
DVT Risk During Long Flights vs. Long Car Rides, Movie Marathons
Find out if sitting for prolonged periods on an airplane is worse than sitting for extended periods in a car or on your sofa for DVT risk.
Maybe you keep hearing about how prolonged sitting during air travel is a risk factor for developing a deep vein thrombosis.
In fact, major airlines, on their planes, provide pamphlets that even explain what to do to lower the risk of developing a DVT from a long flight.
But what about sitting virtually immobile in a deep comfy chair or sofa while watching hour after hour of movies or sitcom reruns, not even getting up to use the john?
Or sitting for extended periods, legs with limited space to move, in a motor vehicle?
Developing a DVT from extended air travel is called “economy class syndrome” because the economy seats don’t allow much room for leg movement.
This is a real concern, says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
“One study showed that the frequency of a PE [pulmonary embolus] was much greater in patients who traveled greater than 5,000 kms compared to those who traveled less than that,” continues Dr. Casey.
What about DVT from long car rides?
“The increased risk during air travel is probably not more than a similar population traveling in a car,” says Dr. Casey. So why isn’t there a lot of media attention to long car travel or even movie marathons at home?
“It is either less discussed and/or less studied,” Dr. Casey says. “But the same risk does apply during prolonged automobile travel and any other period of prolonged immobility.
“The World Health Organization has stated that such an association is likely to be small and mainly affects passengers with other risk factors for VTE [venous thromboembolism].”

DVT prevention exercises while on a flight or in a long car ride
In addition to prolonged immobility, DVT risks include:
Recent joint replacement, abdominal or heart surgery
Obesity
Lack of regular exercise
Dehydration
Pregnancy
Smoking
Increased age
Previous DVT
Clotting disorder
 Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Can You Get a Blood Clot (DVT) from Lifting Weights?

A vascular surgeon answers the question of can lifting weights cause a blood clot (deep vein thrombosis).
Many bodybuilders and those who lift weights want to know if weightlifting can somehow cause a DVT.
Sometimes, it certainly must feel that way, as the athlete strains with heavy compound lifts, especially if the athlete sees their veins “popping” or “bulging” as they struggle with the load.
Another reason those who strength train or work out with weights may wonder about blood clots is because often, they strive to attain vascularity in their appearance, and this makes them think of veins.
All in all, muscle builders and other kinds of weight lifters will sometimes wonder about deep vein thrombosis, though they may not refer to it as that, and instead call it “blood clot.”
What the Doctor Says
“I suspect what this discussion is focused on is Paget-Schroetter syndrome or subclavian vein effort thrombosis,” says Kevin Casey, MD, FACS, a vascular surgeon with West Coast Vascular.
“This is an acute occlusion [blockage] of the axillo-subclavian vein [runs under the clavicle] and is classically found in an otherwise healthy young male who is an avid weightlifter.
“However, it can also be found in pitchers, volleyball players, tennis players, etc.”
What causes this?
Dr. Casey explains, “It is caused by compression of the vein by the musculoskeletal elements of the thoracic outlet.
“It accounts for approximately 1% of acute venous thromboses.
“The treatment involves chemical thrombolysis [blood thinners] of the vein followed by removal of the ipsilateral first rib and scalene muscles.”
Dr. Casey specializes in vascular and vein therapy, and has been the lead researcher on publications examining abdominal aortic aneurysms, carotid artery disease and lower extremity critical limb ischemia.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Super Morbidly Obese: Manipulating Their Enablers

Ever wonder what on earth is going on in the heads of the “caretakers” to the super morbidly obese?
These 600 to 1,000 pound men and women are confined to their bed, so it’s impossible for them to get food.
What makes a person keep bringing tons of junk food to a super morbidly obese family member who’s so huge they can’t even get out of bed?
Or if they CAN get out of bed, they’re certainly too fat to get food, let alone prepare and cook it.
So instead they somehow persuade their enabler to continue bringing them thousands of calories worth of unhealthy food by the hour.
What kind of manipulation skills can these super morbidly obese, bedridden men and women, possibly have?
What kind of power do they possess over their enablers?

Or perhaps it’s more of a situation that their enablers (spouse, significant other, parent, grown child, sibling, even non-relative friend) are just very mentally frail.
“As is the case with drug addiction, changes in the chemistry of the brain can cause people struggling with food addiction to manipulate others,” explains David Sack, MD, a psychiatrist specializing in addiction disorders, and CEO of Promises Treatment Centers in Malibu and Los Angeles.
Their drug of choice is food. And tons of it.
What’s mind-blowing is how a physically incapacitated person with little money can exert control over an able-bodied person who has a car.
“If the enabler tries to stop enabling, the food addict may use a number of strategies to elicit compliance,” says Dr. Sack.
“They may use threats, guilt and heartbreaking pleas that are extremely persuasive,” says Dr. Sack, “especially when used against someone who is codependent.”
The TLC program, “My 600 Pound Life,” never shows the super morbidly obese person exhibiting behavior that puts a stranglehold on the enabler. At least not in my opinion.
For instance, maybe some viewers found “Penny” or “James” to be intimidating. But I sure didn’t.
At the most, the 600+ pounder is shown pouting or whining, occasionally raising their voice – but nothing that would – or should – paralyze the enabler with the fear of “I better bring her three Big Macs or else I’m doomed.”
In other words, the hissy fits when food is occasionally delayed or denied amount to little more force than what a toddler can exert.
Yet the enablers eventually give in. Of course, the dynamic usually (not always) changes once the 600 pounder commits to losing weight to qualify for weight loss surgery.
• I’m sure that the more dramatic fits are edited out.
• Nevertheless, why can’t the enablers just ignore them?
• How about leaving the home when they occur?
• Or popping in ear plugs?
• There ARE options.
The enabler is not the one in control.
The enabler, on a superficial level, seems like the one in control. You’d think that anyone who wipes your fanny would have complete control over you. But it’s the bedridden individual who wears the crown.
Can the Enabler Sometimes Be the One in Control?
However, sometimes it is the enabler who IS in control, and thrives on this control – even if it comes with the daily wiping of grime out from in between huge folds of sweaty fat.
“Those who are morbidly obese are also vulnerable to being manipulated by the people around them,” says Dr. Sack, “who may have their own unconscious emotional needs,” such as relishing being so needed.
 Dr. Sack is a sought-after media expert and has appeared on “Dateline NBC,” “Good Morning America,” “The Early Show,” and “The Doctors,” among many other outlets.
Dr. Sack is a sought-after media expert and has appeared on “Dateline NBC,” “Good Morning America,” “The Early Show,” and “The Doctors,” among many other outlets.
 Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Bulging Disc: How Long to Try Conservative Treatment?

Find out how long you should give conservative treatment a try before having surgery for your bulging (herniated) disc.
If you’ve been diagnosed with a herniated (bulging) disc, you should not rush into the decision to have surgery.
The overwhelming treatment of choice for a herniated disc is conservative — even if the pain is pretty bad.
You may want to get a second opinion if you feel that a recommendation for surgery is coming prematurely.
But the Fair Question Is…
However, how long should you try the conservative approach before it’s fair to conclude that it just won’t solve the problem?
- Cold packs
- Warm packs
- Physical therapy
- Floor stretches
- Yoga
- Acupuncture
- Over the counter pain relievers
“The timing of non-operative care depends on the individual scenario,” says Dr. P. Justin Tortolani, an orthopedic surgeon and spine specialist with University of Maryland St. Joseph Medical Center.
“If someone presents with a weakening in the leg or foot, we might watch cautiously for a few weeks.
“It means that the nerve is compressed by the disc herniation and is being damaged, and generally, means the nerve fibers in each nerve have been compromised so that they’re not transmitting signals to the muscles.
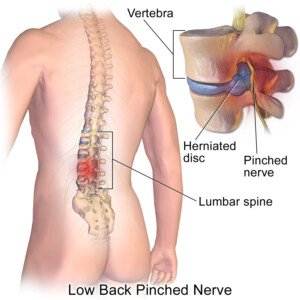
BruceBlaus/CC
“It can be permanent and that’s why we have a lower threshold for considering surgery in a patient who has weakness and is not improving.
“It’s also important to rule out other causes of weakness even with someone with a disc herniation, like Lou Gehrig’s disease or trauma, or syphilis.
“If they present with severe weakness and are showing improvement, they will continue to watch and continue to use non-operative treatment.
“Even with pain, if they are showing signs of strength coming back, we’ll continue to treat without surgery.”
As far as physical therapy, which may be done at home, the patient needs to faithfully stick to the entire exercise regimen in order to give it a fair chance.
Improving symptoms from a herniated or bulging disc through physical therapy can take time.
PT focuses on reducing pain, restoring mobility and strengthening muscles around the spine.
Techniques may include exercises, stretches and manual therapy.
Patience is very important, as it often takes weeks or even months to see significant improvement.
Progress varies based on the severity of the herniation, individual health and adherence to the therapy plan.
Regular follow-ups with the therapist ensure that the treatment is effective and adjusted as needed.
 Dr. Tortolani’s vast experience includes treating all disorders of the spine including herniated discs, spinal stenosis, and adult and adolescent scoliosis.
Dr. Tortolani’s vast experience includes treating all disorders of the spine including herniated discs, spinal stenosis, and adult and adolescent scoliosis.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/TB studio

Can Swollen Anus in Cat Be Caused by Cancer?

How often do you inspect your cat’s anus? Sure, many cat owners don’t like to do this, and in fact, outright avoid it.
However, if your beloved cat has a swollen anus, this can be caused by cancer, says veterinarian Dr. Jules Benson, BVSc, chief veterinary officer with NationwideDVM, a pet insurer company.
Swollen Anus in a Cat: Common Cancers
“Yes – swellings or visible masses around the anus can be caused by cancerous growths,” says Dr. Benson.
The most common abnormal growths in the anal area of a cat are anal gland adenocarcinoma and fibrosarcoma.
“Your vet can help to determine what the cause might be by examining your pet and taking biopsies of any swellings,” says Dr. Benson.
“Unfortunately, adenocarcinoma and fibrosarcoma do not have good prognoses, but evaluation by a veterinarian or even consultation with a veterinary oncologist can result in positive outcomes.”
Treatments Are Expensive
“While these treatments are often expensive, having pet insurance that covers standard cancer treatments can make the difference between being able to pursue the most cutting-edge treatment options, versus palliative care to just keep your pet comfortable,” says Dr. Benson.
 Dr. Benson is regularly consulted by many media outlets including ABC, NBC, FOX, The Wall Street Journal and The New York Times to provide pet health advice to pet parents nationwide.
Dr. Benson is regularly consulted by many media outlets including ABC, NBC, FOX, The Wall Street Journal and The New York Times to provide pet health advice to pet parents nationwide.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Shoulder Pain but No Other Symptoms?

Orthopedic surgeon Dr. Mark Galland talks about causes of shoulder pain in the absence of other symptoms.
“Shoulder pain, in the absence of any other symptoms, is most commonly caused by a rotator cuff tear or tendonitis, bursitis, or osteoarthritis,” says Dr. Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
The Rotator Cuff
The rotator cuff is composed of four muscles and their tendons that form a “cuff” around the shoulder joint, enabling a wide range of motion from the shoulder.
These muscles not only facilitate movement but also provide essential stability to the shoulder.
They act as dynamic stabilizers, supporting larger, inherently stronger muscles like the deltoids and latissimus dorsi during upper body activities, particularly that of strength training and throwing.
Tendonitis
Tendons join muscle to bone. Tendons are vulnerable to inflammation when overused.
In the case of shoulder pain, the tendons involve the rotator cuff. Pain from rotator cuff tendonitis is notorious for “referring” or “radiating.
In other words, you may feel pain at the side of your upper arm, just below the shoulder, even though the origin of the problem is higher up within the shoulder joint.
Bursitis
This is nflammation of the bursa, sac-like structures in the shoulder joint.
A bursa is fluid-filled and cushions a joint. The pain may feel achy or sharp and often worsens with movement or pressure.
However, bursitis pain can actually come and go, especially with activity levels, repetitive motion or if the underlying cause isn’t consistently addressed or treated.
Osteoarthritis
This is inflammation and wearing down of the cartilage that provides shock absorption between bones.
“When the shoulder pain is accompanied by numbness or tingling into the arm or hand, this strongly indicates a pinched nerve in the neck.
“Sometimes shoulder problems in and of themselves can cause numbness to occur, but it is more often indicative of a problem in the neck.”
Cancer Can Cause Shoulder Pain
A rare cause of shoulder pain when there aren’t any other symptoms is a tumor of the lung.
The lungs sit beneath the shoulder nerves. If the tumor is pressing on one of these nerves, pain can result.
But you must realize that this is very rare, especially if it’s not accompanied by other symptoms such as persistent cough, shortness of breath, undue fatigue or unexplained weight loss.
 Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/KlaraBstock

Can Deep Squats Harm the Knee: Orthopedic Surgeon’s Response

Can deep knee squats hurt the knees?
Assume the squats are executed with feet flat on the floor, and that “deep” means the thighs have surpassed the position of being parallel to the floor.
That’s the question I posed to Dr. Mark Galland,orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
“Performing deep squats does not necessarily cause direct harm to the knees,” begins Dr. Galland.
He also points out three conditions that can be conducive to an increased risk of injury or pain to the knees. They are as follows:
“(1) an increase in the bend of the knee or depth of the squat,
(2) over an extended period of time, or
(3) with greater frequency of the activity.”
Keep on Squatting—Smart and with Good Form
“That is not to say that doing deep knee squats should be considered an unsound movement; it only means that, in some cases, caution should be used in order to reduce the chance of injury.”
People who “injure” or “hurt” their knees deep squatting most likely executed poor form, such as tracking the knees ahead of the feet.
This can happen if their heel is elevated on a plank of wood, or if they dorsiflex at an unusually large range of motion (i.e., the “ankle flexibility” that’s needed as one descends into the squat).
Exaggerated dorsiflexion can cause the knees to travel well-ahead of the feet.
Another source of harm can be the knees not tracking properly over the feet, meaning, the knees point out at a certain angle, but the feet don’t match up with this angle.
“Deep knee squatting under extreme weight can also sometimes result in cartilage tears, and prolonged, repetitive deep squatting over a period of time may carry the risk of leading to arthritis under the knee cap, but the likelihood can be minimized by controlling the risk factors above,” says Dr. Galland.
“As with many exercise-related movements, it is reasonable to propose that the potential benefits derived from strengthening the muscles surrounding the knee as a result of doing the squats may outweigh the relatively small risk of injury associated with the movement.”
As a former certified personal trainer, my recommendation is to know the risk factors, concentrate very seriously on executing textbook form, and include squats in your fitness program.
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Pressmaster

Causes of Sharp, Stabbing Pain in Knee when Walking

An orthopedic surgeon names causes of a sharp, stabbing pain in the knee when walking.
“Knee pain experienced during moderate movement such as walking may be caused by any number of factors, including tendonitis, a cartilage tear, arthritis or a pre-arthritic condition,” states Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
Treatment
“Treatment options depend entirely on determining the location and source of the pain, and may include ice massage of the sore area, bracing, anti-inflammatory medication, stretching the hamstring and quadriceps muscles, and modifying your activity for a brief period of time to prevent any aggravation of the area,” explains Dr. Galland.
“These steps would all be reasonable to take regardless of the cause, but ideal treatment would depend on isolating the location and the underlying cause of the pain.”
In rare cases, stabbing knee pain while walking can point to serious problems like a ligament rupture or a stress fracture.
Infections, blood clots or bone tumors can also cause sharp pain, though these are uncommon causes in this context.
Most knee pain isn’t a sign of a serious disorder, but persistent, worsening pain deserves medical attention.
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/sukiyaki
Grinding Noise in Knee, No Pain: Should You Worry?

What can cause a grinding noise in the knee but no pain, and is this something to be concerned about?
“Painless noise in the knee, as well as other joints, can be safely ignored,” says Dr. Mark Galland, orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
“Noises in the knee are fairly common and do not necessarily signify anything significant, although the most common diagnosis associated with a noisy knee is arthritis or pre-arthritis under the knee cap.”
Another Cause of Grinding Sound
“The second most common cause is a painless bursitis behind the knee cap,” says Dr. Galland.
“In arthritic knees, there may be a sound associated when there is bone-on-bone contact; however, the noise associated with this is usually more subtle than the more dramatic noise some patients experience from the benign causes mentioned above.”
Can this morph into a more serious problem and if so, why?
“Surprisingly, a grinding noise in the knee is almost always benign, but any audible symptom, especially if accompanied by pain, should be checked out by a primary care provider or an orthopedist just as a precaution.”
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: ©Lorra Garrick

Questions to Ask Your Surgeon Prior to Knee Arthroscopy

An orthopedic surgeon explains what questions one should ask about their upcoming knee arthroscopy.
Don’t just go into a knee arthroscopy blindly. You should be armed with knowledge ahead of time.
Nature of the Knee Arthroscopy and Description
“A patient should ask the surgeon exactly the nature of the procedure and a description of what will be taking place during the arthroscopy,” says Dr. Mark Galland,orthopedic surgeon, sports medicine specialist and physician at Orthopaedic Specialists of North Carolina.
Ask the surgeon to explain the procedure with a model of the knee joint.
If one is not in the office, your doctor can use a 2D illustration or perhaps already has a favorite video showing the procedure in animated form.
Surgeon’s Expectations of a Successful and Unsuccessful Knee Arthroscopy
“The patient should also ask the surgeon to state his or her expectations of the procedure if it is successful,” says Dr. Galland.
Make sure that the information you get goes beyond just a generic template.
For instance, how soon will you be able to return to your favorite physical activities?
“A surgeon should be able to offer the patient an overview of the long-term ramifications, both in the case of a successful procedure as well as an unsuccessful procedure.”
Recovery Expectations
Finally, Dr. Galland says, “A patient should also ask what they can expect regarding recovery, including how long until they can walk and return to normal activity, as well as what the restrictions may be during convalescence.”
Another question to ask your surgeon about knee arthroscopy is about possible complications and what will be done to help reduce them.
Another good question is about the type of anesthesia (general, regional or local?).
Ask your doctor if you can record the Q & A on your phone.
This way when you wonder about a particular answer, you can conveniently play it back.
Dr. Galland has authored many book chapters and papers in sports medicine. His advice and consultation have been sought by world-class athletes in track and field and Major League Baseball.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.

































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}