

Can Liver Disease Odor Really Smell Like Bleach?

A GI doctor addresses the question of can liver disease cause a bleachy odor.
Have you ever seen references online stating that liver disease can cause an odor in the patient that’s like bleach or “bleachy”?
“No, it does not smell like bleach,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“It’s hard to describe, but it’s usually a very distinct, very pungent odor, and it’s called fetor hepaticus.
“It’s unclear whether it’s ammonia, ketones and/or dimethyl sulfide, but by the time a patient is experiencing this, their liver is in bad shape.”
Perhaps whoever wrote that the odor of liver disease smells like bleach was instead thinking of ammonia.
What about an ammonia smell associated with liver disease?
Dr. Fine says, “The smell associated with liver disease is very distinct and extremely pungent.
“It may be ammonia-like, but it is not the same as the smell of a baby’s diaper (which can smell like ammonia) or sweat from a healthy individual after exercising (some exercisers report an ammonia smell post-workout).”
The odor of liver disease will emanate from a person’s mouth.
Spouses of patients have described the smell as that of “sweet and fecal.”
By the time a person’s liver disease begins causing a maladorous body or breath odor, there will be other symptoms present, such as jaundice, fatigue, unexplained weight loss, nausea and appetite suppression.
Pungent armpit odor in an otherwise healthy person is not a sign of liver disease.

Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
 Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Source: healingwell.com/community/default.aspx?f=25&m=2084180

What Part of the Body Does Liver Disease Odor Come From?

Liver disease can cause a strong body odor, but just what does this mean?
What body part does this stink come from? Is it the entire body or some localized area like the armpit?
You may have read online references to “body odor” when it comes to liver disease, but not much more information than that.
When liver disease causes a change in body odor (regardless of the type of odor), a specific region of the body emits this.
“The odor is caused by the inability of the liver to break down proteins correctly,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“It’s coming from the lungs through the mouth. It’s seen in portal hypertension, where there’s significant portosystemic shunting.”
In portal hypertension there is increased blood pressure in the portal vein, which carries blood from the digestive organs to the liver.
This elevated pressure often results from liver diseases, such as cirrhosis, where scarring blocks blood flow and forces the blood to find alternative routes.
The increased pressure can lead to complications like variceal bleeding (enlarged veins that can rupture), ascites (fluid accumulation in the abdomen) and an enlarged spleen — along with the odor.
A portosystemic shunt means that the vascular connection between the GI tract and liver, due to a pathology, is bypassed (shunted).
“This is a late sign of liver failure,” says Dr. Fine. “Individuals who are experiencing this body odor are in bad shape and should’ve already been seen by a liver transplant hepatologist and surgeon.”
Does it occur even if the patient is NOT perspiring?
Dr. Fine says, “Yes. The odor is caused by the inability of the liver to break down proteins correctly. It comes from the lungs through the mouth.”
You can be a nondrinker and still acquire liver disease. Risk factors for liver disease include excessive alcohol consumption, which can lead to fatty liver disease and cirrhosis.
Viral infections such as hepatitis B and C are also significant contributors, as they can cause chronic inflammation and damage to liver cells.
Obesity and type 2 diabetes increase the risk of non-alcoholic fatty liver disease (NAFLD), which can progress to more severe liver damage.
Certain medications and toxins, as well as a family history of liver disease, can further increase susceptibility.
Can the development of the change in odor occur suddenly, and/or is it usually over a long period of time?
Dr. Fine explains, “The smell can wax and wane, but by the time a person experiences it, they are already in the advanced stages of liver disease.”
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/Nerthuz

Can Bad Body Odor Be the Only Symptom of Liver Disease?

If you begin noticing your body is starting to smell bad, but you feel fine otherwise, is it possible this can be early liver disease?
What if you wash and shower and it doesn’t go away? Have you been wondering about this?
By the time liver disease causes a malodorous odor…does the patient necessarily have other symptoms of this liver disease?
“This odor is indicative of advanced liver disease,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“If a patient’s condition has progressed to this state, other symptoms are likely to be present.”
And those other symptoms would be some or all of the following:
- jaundice
- upper stomach pain
- fatigue
- weight loss
- distended belly
- loss of appetite
- nausea
- vomiting
- chalk-colored or greyish stools.
Can a bad body odor be the only symptom — even temporarily? And then could other symptoms would soon follow?
“Generally speaking, by the time a patient has the bad odor associated with liver disease, they’re in an advanced stage and other symptoms will likely be present,” says Dr. Fine.
“However, these symptoms may improve if the liver function improves.”
Where in the body does this smell come from? Armpits?
“I have not seen a case where the odor only came from the armpit,” says Dr. Fine.
“In the cases I’ve seen, the odor comes from the lungs through the mouth.”
What types of liver disease cause this bad odor?
“All types of liver disease affect body odor like this, but only if they’re in liver failure,” says Dr. Fine.
“The bad odor is caused by the inability of the liver to break down proteins correctly.”
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/ESB Professional
Why “Sitting Disease” Is the New Smoking, plus Solutions
At least four hours a day of sitting is dangerous to health, increasing mortality, heart disease, diabetes, cancer, blood clot risks and more.
Do YOU have the “sitting disease”?
Who would have ever thought that spending lots of time every day in a nice comfy chair could be so threatening to one’s health?
But the research can’t be ignored, and it’s mounting more and more.
You may be wondering, Where was all this research 10 years ago?
Well, just because it took a long time for medical researchers to catch on to the sitting disease, doesn’t mean it doesn’t exist.
Just like with smoking. For years, attention to the harm of smoking was well under the radar, but gradually over time, as study after study proved that smoking is dangerous to health, people became increasingly aware of smoking’s harm to the body.
Similarly, information on the dangers of prolonged sitting has really picked up steam, and there are no studies that contradict the existence of sitting disease.

Shutterstock/FrameStockFootages
Our ancient ancestors, and modern-day hunter-gatherers, do not spend hours and hours sitting like people in industrialized societies do.
Prolonged sitting goes against the nature of our body.
The scary thing about all this is that even strenuous exercise sessions, done DAILY, will NOT offset the negative health effects of sitting for hours every day!
So if you’re hitting the gym like a grizzly bear several times a week, bench pressing and deadlifting hundreds of pounds, dripping sweat from your Tabata workouts and heavy-bag routines…guess what:
This is why it’s so very important to avoid sitting for longer than one hour at a time.
In fact, it would be very wise to get up every 30 to 45 minutes if you know you’ll be sitting for a very long time doing computer work at home or on the job.
“If a person goes on an eight hour flight, they will usually be very aware of the DVT risk,” says Dr. David Beatty, MD, a retired general practitioner with 30+ years of experience and an instructor of general medicine for 20+ years.
A DVT is a deep vein thrombosis: a dangeorus blood clot.
“They’ll do leg exercises, move the calf muscles, get up for a walk to stretch the legs,” continues Dr. Beatty, referring to people in airplanes.
“Do they do any of this when they sit behind a desk for the working day?”
The answer is no, strangely enough — no for many of them.
But excess sitting on land — at home or in the office — increases the risk for DVT.
Excessive sitting, regardless of your fitness habits, is an independent risk factor for various conditions, including increased risk of death from any cause.
Sitting Disease Solutions
– Get a treadmill desk and do as much computer use as possible on it.
– Stand or pace while watching TV, even if it’s just during commercials.
– Stand while on the phone.
– If you don’t have a treadmill desk for computer work, set a timer that goes off every 30 to 45 minutes, then get up and do something, anything (chores, calve raises, pushups, marching in place, watering the houseplants, playing with the dog, etc.)
– Stand while eating.
 Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
Dr. Beatty has worked in primary medicine, surgery, accident and emergency, OBGYN, pediatrics and chronic disease management. He is the Doctor of Medicine for Strong Home Gym.
 Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.

Barefoot Walking on a Treadmill Desk

Don’t walk barefoot on your treadmill desk, even if you love to go around your home barefoot.
Walking barefoot on a treadmill desk is not a good idea.
In fact, there’s really no logical reason to walk barefoot on a treadmill desk.
You may have read that barefoot running has some benefits.
Though the verdict on this is still a bit foggy, there are studies that show running barefoot for some of your runs may be worthwhile.
A Harvard University study endorses barefoot running outdoors.
So one might gather that jogging around without shoes means that it’s safe, even beneficial, to walk without shoes on a treadmill desk.
Shoeless Walking
Modern-day hunter-gatherers, who go just about everywhere barefoot, walk on mostly natural surfaces (think soft earth).
However. the tread belt of any kind of treadmill is a very unnatural surface.
- It’s not earth.
- It’s made in a factory.
- It doesn’t give.
- It’s hard.
- This can hurt your feet over time.
In fact, if you were to try walking, even very slowly, on your treadmill desk in your bare feet, it should start getting uncomfortable within minutes.
The benefits of barefoot running or walking on earth do not carry over to a machine’s tread surface.
I have a treadmill desk. I’ve used it while my feet were in socks with “booties” over them, and even THEN, just 10 minutes of doing this for the first time became uncomfortable.
The only reason I did it was because I was too lazy to put on shoes.
Walking barefoot on a tread surface can lead to repetitive stress injuries including strain of the toes; it’s happened to me while wearing the sock-bootie combo.
Wear what’s comfortable. There’s no reported health or fitness advantage to going barefoot on a treadmill desk.
There’s also no science (so far, anyways) that supports the idea that wearing comfortable and supportive walking shoes while on a treadmill will cause harm.
I suppose it’s just a matter of time before someone comes up with a treadmill desk with a cushion-like belt.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Shutterstock/Sachoneman

Men Who Exercise but Sit a Lot at Risk for Heart Failure
Men who have a desk job have an increased risk of heart failure even if after work they hit the gym like a warrior–not exactly the news you wanted to hear, right?
If you work out like a beast after work, but sit a lot on the job and then also at home, your risk of heart failure increases.
There is a very intriguing study report in the journal Circulation: Heart Failure.
To prevent heart failure, one must take a two-pronged approach: 1) exercise a lot, and 2) avoid prolonged sitting. “Be more active AND sit less,” says lead study author Deborah Rohm Young, PhD, in the paper.
The Study
A racially diverse group of over 84,000 men, from age 45 to 69, without heart failure at the get-go, were followed for about eight years.
The Results
Men with a lot of inactivity were 52 percent more likely to acquire heart failure than were men with high activity levels.
This isn’t just about structured exercise sessions, but overall movement that was carried out beyond the workplace (the study didn’t account for movement on the job).
Beyond the workplace, men who spent at least five hours a day in a chair were 34 percent more likely to acquire heart failure than were men who sat around for less than two hours a day.
This higher heart failure risk was independent of how much they engaged in structured exercise.
For men who sat for a minimum of five hours a day, and did little structured exercise, risk of heart failure was doubled that of men who exercised a lot, as well as spent under two hours a day sitting.
Study Limitations
The results may not apply to women; physical activity was self-reported, and thus, may have been over-reported; results were based strictly on time outside the workplace.
How to Oppose the Sitting Disease
A lot of home sitting time is done while a person works on a computer. How about getting a treadmill desk?

If you’re entrenched in computer activity, you’ll forget you’re walking. I know; I have a treadmill desk.
Set the speed to even one-half mph, and this is all you need to oppose the sitting disease.
Another way to reduce sitting time and lower heart failure risk is to (yes, I’m serious) watch TV while standing. But you should move around a bit while standing.
Less Sitting Time at the Gym
The study shows that gym time alone isn’t enough to fight off the sitting disease.
How much sitting do you do while at the gym in between sets?
You may be on your can far more than you think, what with texting and other phone use in between sets.
Stand while using your phone.
Walk around in between sets instead of sitting on a bench.
If you think someone will grab your seated equipment if you leave it, then pace very close to it, or at least stand beside it — anything to get off your butt.
Lorra Garrick is a former personal trainer certified through the American Council on Exercise. At Bally Total Fitness she trained women and men of all ages for fat loss, muscle building, fitness and improved health.
.
Top image: Freepik.com
Source: sciencedaily.com/releases/2014/01/140121164743.htm
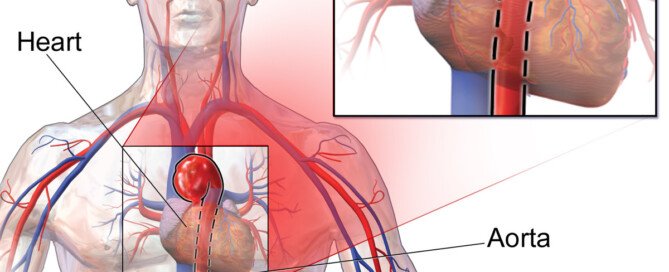
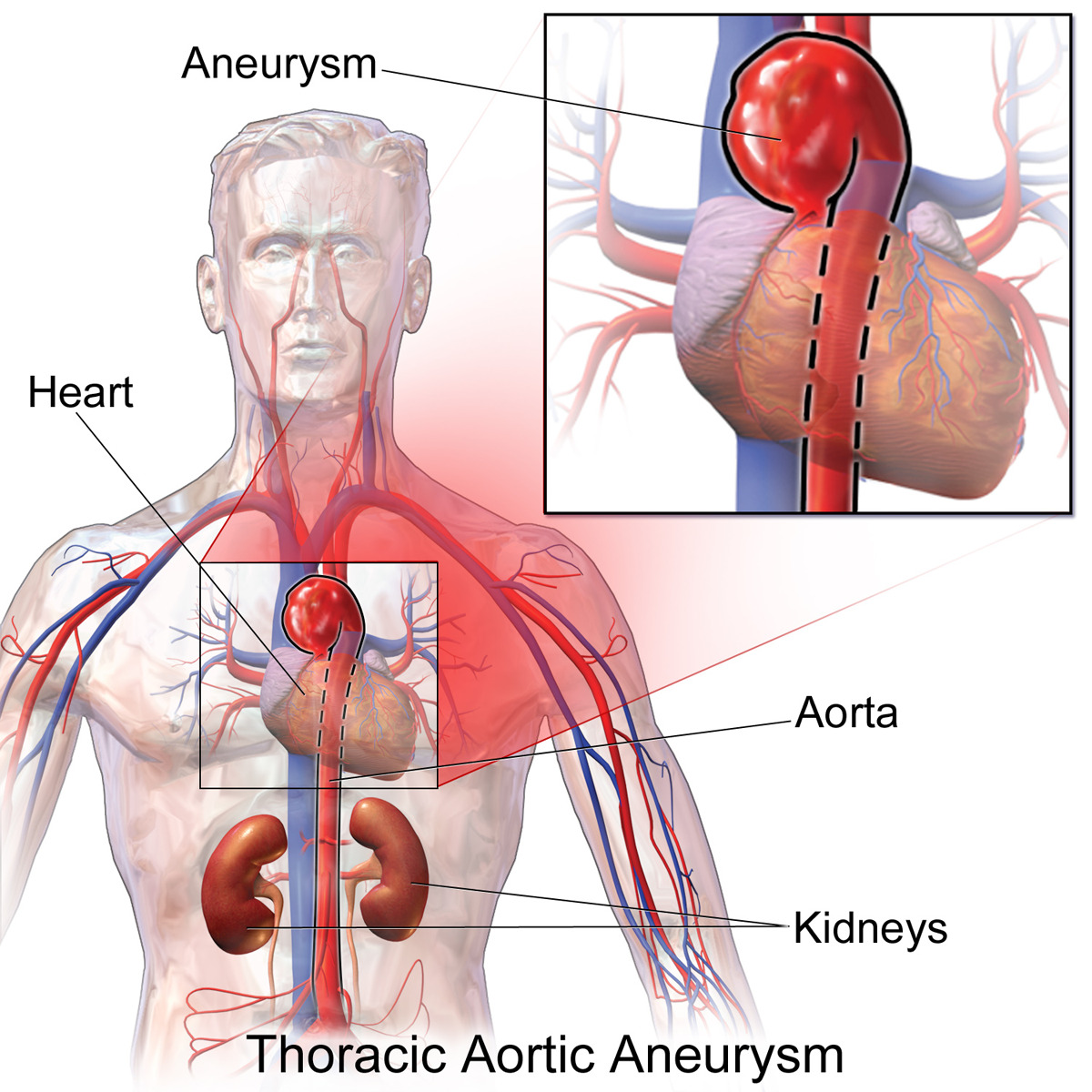
Ascending Aortic Aneurysm Stent Graft Repair Is Here
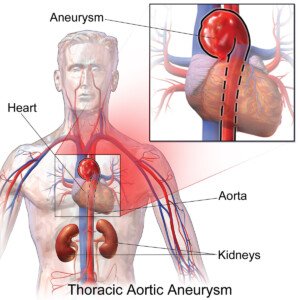
Stent graft technology for the repair of an ascending thoracic aortic aneurysm is a marvel of medical advancement.
Stent technology continues to evolve; soon, endovascular repair (stent grafting) will be more common with ascending aortic aneurysms.
Currently, fusiform ascending aortic aneurysms cannot be repaired with stent grafting (endovascular repair) because the placement of the stent requires landing zones.
The ascending aorta has openings that are formed from the vessels that branch off the top of it where it begins arching.
A stent graft would overlap one of these openings in order for the graft to be set in place.
If one of these portals is obstructed, then adequate blood supply will not flow through the vessel branch and reach other parts of the body.
The descending aorta has no openings formed by vessel branch-offs; hence, stent grafts can be set in place with generous landing zones.
This is why endovascular repair of a descending aortic aneurysm is rather common.
New Stent on the Block

A new kind of stent—multilayer—has been developed, and Grayson H. Wheatley III, MD, is leading the way.
He is an aortic disease surgeon with TriStar Cardiovascular Surgery in Nashville, TN.
“The advantage of this stent is that because the stent has an open structure, it can cover branches without interfering with flow,” explains Dr. Wheatley.
Dr. Wheatley further explains that “the stent can be used in the ascending aorta and if additional landing zones are needed, it can cover the coronary arteries or the great vessels.”
The great vessels are the ones that branch off the aorta’s arch.
“This may be the best solution for ascending aortic aneurysms,” adds Dr. Wheatley.
“There wouldn’t be blood flowing into the aneurysm around the stent except in rare cases where the aneurysm goes all the way to the aortic valve (called aortic root aneurysms).”
When will endovascular treatment of an ascending aortic aneurysm become more common?
“We are working with the FDA to initiate a trial for high risk surgical patients with complex aneurysms.”
Normally, when the diameter of a TAA reaches close to 6 cm, it’s time for repair in a patient who has not been having symptoms, and does not have a connective tissue disorder or a bicuspid aortic valve.
(Patients who do have at least one of these variables have a lower measurement threshold before surgical repair is warranted.)
Learning about this threshold got me thinking about how all of those people, who are under 5.7 cm but greater than 4 cm, must continuously live on what I call the disability list, not to mention the anxiety that a sudden charge of emotions, straining on the toilet or lifting a child might cause a rupture.
Could the new multilayered stent graft lower the threshold measurement?
After all, living with a TAA is unnerving; why wait for it to reach 5.8 cm when it can be endovascularly repaired at 4.5 cm?
Lowering the threshold is a potential possibility, says Dr. Wheatley. “The decision on when to treat an aneurysm is based on the risk of rupture versus risk of surgery.
“With this new stent, the risk of the surgery would potentially be much lower and thus we might be able to treat patients earlier with smaller aneurysms, but this has yet to be studied with this device.”
The evolution of a milestone in stent technology is only beginning; you will be hearing a lot more about this remarkable advance in endovascular stent grafting for thoracic aortic aneurysms.
More About the Stent
Dr. Wheatley explains: “This type of stent functions differently than coronary stents even though they both have an open mesh.
“This stent was developed by a team of engineers who understood fluid dynamics and the role of blood flow in an aneurysm sac.
“These specialists took their understanding of fluids and applied it in a way that no one had previously thought of with regards to treating aneurysms.”
 Dr. Wheatley is an internationally recognized expert in aortic treatments and specializes in open and endovascular repair of complex aortic diseases plus the surgical treatment of coronary artery disease and valvular heart disease. Check out his website.
Dr. Wheatley is an internationally recognized expert in aortic treatments and specializes in open and endovascular repair of complex aortic diseases plus the surgical treatment of coronary artery disease and valvular heart disease. Check out his website.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Shutterstock/BruceBlaus

My 600 Pound Life: Enablers Should Be Questioned

Why doesn’t the show, “My 600 Pound Life,” corner the enabling spouses and require them to explain their actions?
The enabling spouses on “My 600 Pound Life” need to explain why they continue bringing huge quantities of junk food to their bedridden, super morbidly obese partners.
One episode of “My 600 Pound Life” focused on Penny Saeger. She was bound to her bed, and her husband, Edgar, was shown bringing her tray-fuls of rich, high calorie foods.
At one point, Penny Saeger’s sister spoke about this — and quite briefly.
Penny’s sister commented to the effect that Edgar brings his wife what she wants — or there will be “trouble” otherwise. Then the brief segment ended.

Penny (above image) underwent the surgery and was not losing weight despite being in the hospital.
The surgeon, Dr. Younan Nowzaradan, believed someone was sneaking her food, though this was not confirmed.
She was sent home, which was actually an apartment that Edgar had found nearby the hospital.
From the apartment, Penny was expected to stick to a low calorie diet and attend doctor appointments.
Instead, the cameras followed Edgar preparing huge amounts of junk food and bringing them to Penny, who was as bedbound as ever.
The cameras did not show Penny demanding Edgar bring her the food. The show simply followed him serving her, and her gorging.
The question all viewers have of “My 600 Pound Life” is what is going ON with Edgar and all the other enabling spouses?
They do not care about one more box of donuts being handed to the bed- or chair-bound 600+ pound family member.
In nearly every episode of “My 600 Pound Life,” the subject lives with at least one enabler.

They never live alone — except maybe for one or two over the many seasons of the show.
That’s because if they did, there’d be no enabler to help them become bed- or chair-bound.
- Viewers would like to know what the enablers are afraid of.
- Viewers wonder if there’s more to the dynamic than, “I bring her food because it makes her happy.”
How much power can a bedridden person have?
A bedridden person can wield a LOT of power to the enabler who has severe psychological issues.
Childhood Roots
Anyone who saw Penny on “My 600 Pound Life” can easily figure out why she was so afraid to commit to lifestyle changes to lose weight.
The tragedy is rooted in Penny’s childhood. Briefly touched upon was abuse at the hands of her father.
Penny’s parents were not mentioned in the present. We can easily imagine that her father made her believe she’d fail at anything she’d try.
So maybe the idea of trying to walk with the help of a physical therapist, post-surgery, was too frightening, which is why after four months, she couldn’t even take a few steps.
And the idea of sticking to a diet so that she could live long enough to see her son enter middle school was just too daunting.
Why Won’t TLC Explore the Enabling Dynamic?
Sometimes the enabler is asked point-blank by Dr. Now why they bring so much food to the sufferer.
There are three basic responses:
- I hate to see her hungry.
- It makes him happy.
- There’ll be hell to pay if I don’t.
And then the probing stops there. Viewers are left thinking, “WHAT…?!
Perhaps the probing indeed gets carried out, but the footage gets cut — but if that’s the case…then why has it been getting cut for all but a few episodes?
Much episode footage involves moving preparations to Houston, surgical prep and the actual surgery.
Thus, there is plenty of air time to explore the enabler dynamic. Certainly, viewers would rather see this investigated than watch people packing boxes for the move or endoscopic images of someone’s gut.
This is one reality TV show that can’t be faked, save for perhaps what seem to be some pre-orchestrated argument scenes among family members and the overly scripted “I’m afraid the doctor will turn me away.”
Each episode of “My 600 Pound Life” is now two hours. For sure, there is plenty of time to delve into the mysteries of what makes the enabler’s mind tick.
Lorra Garrick is a former personal trainer certified by the American Council on Exercise. At Bally Total Fitness she trained clients of all ages for fat loss, muscle building, fitness and improved health.

Microscopic Colitis Exercise Guidelines by GI Doctor

Exercise will NOT make microscopic colitis worse.
So don’t use microscopic colitis as an excuse to avoid working out at a gym, even if you’re having diarrhea 20 times a day.
“Generally speaking, exercise is good for the body,” begins Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“It can improve specific conditions, such as microscopic colitis, and your general health.”
If urgency is a problem, then you should try to configure your workout routine close to the gym’s restroom, whenever possible.
Dr. Fine’s Recommendations for Exercising with Microscopic Colitis
Consider yoga. Yoga exercises can aid in the digestion process.
Certain yoga poses may help people with microscopic colitis or other gastrointestinal (GI) conditions.
A few poses I recommend include flowing bridge pose, Marichi’s pose and revolved triangle pose (below).
If you aren’t sure how to get started, there are many websites, books and classes that may help you learn about yoga.
Establishing a regular exercise routine is essential for maintaining long-term fitness and health.
By incorporating exercise into your daily schedule, you form a habit that increases your likelihood of sticking with it.
To support this habit, start with a basic routine that you can gradually build upon.
Stretching before and after your workouts is crucial for relieving muscle tension and reducing the risk of injury.
If you have gastrointestinal conditions like microscopic colitis, pay special attention to exercises targeting muscle groups near the GI tract.
Kegel and pelvic floor exercises can be particularly beneficial in this regard.
Incorporate both core strengthening and cardiovascular exercises into your routine.
Cardiovascular workouts are excellent for managing weight, which can ease joint stress and mitigate the risks associated with diabetes, heart disease, and various GI conditions.
Strengthening your core supports overall stability and can improve posture and balance.

Freepik.com/yanalya
Exercising with a friend can make your workouts more enjoyable and provide motivation.
Having a workout buddy can also help you stay accountable to your fitness goals.
Finally, always seek recommendations from your doctor to ensure that your exercise routine is safe and effective for your individual needs.
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.
Top image: Freepik.com

Can Microscopic Colitis Diarrhea Cause Nutrient Loss?

Do you ever wonder if all the good things you eat are being passed out of your system by your microscopic colitis?
Does this disease make healthy food come out withthe diarrhea?
Let’s say a person eats a lot of fruits and vegetables whole, and/or juices them.
Shortly after they have the classic porridge-like or watery diarrhea the color of the consumed produce (greenish for spinach, reddish for beets, plus visible particles of produce floating in the toilet water).
Does this indicate that a significant amount of nutrients went right through the person?
“Yes, when the body expels waste, nutrients are also expelled,” says Jeffrey Fine, MD, chief of gastroenterology at the Medical Surgical Clinic of Irving.
“That’s one of the reasons it’s so important to stay hydrated. I recommend drinking an ounce of filtered water, per kilogram per day.”
What would you tell a patient who’s concerned about wasting produce because it appears that much of it comes out in their diarrhea?
Assume this individual has only microscopic colitis—no other GI diseases or other medical conditions.
But they’re concerned that all that juicing or whole-fruit consumption—which they do for the nutrient density—is being wasted.
“What you’re describing is rapid transit and possible malabsorption,” says Dr. Fine.
“The patient should see a gastroenterologist for evaluation. The gastroenterologist can recommend treatment options, including diet changes.
“What he/she recommends depends on what is causing the rapid transit, but usually in situations like this, I recommend chicken and rice soup, and nutritional supplements with predigested sugar components.
“Also, avoid juices and raw vegetables while the diarrhea is occurring and take a multivitamin with minerals.”
That may be a tough pill to swallow for those with microscopic colitis who strive to get a lot of antioxidants and enzymes (abundant in fruits and vegetables) in their daily diet.
But if a significant amount of these nutrients is going to end up getting expelled through your other end, you may as well avoid these foods so that the flare-up of microscopic colitis has a chance to recede.
After all, it’s no secret that fruits and vegetables can bring the diarrhea into the spotlight.
Dr. Fine has been in practice for over 30 years and specializes in digestive health, integrative medicine and food sensitivities.
Lorra Garrick has been covering medical, fitness and cybersecurity topics for many years, having written thousands of articles for print magazines and websites, including as a ghostwriter. She’s also a former ACE-certified personal trainer.
.


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}