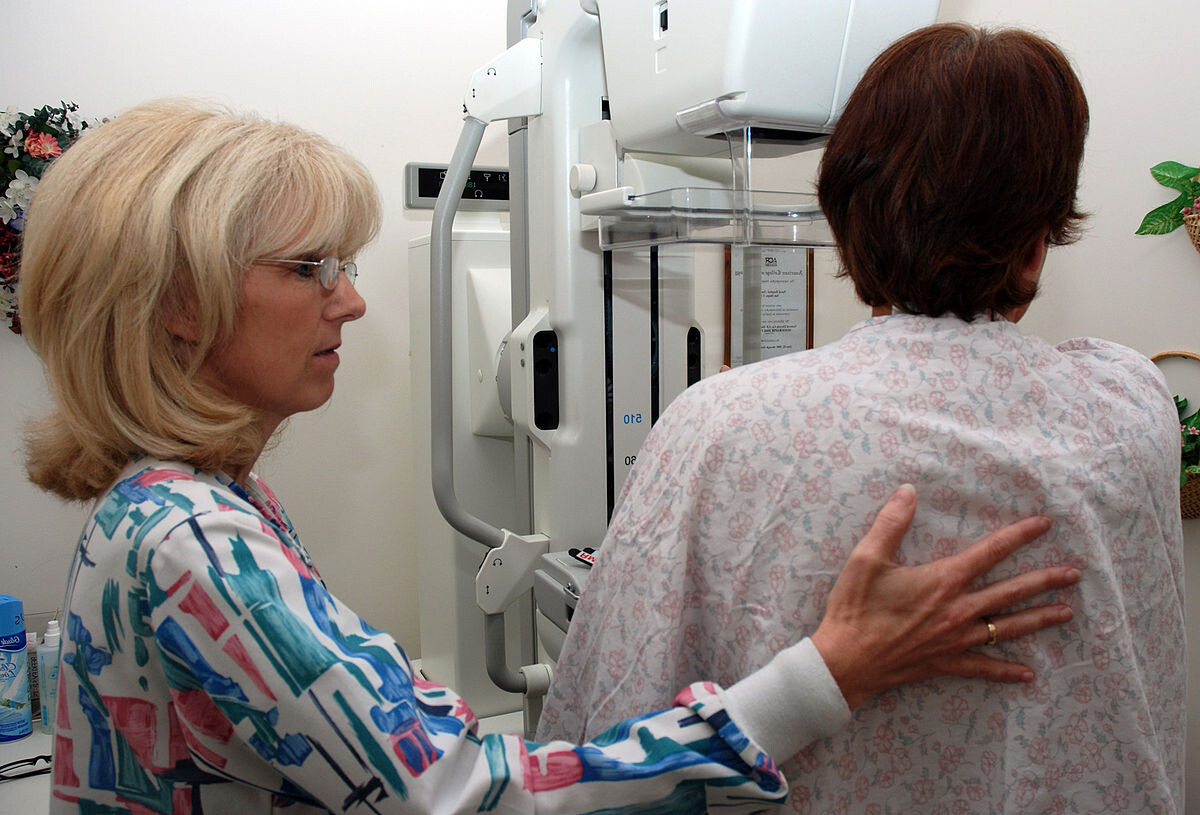
How Often Women with Dense Breasts Should Get Mammogram

Women with dense breasts have a significantly increased risk of breast cancer. Is the yearly mammogram often enough for adequate for tumor detection?
Because dense tissue increases the risk of breast cancer, one may wonder if a woman with dense breasts should have mammograms more often than women without this feature.
“Annual mammogram starting at the age of 40 saves the most lives and is appropriate for women of all breast densities,” says Anjali Malik, MD, a board certified diagnostic radiologist with Washington Radiology in Washington, DC. She interprets mammograms, breast MRIs and ultrasounds, and performs biopsies.
“Breast tomosynthesis [3D mammogram] has improved the detection of small, invasive breast cancers and decreased the ‘false positive’ call-backs,” continues Dr. Malik.
A report in JAMA Internal Medicine (March 2013) says that a study involving over 900,000 women concludes that mammograms once every two years are just as beneficial as annual screenings—even for patients with dense breasts.
The every-two-year screening results in fewer false positives, meaning, fewer indications of malignancy that turn out to be benign.
The researchers (UC San Francisco and Seattle-based Group Health Research Institute) say these recommendations apply to women 50 to 74.
Dr. Malik explains, “In 2013 (the time of the JAMA report), breast tomosynthesis (3D mammography) was not in routine use.
“The 2013 JAMA report was based on 2D analog mammography and prospective data from 1994-2008.
“Currently, 3D digital mammography is in use, and most centers use fellowship trained breast imaging radiologists, where this was not as widespread in the ‘90s and early 2000s. Therefore, this data is near obsolete in 2019.”
What about women in their 40s with dense breasts?
“For women, particularly for those women ages 40-49, who are also more likely to have dense breast parenchyma, nine per 10,000 breast cancer deaths are prevented by annual screening mammograms,” says Dr. Malik.
This data comes from a study by Nelson et al (Annals of Internal Medicine, 164(4):244-55, 2016).
A woman with dense breasts may wonder if more of an important screening tool means better: twice a year mammograms, whether they’re 3D or 2D.
But here’s the problem (other than the extra radiation exposure): Biannual screening increases the call-back rate and the rate of false positives.
This creates tremendous anxiety and sometimes unnecessary biopsies.
Though biannual screening via mammogram has been shown by limited research to result in more cancers detected, it has not been shown to increase survival rates.
Women with dense breasts (as determined mammographically) should ask their doctor about annual 3D mammograms supplemented with annual ultrasounds.
 Dr. Malik is a frequent public speaker and advocate for breast health awareness. She has lectured on the latest advances in breast cancer screening including 3D Mammography™. Follow her on Instagram: @AnjaliMalikMD
Dr. Malik is a frequent public speaker and advocate for breast health awareness. She has lectured on the latest advances in breast cancer screening including 3D Mammography™. Follow her on Instagram: @AnjaliMalikMD
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Source: sciencedaily.com/releases/2013/03/130319144537.htm
Does Back Pain with Chest Pain Mean a Heart Attack?

What are the odds that if you uexplainably feel pain in both your back and your chest that it’s a heart attack?
Perhaps you’ve read that back pain can signal an oncoming heart attack, or occur with the actual heart attack.
Maybe you’ve heard that both back and chest pain can occur with a heart attack.
However, does pain in the back, plus chest, automatically mean that there is something wrong with your heart?
“Not necessarily, but possibly,” says Robert M. Davidson, MD, a cardiologist with SignatureMD.
“If it is associated with exertion or stress, it might be heart related. If it is affected by movement or position, it is more likely to be muscular-skeletal.”
A condition that can cause back and chest pain, upon body position or movement, is costochondritis, an injury to the cartilage in the ribcage. This can hurt pretty bad, but it is benign.
Dr. Davidson continues, “Severe back pain, sometimes radiating to the chest, can be a sign of a leaking or ruptured aortic aneurysm, which is a medical emergency, and should be considered if someone has risk factors such as high blood pressure, older age, or known arteriosclerosis. The type of pain associated with this is often described as tearing.”
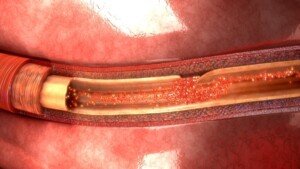
A tear in the inner lining of the aorta. Shutterstock
People who have survived a ruptured aortic aneurysm, or aortic dissection, have also described the feeling as “ripping.”
An aneurysm is an abnormally dilated or enlarged section of an artery.
Usually there are no symptoms until the aneurysm tears. Most aortic aneurysms are discovered by accident via imaging for another issue.
Most non-leaking or non-rupturing aneurysms don’t cause symptoms, but when they do, they may consist of chest, back, neck and jaw pain, a hoarse voice, abnormal stethoscope sounds, coughing and shortness of breath.
An esophageal spasm is another possible cause of chest pain that radiates to the back (including between the shoulder blades).
This is a benign (though sometimes very painful) non-cardiac issue and has no known cause.
Keep in mind that you can have both a musculoskeletal problem and a heart problem — both causing chest and back pain!

Dr. Davidson is with the Division of Cardiology at Cedars-Sinai Medical Center, Los Angeles, and has been practicing for 35+ years. Areas of specialty include coronary artery disease, heart attack and palpitations.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ArtFamily
Source: webmd.com/digestive-disorders/tc/esophageal-spasm-topic-overview

How Are Kids and Teens Treated for Blood Clots?

Yes, children, teens and young adults can develop a potentially fatal blood clot, also known as a deep vein thrombosis (DVT).
Even fit kids, under the wrong circumstances, can end up with this serious condition that demands immediate treatment.
Blood clots in kids, as well as in adults, pose a serious risk because they can break loose and travel to the lungs, resulting in a potentially life-threatening condition known as a pulmonary embolism.
When a blood clot lodges in the lungs, it obstructs blood flow, which can lead to sudden and severe symptoms such as difficulty breathing and chest pain.
A pulmonary embolism may cause rapid onset of shortness of breath, sharp or stabbing chest pain, and in some cases, even coughing up blood.
Immediate medical attention is crucial for managing a pulmonary embolism, as prompt treatment can significantly impact the outcome and reduce the risk of severe complications or death.
Young adults and children are not immune to DVT , which is a blood clot in a vein.
DVT stands for deep vein thrombosis. It’s a clump of blood — a sticky thick network of blood cells — attached to the inner wall of a vein, obstructing blood flow.
“Kids and teens are treated for blood clots according by identifying the underlying cause of the blood clot,” says Dr. Lisa Lewis, MD, a board certified pediatrician in Fort Worth, Texas, and author of “Feed the Baby Hummus, Pediatrician-Backed Secrets from Cultures Around the World.”
“Typically, blood clots are treated with an anticoagulant [blood thinner] and sometimes aspirin.”
Blood thinners would include heparin, or its low molecular weight version, given with warfarin (Coumadin), or just warfarin alone.
The INR blood work is taken on a scheduled basis so that the effect of the anticoagulant drug can be monitored to ensure it stays within therapeutic range.
“Although uncommon, a large percentage of blood clots in children and teens are inherited,” says Dr. Lewis.
What if a child or young adult has an acute, large DVT?
A large deep vein thrombosis can completely obstruct flow of blood from a limb.
In this case, other medications may be used early on, such as a thrombolytic (clot-busting) agent. This would be followed by anticoagulant medications.
Long-term management of deep vein thrombosis (and pulmonary embolism) in kids:
1) The safe prevention of additional DVTs is emphasized
2) Management is designed to enable the young patient to function as normally as possible.



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}